Anda mungkin juga menyukai
- PK Design Doses PDFDokumen7 halamanPK Design Doses PDFJuan CarBelum ada peringkat
- Dose and IntervalDokumen37 halamanDose and IntervalRosel Ann BontiaBelum ada peringkat
- SK Suraj, Biopharmaceutices & Pharmacokinetices, Roll No - 38301921059, 3RD Year 6TH Sem..ca2-1Dokumen9 halamanSK Suraj, Biopharmaceutices & Pharmacokinetices, Roll No - 38301921059, 3RD Year 6TH Sem..ca2-1Sk SurajBelum ada peringkat
- 2 Design of DOSAGE DESIGNDokumen16 halaman2 Design of DOSAGE DESIGNMarjo100% (1)
- Lesson 3 Dosing SchedulingDokumen20 halamanLesson 3 Dosing SchedulingAngelica GomezBelum ada peringkat
- Therapeutic Drug MonitoringDokumen6 halamanTherapeutic Drug MonitoringEdi Uchiha SutarmantoBelum ada peringkat
- I Am Sharing 'Pharmacokinetics' With YouDokumen12 halamanI Am Sharing 'Pharmacokinetics' With Youizhar ul haqBelum ada peringkat
- May 4, 2010 Class: Surgery: Basic Clinical Pharmacokinetics SummaryDokumen4 halamanMay 4, 2010 Class: Surgery: Basic Clinical Pharmacokinetics SummaryShoaib BiradarBelum ada peringkat
- Population PharmacokineticsDokumen37 halamanPopulation Pharmacokineticsyuppie_raj2175Belum ada peringkat
- 01 BiopharmaceuticsDokumen69 halaman01 BiopharmaceuticsRiczen Mae F. Vila100% (1)
- Therapeutic Drug Monitoring Part 2 PDFDokumen23 halamanTherapeutic Drug Monitoring Part 2 PDFChandra AvicennaBelum ada peringkat
- PKVPD Clinical PharmaDokumen8 halamanPKVPD Clinical Pharmadanilo cordobaBelum ada peringkat
- Therapeutic Drug MonitoringDokumen50 halamanTherapeutic Drug MonitoringKapusetti Vanaja0% (1)
- Therapeutic Drug Monitoring: RVS Chaitanya KoppalaDokumen33 halamanTherapeutic Drug Monitoring: RVS Chaitanya KoppalaDr. Raghavendra Kumar GundaBelum ada peringkat
- Lec. 2 Selected TopicsDokumen22 halamanLec. 2 Selected TopicsMustafa KamelBelum ada peringkat
- st03 PDFDokumen8 halamanst03 PDFLutfi HidiyaningtyasBelum ada peringkat
- Estimation of Cefuroxime Dosage Using Pharmacodynamic Targets, MIC DistributionsDokumen13 halamanEstimation of Cefuroxime Dosage Using Pharmacodynamic Targets, MIC DistributionsLuciana OliveiraBelum ada peringkat
- Individualizing Propofol Dosage: A Multivariate Linear Model ApproachDokumen12 halamanIndividualizing Propofol Dosage: A Multivariate Linear Model ApproachFranklinBelum ada peringkat
- MDR SHDokumen58 halamanMDR SHsmithalexBelum ada peringkat
- ACTD Rev.1 Part IV Clinical DocumentDokumen50 halamanACTD Rev.1 Part IV Clinical DocumentRaeanne SabadoBelum ada peringkat
- Therapeutic Drug Monitoring-FinalDokumen49 halamanTherapeutic Drug Monitoring-FinalSaiesh PhaldesaiBelum ada peringkat
- Use Pharmaceutical Calculation Techniques and TerminologiesDokumen62 halamanUse Pharmaceutical Calculation Techniques and TerminologiesKena Samuel100% (3)
- Pharmaco KineticsDokumen46 halamanPharmaco Kineticssakumar5678Belum ada peringkat
- 1-Lecture One IntroductionDokumen45 halaman1-Lecture One IntroductionKerolus Joseph AminBelum ada peringkat
- Clinical Pharmacokinetics Sample ChapterDokumen44 halamanClinical Pharmacokinetics Sample Chapterpinkbutter100% (1)
- Standardization of Pharmacokinetic/pharmacodynamic (PK/PD) Terminology For Anti-Infective DrugsDokumen4 halamanStandardization of Pharmacokinetic/pharmacodynamic (PK/PD) Terminology For Anti-Infective DrugsManMan AR-llBelum ada peringkat
- TDM Basic PrinciplesDokumen10 halamanTDM Basic PrinciplesabinchandrakumarBelum ada peringkat
- Biopharmaceutics & pharmacokinetics-II AssignmentDokumen7 halamanBiopharmaceutics & pharmacokinetics-II AssignmentRA TanvirBelum ada peringkat
- Bension Mirzakan - IPPE Assignment 1.13Dokumen4 halamanBension Mirzakan - IPPE Assignment 1.13bmirzakanBelum ada peringkat
- Applied Biopharmaceutics & PharmacokineticsDokumen28 halamanApplied Biopharmaceutics & PharmacokineticsFirman Syarifudin Saputra100% (1)
- 01 IntroductionDokumen45 halaman01 IntroductionTulin QadriBelum ada peringkat
- ACTD PartIVClinical Nov05Dokumen50 halamanACTD PartIVClinical Nov05TueBelum ada peringkat
- Pharmacokinetic & Pharmacodynamic (PK and PD) Models of Controlled Release SystemDokumen23 halamanPharmacokinetic & Pharmacodynamic (PK and PD) Models of Controlled Release Systemdeep22123Belum ada peringkat
- 2018 - Workshop EAHP - Therapeutic Drug Monitoring - Thuerig - DefDokumen55 halaman2018 - Workshop EAHP - Therapeutic Drug Monitoring - Thuerig - DefMickelson Joseph VilBelum ada peringkat
- Clinical Pharmacokinetics Equations and Calculations IIDokumen7 halamanClinical Pharmacokinetics Equations and Calculations IILama SaudBelum ada peringkat
- Clinical PharmacokineticsDokumen1.135 halamanClinical PharmacokineticstayhodgesBelum ada peringkat
- Prepared By: Murari Pavan M.Pharm (Pharmaceutics) Gautham College of PharmacyDokumen22 halamanPrepared By: Murari Pavan M.Pharm (Pharmaceutics) Gautham College of PharmacyAshutosh LohumiBelum ada peringkat
- Jay Raja: Mr. Ashish KyadaDokumen36 halamanJay Raja: Mr. Ashish Kyadajvraja80100% (2)
- Chapter - 7 Therapeutic Drug Monitoring - Concepts, Methodology, Clinical Applications and LimitationsDokumen5 halamanChapter - 7 Therapeutic Drug Monitoring - Concepts, Methodology, Clinical Applications and LimitationsTasmih Rob MowBelum ada peringkat
- Concepts in Clinical Pharmacokinetics - 4th Ed. 2005Dokumen298 halamanConcepts in Clinical Pharmacokinetics - 4th Ed. 2005mohanjaga793100% (3)
- Anticancer Dose Adjustment For Patients With Renal and Hepatic Dysfunction: From Scientific Evidence To Clinical ApplicationDokumen16 halamanAnticancer Dose Adjustment For Patients With Renal and Hepatic Dysfunction: From Scientific Evidence To Clinical ApplicationRiz Qie NaBelum ada peringkat
- 2 Determination of Dose and Dosing IntervalDokumen36 halaman2 Determination of Dose and Dosing IntervalSreya Sanil100% (1)
- 07 Dosage RegimenDokumen44 halaman07 Dosage Regimenzetttttttttt100% (3)
- AssignmentDokumen3 halamanAssignmentZeeshan NazarBelum ada peringkat
- A Peak at PKDokumen9 halamanA Peak at PKErik Ahmad HasyimBelum ada peringkat
- Pharmacokinetics and PharmacodynamicsDokumen12 halamanPharmacokinetics and PharmacodynamicsDrVinod Kumar Goud VemulaBelum ada peringkat
- Drug Dosing Renal Failure PDFDokumen41 halamanDrug Dosing Renal Failure PDFWildan Wisnu WardayaBelum ada peringkat
- TDM ClassDokumen26 halamanTDM Classsayan mandalBelum ada peringkat
- Cerminara Et Al 2017 A Single Center Retrospective Analysis of A Protocol For High Dose Methotrexate and LeucovorinDokumen9 halamanCerminara Et Al 2017 A Single Center Retrospective Analysis of A Protocol For High Dose Methotrexate and Leucovorinanton.neonatusBelum ada peringkat
- Population Pharmacokinetics IDokumen5 halamanPopulation Pharmacokinetics IJosé David Sanabria VanegasBelum ada peringkat
- Essential Pharmacokinetics: A Primer for Pharmaceutical ScientistsDari EverandEssential Pharmacokinetics: A Primer for Pharmaceutical ScientistsPenilaian: 5 dari 5 bintang5/5 (1)
- Physicochemical and Biomimetic Properties in Drug Discovery: Chromatographic Techniques for Lead OptimizationDari EverandPhysicochemical and Biomimetic Properties in Drug Discovery: Chromatographic Techniques for Lead OptimizationBelum ada peringkat
- Analytical Chemistry for Assessing Medication AdherenceDari EverandAnalytical Chemistry for Assessing Medication AdherenceBelum ada peringkat
- Pharmacoepidemiology, Pharmacoeconomics,PharmacovigilanceDari EverandPharmacoepidemiology, Pharmacoeconomics,PharmacovigilancePenilaian: 3 dari 5 bintang3/5 (1)
- Therapeutic Drug Monitoring: Newer Drugs and BiomarkersDari EverandTherapeutic Drug Monitoring: Newer Drugs and BiomarkersPenilaian: 2.5 dari 5 bintang2.5/5 (2)
- Clinical Challenges in Therapeutic Drug Monitoring: Special Populations, Physiological Conditions and PharmacogenomicsDari EverandClinical Challenges in Therapeutic Drug Monitoring: Special Populations, Physiological Conditions and PharmacogenomicsBelum ada peringkat
- Pharmaceutics: Basic Principles and Application to Pharmacy PracticeDari EverandPharmaceutics: Basic Principles and Application to Pharmacy PracticeAlekha DashBelum ada peringkat
- Renal Pharmacotherapy: Dosage Adjustment of Medications Eliminated by the KidneysDari EverandRenal Pharmacotherapy: Dosage Adjustment of Medications Eliminated by the KidneysBelum ada peringkat
- Flow Cytometry in Hematopathology: A Visual Approach to Data Analysis and InterpretationDari EverandFlow Cytometry in Hematopathology: A Visual Approach to Data Analysis and InterpretationBelum ada peringkat
- Development of Pharmacy Service Weights in the Implementation of Casemix System for Provider Payment: Concept, Methods and ApplicationsDari EverandDevelopment of Pharmacy Service Weights in the Implementation of Casemix System for Provider Payment: Concept, Methods and ApplicationsBelum ada peringkat
- PCI B Pharm Syllabus PDFDokumen189 halamanPCI B Pharm Syllabus PDFDrGajanan Vaishnav100% (1)
- Partially Miscible LiquidsDokumen16 halamanPartially Miscible LiquidsYuppie Raj86% (7)
- Solubility of Liquids in LiquidsDokumen12 halamanSolubility of Liquids in LiquidsYuppie RajBelum ada peringkat
- Posology Notes Yuppie's GaloreDokumen6 halamanPosology Notes Yuppie's GaloreYuppie RajBelum ada peringkat
- Solubility of Liquids in LiquidsDokumen33 halamanSolubility of Liquids in LiquidsYuppie Raj67% (3)
- Quantitative Approach To Factors Affecting Solubility of DrugsDokumen18 halamanQuantitative Approach To Factors Affecting Solubility of DrugsYuppie Raj100% (3)
- Diffusion Principles in Biological SystemsDokumen18 halamanDiffusion Principles in Biological SystemsYuppie Raj100% (2)
- Analysis and Design of Pharmacokinetic ModelsDokumen77 halamanAnalysis and Design of Pharmacokinetic ModelsYuppie RajBelum ada peringkat
- Ideal Solubility ParametersDokumen14 halamanIdeal Solubility ParametersYuppie Raj100% (2)
- Solvation, Association and DissociationDokumen14 halamanSolvation, Association and DissociationYuppie RajBelum ada peringkat
- Ideal Solubility ParametersDokumen14 halamanIdeal Solubility ParametersYuppie Raj100% (2)
- Solute Solvent Interactions PPI BPII - IDokumen32 halamanSolute Solvent Interactions PPI BPII - IYuppie Raj100% (2)
- Solubility ExpressionsDokumen7 halamanSolubility ExpressionsYuppie Raj100% (1)
- Solubility Notes Summary Physical Pharmacy PharmaceuticsDokumen9 halamanSolubility Notes Summary Physical Pharmacy PharmaceuticsYuppie RajBelum ada peringkat
- DEGRADATIONPATHWAY B. Pharm 2-2Dokumen22 halamanDEGRADATIONPATHWAY B. Pharm 2-2Yuppie RajBelum ada peringkat
- Revised BiopharmaceuticsDokumen34 halamanRevised BiopharmaceuticsYuppie RajBelum ada peringkat
- Multiple-Dosing Regimens (Repetitive Dosing)Dokumen4 halamanMultiple-Dosing Regimens (Repetitive Dosing)Yuppie RajBelum ada peringkat
- Drug Dosing in Obese Patients: A Dilemma: International Journal of Advances in PharmaceuticsDokumen7 halamanDrug Dosing in Obese Patients: A Dilemma: International Journal of Advances in PharmaceuticsYuppie RajBelum ada peringkat
- Laboratory Manual: Prepared byDokumen14 halamanLaboratory Manual: Prepared byYuppie Raj100% (1)
- Panda2020 Article FormulationAndDevelopmentOfFlo PDFDokumen9 halamanPanda2020 Article FormulationAndDevelopmentOfFlo PDFYuppie RajBelum ada peringkat
- Rajasekhar SirDokumen1 halamanRajasekhar SirYuppie RajBelum ada peringkat
- MethocelDokumen5 halamanMethocelYuppie RajBelum ada peringkat
- Laboratory Manual: Prepared byDokumen34 halamanLaboratory Manual: Prepared byYuppie RajBelum ada peringkat
- Design of Dosage Regimens:: 1. Introduction To Clinical PharmacokineticsDokumen1 halamanDesign of Dosage Regimens:: 1. Introduction To Clinical PharmacokineticsYuppie RajBelum ada peringkat
- Rajasekhar Sir LORDokumen1 halamanRajasekhar Sir LORYuppie RajBelum ada peringkat
- Dnyaneshwari: The Philosophical PartDokumen6 halamanDnyaneshwari: The Philosophical PartGargaBelum ada peringkat
- Nursing MGT For StrokeDokumen7 halamanNursing MGT For StrokeRubijen NapolesBelum ada peringkat
- Adarsh Patil: Personal DetailsDokumen4 halamanAdarsh Patil: Personal DetailsAdarsh PatilBelum ada peringkat
- Daily Lesson Plan in Grade 10 MathematicsDokumen6 halamanDaily Lesson Plan in Grade 10 MathematicsRandy Asilum AlipaoBelum ada peringkat
- Designing Type A and Type B Syllabuses - Advantages and DisadvantagesDokumen12 halamanDesigning Type A and Type B Syllabuses - Advantages and Disadvantagesjamel_terzi_alimi100% (7)
- History of Health EducationDokumen6 halamanHistory of Health EducationCorrine Ivy100% (2)
- A3 Book Club Freewrite Lesson PlanDokumen3 halamanA3 Book Club Freewrite Lesson Planapi-250493968Belum ada peringkat
- Competence-Based Learning Materials: Sector: TourismDokumen68 halamanCompetence-Based Learning Materials: Sector: TourismAnalizaViloriaBelum ada peringkat
- Health EducationDokumen2 halamanHealth EducationRhea Cherl Ragsag IIBelum ada peringkat
- An Assignment On Checklist: Submitted To:-Submitted By: - Divya MSC NSG 1 YearDokumen4 halamanAn Assignment On Checklist: Submitted To:-Submitted By: - Divya MSC NSG 1 YearNehaBelum ada peringkat
- John TrussDokumen7 halamanJohn Trussrobinson robertsBelum ada peringkat
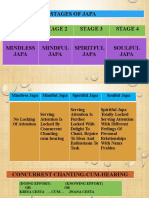
- SOULFUL JAPA - Bliss Unlimited by Japa YagnaDokumen28 halamanSOULFUL JAPA - Bliss Unlimited by Japa Yagnabalaganesh spk100% (1)
- Literature ReviewDokumen6 halamanLiterature Reviewapi-609322356Belum ada peringkat
- Arthur Douglas (Doug) Ayars Jr. ApplicationDokumen9 halamanArthur Douglas (Doug) Ayars Jr. ApplicationThe Florida Times-UnionBelum ada peringkat
- The Abington Journal 02-01-2012Dokumen20 halamanThe Abington Journal 02-01-2012The Times LeaderBelum ada peringkat
- Narrative ReportDokumen23 halamanNarrative Reportmark batacBelum ada peringkat
- Learning Process: CS/CMPE 537 - Neural NetworksDokumen34 halamanLearning Process: CS/CMPE 537 - Neural Networkskunalbhatia15Belum ada peringkat
- HS 2nd Yr Assamese Syllabus 2016Dokumen1 halamanHS 2nd Yr Assamese Syllabus 2016Principal Universal AcademyBelum ada peringkat
- Teaching Film123Dokumen2 halamanTeaching Film123Can YesilBelum ada peringkat
- Ge09 Memory Test #9 Mojica, Adrienne B.Dokumen4 halamanGe09 Memory Test #9 Mojica, Adrienne B.Adrienne Dave Mojica100% (1)
- Postman Collate 270321Dokumen138 halamanPostman Collate 270321TiniBelum ada peringkat
- Department of Civil Engineering College of Engineering University of SulaimaniDokumen233 halamanDepartment of Civil Engineering College of Engineering University of SulaimaniAhmad PshtiwanBelum ada peringkat
- Unit Outline: School of Biomedical Biomolecular and Chemical SciencesDokumen4 halamanUnit Outline: School of Biomedical Biomolecular and Chemical SciencesEvilasio CostaBelum ada peringkat
- The Parable of The Rainbow ColorsDokumen17 halamanThe Parable of The Rainbow Colorskristine remolloBelum ada peringkat
- Lacrosse Unit Plan Educ530 Oct31Dokumen13 halamanLacrosse Unit Plan Educ530 Oct31api-390594147Belum ada peringkat
- Case Study - 23: Personal Relations Vs Ethical ValuesDokumen3 halamanCase Study - 23: Personal Relations Vs Ethical ValuesPratik BajajBelum ada peringkat
- Key Point Slides - Ch5Dokumen21 halamanKey Point Slides - Ch5Nuzul DwiBelum ada peringkat
- Action Plan in MathDokumen4 halamanAction Plan in MathRoselyn Catubig Vidad Jumadla100% (4)
- Programme Handbook 21-22 FinalDokumen27 halamanProgramme Handbook 21-22 Final4wqzcq7p9xBelum ada peringkat
- Linguistic FunctionsDokumen42 halamanLinguistic FunctionsRussel John CalloBelum ada peringkat