Anda mungkin juga menyukai
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- A Review of Disrupted-in-Schizophrenia-1 (Disc1) : Neurodevelopment, Cognition, and Mental ConditionsDokumen9 halamanA Review of Disrupted-in-Schizophrenia-1 (Disc1) : Neurodevelopment, Cognition, and Mental Conditionsrocambolescas perthBelum ada peringkat
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Basch 2004Dokumen15 halamanBasch 2004rocambolescas perthBelum ada peringkat
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- Disrupted in Schizophrenia 1: Building Brains and Memories: David J Porteous and J Kirsty MillarDokumen7 halamanDisrupted in Schizophrenia 1: Building Brains and Memories: David J Porteous and J Kirsty Millarrocambolescas perthBelum ada peringkat
- Evidence For An Expansion-Based Temporal SHH Gradient in Specifying Vertebrate Digit IdentitiesDokumen12 halamanEvidence For An Expansion-Based Temporal SHH Gradient in Specifying Vertebrate Digit Identitiesrocambolescas perthBelum ada peringkat
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (400)
- Glycinergic Transmission: Glycine Transporter Glyt2 in Neuronal PathologiesDokumen10 halamanGlycinergic Transmission: Glycine Transporter Glyt2 in Neuronal Pathologiesrocambolescas perthBelum ada peringkat
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- Pittenger 2007Dokumen22 halamanPittenger 2007rocambolescas perthBelum ada peringkat
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- 2,2 - Thiodiethanol: A New Water Soluble Mounting Medium For High Resolution Optical MicrosDokumen9 halaman2,2 - Thiodiethanol: A New Water Soluble Mounting Medium For High Resolution Optical Microsrocambolescas perthBelum ada peringkat
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Cellular Mechanisms of Cerebellar LTD: Hervé Daniel, Carole Levenes and Francis CrépelDokumen7 halamanCellular Mechanisms of Cerebellar LTD: Hervé Daniel, Carole Levenes and Francis Crépelrocambolescas perthBelum ada peringkat
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- API Boarding Pass: Ankara Esenboga - MunichDokumen6 halamanAPI Boarding Pass: Ankara Esenboga - Munichrocambolescas perthBelum ada peringkat
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Note On Burden and Standard of Proof in Refugee ClaimsDokumen7 halamanNote On Burden and Standard of Proof in Refugee Claimsrocambolescas perthBelum ada peringkat
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Molecular Mechanisms of Neuronal Migration Disorders, Quo Vadis?Dokumen12 halamanMolecular Mechanisms of Neuronal Migration Disorders, Quo Vadis?rocambolescas perthBelum ada peringkat
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- FullDokumen8 halamanFullrocambolescas perthBelum ada peringkat
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- Synaptic Actin Dysregulation, A Convergent Mechanism of Mental Disorders?Dokumen7 halamanSynaptic Actin Dysregulation, A Convergent Mechanism of Mental Disorders?rocambolescas perthBelum ada peringkat
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (74)
- Review Polarity Proteins in Axon Specification and SynaptogenesisDokumen14 halamanReview Polarity Proteins in Axon Specification and Synaptogenesisrocambolescas perthBelum ada peringkat
- Neural Circuits Underlying The Pathophysiology of Mood DisordersDokumen11 halamanNeural Circuits Underlying The Pathophysiology of Mood Disordersrocambolescas perthBelum ada peringkat
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- PTEN: From Pathology To Biology: Maria Luisa Sulis and Ramon ParsonsDokumen6 halamanPTEN: From Pathology To Biology: Maria Luisa Sulis and Ramon Parsonsrocambolescas perthBelum ada peringkat
- 1 s2.0 S0012160604004233 Main PDFDokumen10 halaman1 s2.0 S0012160604004233 Main PDFrocambolescas perthBelum ada peringkat
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- Review Miniaturization of Nervous Systems and NeuronsDokumen7 halamanReview Miniaturization of Nervous Systems and Neuronsrocambolescas perthBelum ada peringkat
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (345)
- Review: Evolution of Vertebrates As Viewed From The CrestDokumen9 halamanReview: Evolution of Vertebrates As Viewed From The Crestrocambolescas perthBelum ada peringkat
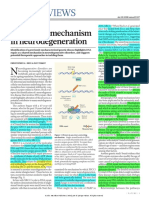
- News & Views: A Unifying Mechanism in NeurodegenerationDokumen2 halamanNews & Views: A Unifying Mechanism in Neurodegenerationrocambolescas perthBelum ada peringkat
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- Ptenless Means More: Bangyan Stiles, Matthias Groszer, Shunyou Wang, Jing Jiao, Hong WuDokumen10 halamanPtenless Means More: Bangyan Stiles, Matthias Groszer, Shunyou Wang, Jing Jiao, Hong Wurocambolescas perthBelum ada peringkat
- Toolkit Template a.D.D.I.E. ModelDokumen3 halamanToolkit Template a.D.D.I.E. ModelDiego Granda100% (1)
- Block1 504Dokumen87 halamanBlock1 504Maharghya BiswasBelum ada peringkat
- Lecture DisscusionDokumen1 halamanLecture Disscusionapi-313409388Belum ada peringkat
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- Behavioral Analysis: Mary Anne A. Portuguez, MP, RPMDokumen20 halamanBehavioral Analysis: Mary Anne A. Portuguez, MP, RPMDivine Grace LattaoBelum ada peringkat
- A. Summary of What Infants and Toddlers Can Do Cognitively: 0-6 Months 7-12 MonthsDokumen40 halamanA. Summary of What Infants and Toddlers Can Do Cognitively: 0-6 Months 7-12 MonthsJohann Emmanuel MolatoBelum ada peringkat
- Introduction To Artificial Intelligence: Aiza Shabir Lecturer Institute of CS&IT The Women University MultanDokumen25 halamanIntroduction To Artificial Intelligence: Aiza Shabir Lecturer Institute of CS&IT The Women University MultanShah JeeBelum ada peringkat
- Lesson Plan 3 - Five Fram AdditionDokumen4 halamanLesson Plan 3 - Five Fram Additionapi-267744702Belum ada peringkat
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- Agree or DisagreeDokumen2 halamanAgree or DisagreeHanBelum ada peringkat
- ODLDokumen6 halamanODLSharifah Aini Syed IdrusBelum ada peringkat
- Entrepreneurial Mindset and Thinking SkillsDokumen54 halamanEntrepreneurial Mindset and Thinking SkillsRomen CenizaBelum ada peringkat
- Expressive AphasiaDokumen2 halamanExpressive AphasiavishwanathBelum ada peringkat
- What Is Differentiated InstructionDokumen5 halamanWhat Is Differentiated InstructionMK MendozaBelum ada peringkat
- A Neuroscientist Reveals How To Think DifferentlyDokumen6 halamanA Neuroscientist Reveals How To Think DifferentlyNizam UddinBelum ada peringkat
- Brain Plasticity - How Experience Changes The BrainDokumen5 halamanBrain Plasticity - How Experience Changes The BrainWilson OTOBelum ada peringkat
- Cunha Et Al., 2019 - Art 2Dokumen9 halamanCunha Et Al., 2019 - Art 2Erika SierraBelum ada peringkat
- Neuropsychological Rehabilitation, Neuroimaging and Neuropasticity A Clinical CommentaryDokumen11 halamanNeuropsychological Rehabilitation, Neuroimaging and Neuropasticity A Clinical CommentaryRossana Maciel Taboada GarzónBelum ada peringkat
- Student ID BC170202121: Task 1: Identify at Least Ten (10) Bad Habits Within You, Which Hinder Your Listening AbilityDokumen3 halamanStudent ID BC170202121: Task 1: Identify at Least Ten (10) Bad Habits Within You, Which Hinder Your Listening AbilitySaddam HussianBelum ada peringkat
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- Physical and Cognitive DevelopmentDokumen2 halamanPhysical and Cognitive DevelopmentalyBelum ada peringkat
- Map & Tree Map.: Figure 1: Circle Map (Sources Maps - HTML)Dokumen8 halamanMap & Tree Map.: Figure 1: Circle Map (Sources Maps - HTML)Hus HusainiBelum ada peringkat
- Exercise 1Dokumen2 halamanExercise 1danilo miguelBelum ada peringkat
- Language Skills: Reading Writing Speaking ListeningDokumen18 halamanLanguage Skills: Reading Writing Speaking ListeningAbdul Bambang SyukurBelum ada peringkat
- Lecture 1 - Intro History MethodsDokumen77 halamanLecture 1 - Intro History MethodsHenok FikaduBelum ada peringkat
- Learn10 - Ways 1472563RDokumen5 halamanLearn10 - Ways 1472563RricardoBelum ada peringkat
- Can Be Encoded or Handwritten.)Dokumen2 halamanCan Be Encoded or Handwritten.)Jhon Paul AlteroBelum ada peringkat
- Cain Et Al. 2004 - Childrens Reading Comprehension Ability Concurrent Prediction by Working Memory, Verbal Ability, and Component SkillsDokumen12 halamanCain Et Al. 2004 - Childrens Reading Comprehension Ability Concurrent Prediction by Working Memory, Verbal Ability, and Component SkillsDespina KalaitzidouBelum ada peringkat
- Technology in Constructivist Learning EnvironmentDokumen26 halamanTechnology in Constructivist Learning EnvironmentAbegail Ebio TodioBelum ada peringkat
- Test I. True or False. Write TRUE If The Statement Is Correct and FALSE If The Statement Is IncorrectDokumen2 halamanTest I. True or False. Write TRUE If The Statement Is Correct and FALSE If The Statement Is IncorrectMariecris Barayuga Duldulao-AbelaBelum ada peringkat
- Group 1: Lê Thị Thủy Tuyên Phan Hoàng Bảo Trân Cao Nguyễn Đan ThyDokumen48 halamanGroup 1: Lê Thị Thủy Tuyên Phan Hoàng Bảo Trân Cao Nguyễn Đan ThyTuyenLeBelum ada peringkat
- Motivation As A Contributing Factor in Second Language AcquisitionDokumen6 halamanMotivation As A Contributing Factor in Second Language AcquisitionentjinrBelum ada peringkat
- Cognitive Control Therapy With Children and AdolescentsDokumen426 halamanCognitive Control Therapy With Children and AdolescentsDushyantha JayawardenaBelum ada peringkat
- Summary of The Body Keeps the Score: Brain, Mind, and Body in the Healing of Trauma by Bessel van der Kolk MDDari EverandSummary of The Body Keeps the Score: Brain, Mind, and Body in the Healing of Trauma by Bessel van der Kolk MDPenilaian: 4.5 dari 5 bintang4.5/5 (167)
- EVERYTHING/NOTHING/SOMEONE: A MemoirDari EverandEVERYTHING/NOTHING/SOMEONE: A MemoirPenilaian: 4.5 dari 5 bintang4.5/5 (49)
- Critical Thinking: How to Effectively Reason, Understand Irrationality, and Make Better DecisionsDari EverandCritical Thinking: How to Effectively Reason, Understand Irrationality, and Make Better DecisionsPenilaian: 4.5 dari 5 bintang4.5/5 (39)
- The Upward Spiral: Using Neuroscience to Reverse the Course of Depression, One Small Change at a TimeDari EverandThe Upward Spiral: Using Neuroscience to Reverse the Course of Depression, One Small Change at a TimePenilaian: 4.5 dari 5 bintang4.5/5 (140)