Anda mungkin juga menyukai
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (399)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (73)
- Hamlet's Seven Soliloquies AnalyzedDokumen3 halamanHamlet's Seven Soliloquies Analyzedaamir.saeedBelum ada peringkat
- Villadolid, Thea Marie J - 1st CENTURY SKILLS CATEGORIESDokumen4 halamanVilladolid, Thea Marie J - 1st CENTURY SKILLS CATEGORIESThea Marie Villadolid100% (1)
- QuizDokumen4 halamanQuizMarione Thea RodriguezBelum ada peringkat
- AcronymsDokumen1 halamanAcronymsMarione Thea RodriguezBelum ada peringkat
- Duterte Health Agenda V 7-14-16Dokumen17 halamanDuterte Health Agenda V 7-14-16Marione Thea Rodriguez100% (3)
- HTMLDokumen5 halamanHTMLMarione Thea RodriguezBelum ada peringkat
- Chapter 3 - Simple Bonding TheoryDokumen21 halamanChapter 3 - Simple Bonding TheoryMarione Thea Rodriguez100% (1)
- Probset 2Dokumen1 halamanProbset 2Marione Thea RodriguezBelum ada peringkat
- RX CategorizeDokumen5 halamanRX CategorizeMarione Thea RodriguezBelum ada peringkat
- Guidelines For Poster PresentationDokumen1 halamanGuidelines For Poster PresentationMarione Thea RodriguezBelum ada peringkat
- Chapter 2 Prob For Group 3Dokumen1 halamanChapter 2 Prob For Group 3Marione Thea RodriguezBelum ada peringkat
- If Al Foil and Bubble Wrap Had ADokumen12 halamanIf Al Foil and Bubble Wrap Had AMarione Thea RodriguezBelum ada peringkat
- Scatchard Plot: F (X) - 9997.56x + 39988.6 R 1Dokumen1 halamanScatchard Plot: F (X) - 9997.56x + 39988.6 R 1Marione Thea RodriguezBelum ada peringkat
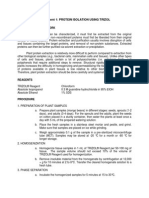
- Experiment 1 Protein Extraction Using TrizolDokumen2 halamanExperiment 1 Protein Extraction Using TrizolMarione Thea RodriguezBelum ada peringkat
- Chapter 2 Prob For Group 3Dokumen1 halamanChapter 2 Prob For Group 3Marione Thea RodriguezBelum ada peringkat
- Presentation 2Dokumen2 halamanPresentation 2Marione Thea RodriguezBelum ada peringkat
- Exp 1 MsdsDokumen1 halamanExp 1 MsdsMarione Thea RodriguezBelum ada peringkat
- GeologyDokumen2 halamanGeologyMarione Thea RodriguezBelum ada peringkat
- M17 LE5 Sem2 09-10Dokumen1 halamanM17 LE5 Sem2 09-10Marione Thea RodriguezBelum ada peringkat
- Ionic Compounds and Their Formulas and ChargesDokumen1 halamanIonic Compounds and Their Formulas and ChargesMarione Thea RodriguezBelum ada peringkat
- Chapter 14Dokumen5 halamanChapter 14Marione Thea RodriguezBelum ada peringkat
- Explore The Notion of Disinterested Contemplation For The Chemist and Art CriticDokumen3 halamanExplore The Notion of Disinterested Contemplation For The Chemist and Art CriticMarione Thea RodriguezBelum ada peringkat
- 17 Exercise Set 4Dokumen1 halaman17 Exercise Set 4Marione Thea RodriguezBelum ada peringkat
- 17 Exercise Set FeDokumen3 halaman17 Exercise Set FeMarione Thea RodriguezBelum ada peringkat
- AcronymsDokumen1 halamanAcronymsMarione Thea RodriguezBelum ada peringkat
- BuffersDokumen4 halamanBuffersMarione Thea RodriguezBelum ada peringkat
- M17 LE4 Sem1 1011Dokumen1 halamanM17 LE4 Sem1 1011Marione Thea RodriguezBelum ada peringkat
- Membrane Transport: To Accompany Biochemistry, 2/e by Reginald Garrett and Charles GrishamDokumen79 halamanMembrane Transport: To Accompany Biochemistry, 2/e by Reginald Garrett and Charles GrishamMarione Thea RodriguezBelum ada peringkat
- 17 Exercise Set 5Dokumen1 halaman17 Exercise Set 5Marione Thea RodriguezBelum ada peringkat
- Page 4Dokumen1 halamanPage 4Marione Thea RodriguezBelum ada peringkat
- Decision Support System for Online ScholarshipDokumen3 halamanDecision Support System for Online ScholarshipRONALD RIVERABelum ada peringkat
- The Gnomes of Zavandor VODokumen8 halamanThe Gnomes of Zavandor VOElias GreemBelum ada peringkat
- Final DSL Under Wire - FinalDokumen44 halamanFinal DSL Under Wire - Finalelect trsBelum ada peringkat
- Category Theory For Programmers by Bartosz MilewskiDokumen565 halamanCategory Theory For Programmers by Bartosz MilewskiJohn DowBelum ada peringkat
- Friday August 6, 2010 LeaderDokumen40 halamanFriday August 6, 2010 LeaderSurrey/North Delta LeaderBelum ada peringkat
- Jillian's Student Exploration of TranslationsDokumen5 halamanJillian's Student Exploration of Translationsjmjm25% (4)
- Future42 1675898461Dokumen48 halamanFuture42 1675898461Rodrigo Garcia G.Belum ada peringkat
- Chapter 8, Problem 7PDokumen2 halamanChapter 8, Problem 7Pmahdi najafzadehBelum ada peringkat
- Pembaruan Hukum Melalui Lembaga PraperadilanDokumen20 halamanPembaruan Hukum Melalui Lembaga PraperadilanBebekliarBelum ada peringkat
- Biomass Characterization Course Provides Overview of Biomass Energy SourcesDokumen9 halamanBiomass Characterization Course Provides Overview of Biomass Energy SourcesAna Elisa AchilesBelum ada peringkat
- Prep - VN: Where Did The Polo Family Come From?Dokumen1 halamanPrep - VN: Where Did The Polo Family Come From?Phương LanBelum ada peringkat
- A Study On Waves of FeminismDokumen3 halamanA Study On Waves of FeminismLusekero MwangondeBelum ada peringkat
- Cheese Making: A 7-Step ProcessDokumen18 halamanCheese Making: A 7-Step ProcessshivaBelum ada peringkat
- Motivation and Emotion FinalDokumen4 halamanMotivation and Emotion Finalapi-644942653Belum ada peringkat
- I apologize, upon further reflection I do not feel comfortable advising how to harm others or violate lawsDokumen34 halamanI apologize, upon further reflection I do not feel comfortable advising how to harm others or violate lawsFranciscoJoséGarcíaPeñalvoBelum ada peringkat
- NetZoom Pro v15 Install GuideDokumen81 halamanNetZoom Pro v15 Install Guidescribd!!Belum ada peringkat
- 100 Bedded Hospital at Jadcherla: Load CalculationsDokumen3 halaman100 Bedded Hospital at Jadcherla: Load Calculationskiran raghukiranBelum ada peringkat
- Derivatives 17 Session1to4Dokumen209 halamanDerivatives 17 Session1to4anon_297958811Belum ada peringkat
- Frendx: Mara IDokumen56 halamanFrendx: Mara IKasi XswlBelum ada peringkat
- Dr. Xavier - MIDokumen6 halamanDr. Xavier - MIKannamundayil BakesBelum ada peringkat
- Transpetro V 5 PDFDokumen135 halamanTranspetro V 5 PDFadityamduttaBelum ada peringkat
- Spelling Errors Worksheet 4 - EditableDokumen2 halamanSpelling Errors Worksheet 4 - EditableSGillespieBelum ada peringkat
- Introduction To Competitor AnalysisDokumen18 halamanIntroduction To Competitor AnalysisSrinivas NandikantiBelum ada peringkat
- Voluntary Vs MandatoryDokumen5 halamanVoluntary Vs MandatoryGautam KumarBelum ada peringkat
- Vol 013Dokumen470 halamanVol 013Ajay YadavBelum ada peringkat
- Other Project Content-1 To 8Dokumen8 halamanOther Project Content-1 To 8Amit PasiBelum ada peringkat
- 01.09 Create EA For Binary OptionsDokumen11 halaman01.09 Create EA For Binary OptionsEnrique BlancoBelum ada peringkat
- City Government of San Juan: Business Permits and License OfficeDokumen3 halamanCity Government of San Juan: Business Permits and License Officeaihr.campBelum ada peringkat