Anda mungkin juga menyukai
- Neurocognitive Disorder Diagnosis and TreatmentDokumen3 halamanNeurocognitive Disorder Diagnosis and TreatmentIT’S ME HAYLABelum ada peringkat
- 36 Applied NeuroscienceDokumen26 halaman36 Applied Neurosciencecercuri pătrate de fumBelum ada peringkat
- Neurology Board ReviewDokumen16 halamanNeurology Board ReviewNabeel Kouka, MD, DO, MBA, MPH67% (3)
- Autism Children-Dr. PurboyoDokumen22 halamanAutism Children-Dr. PurboyoAs MiniBelum ada peringkat
- Dementia 2Dokumen51 halamanDementia 2Arsal MushtaqBelum ada peringkat
- Amnesia DemensiaDokumen2 halamanAmnesia DemensiaAlexander TegarBelum ada peringkat
- Got Me Feelin Like A PsychoDokumen5 halamanGot Me Feelin Like A PsychoChan's RoomBelum ada peringkat
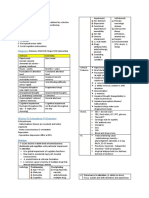
- Diagrams & Illustrations of Dementia Signs & SymptomsDokumen1 halamanDiagrams & Illustrations of Dementia Signs & Symptomsdysa ayu shalsabilaBelum ada peringkat
- Repaso Sx. MentalesDokumen5 halamanRepaso Sx. MentalesBreyner LassoBelum ada peringkat
- Activity 1. Comparison of Delirium and Dementia: Cognitive DisordersDokumen1 halamanActivity 1. Comparison of Delirium and Dementia: Cognitive DisordersDan Dan ManaoisBelum ada peringkat
- Dementia: Geriatrics Evaluation & ManagementDokumen2 halamanDementia: Geriatrics Evaluation & ManagementAngeles SlzrBelum ada peringkat
- DisabilitiesDokumen3 halamanDisabilitiesapi-644329047Belum ada peringkat
- Alzheimers DiseaseDokumen1 halamanAlzheimers DiseaseMartha Marty BalintBelum ada peringkat
- Case Analysis and Interventions Pyschopathology: Predisposing Factor Precipitating FactorDokumen1 halamanCase Analysis and Interventions Pyschopathology: Predisposing Factor Precipitating FactorSydelle GravadorBelum ada peringkat
- PsychiatryDokumen9 halamanPsychiatryDr .Boobalan VengateshBelum ada peringkat
- Feature Dementia Delirium Depression: Onset and DurationDokumen2 halamanFeature Dementia Delirium Depression: Onset and Durationwali mukadinmohamedBelum ada peringkat
- Dementia & DeliriumDokumen7 halamanDementia & DeliriumSudesna Roy ChowdhuryBelum ada peringkat
- PsychiatryDokumen18 halamanPsychiatryWorld MedclickzBelum ada peringkat
- Osmosis 4Dokumen1 halamanOsmosis 4dysa ayu shalsabilaBelum ada peringkat
- Components of Mental Status ExaminationDokumen5 halamanComponents of Mental Status ExaminationDesta FransiscaBelum ada peringkat
- Seminar DementiaDokumen63 halamanSeminar DementiaAhmad Syahmi YZBelum ada peringkat
- Trance: Ns. Mohamad Nur, S.Kep.,M.Si (Ked)Dokumen38 halamanTrance: Ns. Mohamad Nur, S.Kep.,M.Si (Ked)Asiatul JannahBelum ada peringkat
- Drug Study DiazepamDokumen1 halamanDrug Study DiazepamjolibeecaldonaBelum ada peringkat
- Drug Study DiazepamDokumen1 halamanDrug Study DiazepamAnjae GariandoBelum ada peringkat
- Quick guide to common headache typesDokumen1 halamanQuick guide to common headache typesAlpacaBelum ada peringkat
- NEUROMUSCULARDokumen5 halamanNEUROMUSCULARIsabel HigginsBelum ada peringkat
- Regions Major Structures Functions Deficits: Anatomy of The BrainDokumen6 halamanRegions Major Structures Functions Deficits: Anatomy of The BrainCassandraBelum ada peringkat
- Cva Other DiseasesDokumen10 halamanCva Other Diseasessheila roma sibugBelum ada peringkat
- Compiled Psych MidtermsDokumen13 halamanCompiled Psych MidtermsicBelum ada peringkat
- Difference between dementia and normal agingDokumen152 halamanDifference between dementia and normal agingKaren Lim Delos ReyesBelum ada peringkat
- BSN3 - MEDSURG2 RLE - Neuro Assessment & Seizure PrecautionDokumen6 halamanBSN3 - MEDSURG2 RLE - Neuro Assessment & Seizure PrecautionADRIANNA NICOLE BAHALA GONZALEZBelum ada peringkat
- Medicine - Primary HeadacheDokumen5 halamanMedicine - Primary HeadacheyapBelum ada peringkat
- A Companion To Fish's PsychopathologyDokumen77 halamanA Companion To Fish's Psychopathologyolivukovic100% (1)
- Stroke Signs, Risks, and Nursing CareDokumen1 halamanStroke Signs, Risks, and Nursing CareMariel Febreo MerlanBelum ada peringkat
- Pathophysiology of SchizophreniaDokumen1 halamanPathophysiology of Schizophreniasarzlasco090% (1)
- Disorders of PerceptionDokumen36 halamanDisorders of Perceptionanony100% (1)
- PSY NSG DAY 2 SCHIZOPHRENIA CRISIS TYPESDokumen4 halamanPSY NSG DAY 2 SCHIZOPHRENIA CRISIS TYPESVictoria Castillo TamayoBelum ada peringkat
- Sudden Onset (Within 2 Weeks) of at Least One of TheDokumen2 halamanSudden Onset (Within 2 Weeks) of at Least One of TheNeicole BandalaBelum ada peringkat
- Icc & Nao PC HPC: Psychiatric HistoryDokumen10 halamanIcc & Nao PC HPC: Psychiatric HistoryJeffrey XieBelum ada peringkat
- SCHIZOPHRENIA: A Clinical Syndrome of Variable PsychopathologyDokumen7 halamanSCHIZOPHRENIA: A Clinical Syndrome of Variable PsychopathologyNica Lopez FernandezBelum ada peringkat
- Chapter 13Dokumen5 halamanChapter 13April Rose ElopreBelum ada peringkat
- Seizure and EpilepsyDokumen18 halamanSeizure and EpilepsyJamal JosephBelum ada peringkat
- Psychiatry 101Dokumen17 halamanPsychiatry 101Vaso Talakvadze0% (1)
- SchizophreniaDokumen2 halamanSchizophreniaIT’S ME HAYLA100% (1)
- Multi Infarct DementiaDokumen2 halamanMulti Infarct DementiaChristelle Ann FarralesBelum ada peringkat
- SchizopheniaDokumen2 halamanSchizopheniaChamara MudalinayakaBelum ada peringkat
- DR - Sherif Saad: Consultant of PsychiatryDokumen82 halamanDR - Sherif Saad: Consultant of PsychiatryKreshnik IdrizajBelum ada peringkat
- Neurological Examination SummaryDokumen90 halamanNeurological Examination SummaryAlida Taranu TernströmBelum ada peringkat
- Clinical Significance of Demyelinating Lesions of The CNSDokumen5 halamanClinical Significance of Demyelinating Lesions of The CNSTransverse Myelitis AssociationBelum ada peringkat
- Table 59-5 - Clinical Features of Common DementiasDokumen1 halamanTable 59-5 - Clinical Features of Common DementiasDragutin PetrićBelum ada peringkat
- Differential DiagnosisDokumen6 halamanDifferential Diagnosisjkarylle1216Belum ada peringkat
- Revista Chilena de Neuro-Psiquiatría: Corticobasal Degeneration: Clinical Report of 5 CasesDokumen15 halamanRevista Chilena de Neuro-Psiquiatría: Corticobasal Degeneration: Clinical Report of 5 CasesJurlay Dayana Villalba MartínezBelum ada peringkat
- Assessment & Management of Dissociative Disorders: Chairperson: DR - Safeekh A.T. Presenter: Dr.D.ArchanaaDokumen62 halamanAssessment & Management of Dissociative Disorders: Chairperson: DR - Safeekh A.T. Presenter: Dr.D.Archanaadrkadiyala2Belum ada peringkat
- Osms - It/alzheimers-Disease: Pathology & CausesDokumen1 halamanOsms - It/alzheimers-Disease: Pathology & Causesdysa ayu shalsabilaBelum ada peringkat
- Síndrome de Asperger: Una guía completa para comprender, vivir y tratar el síndrome de AspergerDari EverandSíndrome de Asperger: Una guía completa para comprender, vivir y tratar el síndrome de AspergerBelum ada peringkat
- Psychiatric Phenomenology From First Principles for Medical Students, Psychiatric Residents, and PractitionersDari EverandPsychiatric Phenomenology From First Principles for Medical Students, Psychiatric Residents, and PractitionersBelum ada peringkat
- Psychic Ability Plain & Simple: The Only Book You'll Ever NeedDari EverandPsychic Ability Plain & Simple: The Only Book You'll Ever NeedPenilaian: 5 dari 5 bintang5/5 (1)
- Hidden Disabilities and Conditions: Creating an Inclusive WorkplaceDari EverandHidden Disabilities and Conditions: Creating an Inclusive WorkplaceBelum ada peringkat
- Grade 11 Filipino Class Focuses on Language ConceptsDokumen6 halamanGrade 11 Filipino Class Focuses on Language ConceptsJeppssy Marie Concepcion MaalaBelum ada peringkat
- Statistics For Business Decision Making and Analysis 2nd Edition Stine Foster Test BankDokumen5 halamanStatistics For Business Decision Making and Analysis 2nd Edition Stine Foster Test Bankeloise100% (19)
- Kalidasa's Abhijnana Shakuntala and Indian PoeticsDokumen14 halamanKalidasa's Abhijnana Shakuntala and Indian PoeticsRishi BoraBelum ada peringkat
- First Seminar Presentation On Sing Unburied Sing by Jesmyn Ward - Section 24Dokumen3 halamanFirst Seminar Presentation On Sing Unburied Sing by Jesmyn Ward - Section 24hjt7cdnzhjBelum ada peringkat
- Culture, Law, and Reasoning: Week 1Dokumen77 halamanCulture, Law, and Reasoning: Week 1LIU DANBelum ada peringkat
- Plan Lectie, CL Ax-A, Word FormationDokumen5 halamanPlan Lectie, CL Ax-A, Word FormationBogdan Zancu100% (1)
- Moog Animatics SmartMotor DevelopersGuide Manual enDokumen948 halamanMoog Animatics SmartMotor DevelopersGuide Manual enAsh KetchumBelum ada peringkat
- English to Tamil Translation Tools and ResourcesDokumen1 halamanEnglish to Tamil Translation Tools and Resourcesarvind vinoBelum ada peringkat
- Logic and Reasoning Q3 FARIS NASIR F. QUILLA 2-2-22Dokumen5 halamanLogic and Reasoning Q3 FARIS NASIR F. QUILLA 2-2-22Shermen B. FloresBelum ada peringkat
- BSOD CodesDokumen19 halamanBSOD CodesJm VilleBelum ada peringkat
- Reported Speech With Reporting VerbsDokumen2 halamanReported Speech With Reporting Verbsklaid proctorBelum ada peringkat
- ProverbsDokumen12 halamanProverbsNantenainaFitiaBelum ada peringkat
- A. Definition of X-Bar Theory: B. The Syntax AssemblyDokumen9 halamanA. Definition of X-Bar Theory: B. The Syntax AssemblyMeggie UllyahBelum ada peringkat
- By Archibald Macleish: Ars PoeticaDokumen3 halamanBy Archibald Macleish: Ars PoeticaYasmin G. BaoitBelum ada peringkat
- GoalBankIEPVersion9NY PDFDokumen173 halamanGoalBankIEPVersion9NY PDFlirebien94% (16)
- Open Source - Kerja Kursus ICTDokumen11 halamanOpen Source - Kerja Kursus ICTFirdaus Ahmad100% (1)
- Create Permission RoleDokumen13 halamanCreate Permission RolemalimojBelum ada peringkat
- ETC Peter Rabbit Study GuideDokumen33 halamanETC Peter Rabbit Study GuideMohammad WorldBelum ada peringkat
- DDCA Lab05Dokumen3 halamanDDCA Lab05Группа СМ5-41Belum ada peringkat
- Linear Control Lab Manual Introduction to MATLABDokumen69 halamanLinear Control Lab Manual Introduction to MATLABHadiGunaBelum ada peringkat
- The Clown PunkDokumen1 halamanThe Clown Punkraab1Belum ada peringkat
- Guided Notes Packet - Argumentative WritingDokumen12 halamanGuided Notes Packet - Argumentative Writingapi-498343131Belum ada peringkat
- Mecal: Ecu Calibration SoftwareDokumen58 halamanMecal: Ecu Calibration SoftwarecastrokermanBelum ada peringkat
- Oracle Apps Blog - Tricks & Scripts ..Dokumen10 halamanOracle Apps Blog - Tricks & Scripts ..ashibekBelum ada peringkat
- DCP-9040CN 9042CDN MFC-9440CN 9450CDN PDFDokumen43 halamanDCP-9040CN 9042CDN MFC-9440CN 9450CDN PDFStefanGarnetBelum ada peringkat
- Multicon User Manual: Revision: TDokumen99 halamanMulticon User Manual: Revision: TRaj BenBelum ada peringkat
- Learn Object-Oriented Programming (OOP) in CDokumen39 halamanLearn Object-Oriented Programming (OOP) in CkarijghfdBelum ada peringkat
- HANA Tables TemporaryTables 1.00.100+Dokumen7 halamanHANA Tables TemporaryTables 1.00.100+subra1032Belum ada peringkat
- Human Evolution UCSPDokumen4 halamanHuman Evolution UCSPJamaela BulajaoBelum ada peringkat
- A Jump Start to OpenCL: Another Language for Parallel ComputingDokumen74 halamanA Jump Start to OpenCL: Another Language for Parallel ComputingkaoutarBelum ada peringkat