Anda mungkin juga menyukai
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (399)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- Assessment PrintDokumen204 halamanAssessment Printbruceaq100% (7)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (73)
- 3.5 Developmental Stages in Infant and Toddler Feeding NEWDokumen12 halaman3.5 Developmental Stages in Infant and Toddler Feeding NEWYusrinaNoorAzizahBelum ada peringkat
- Mammography Solutions: Serenys Serenys DR Serenys DBTDokumen4 halamanMammography Solutions: Serenys Serenys DR Serenys DBTHanna FettahBelum ada peringkat
- Social Media Use by SeniorsDokumen8 halamanSocial Media Use by SeniorsHelloBelum ada peringkat
- Social Media Use by SeniorsDokumen8 halamanSocial Media Use by SeniorsHelloBelum ada peringkat
- AEPS Criteria Birth To 3Dokumen49 halamanAEPS Criteria Birth To 3Yamuna Govindaraj100% (1)
- Prinsip OnkologiDokumen20 halamanPrinsip OnkologiTitaPuspitasariBelum ada peringkat
- Is Generation Y Addicted? How Social Media Affects RelationshipsDokumen10 halamanIs Generation Y Addicted? How Social Media Affects RelationshipsYamuna GovindarajBelum ada peringkat
- Is Generation Y Addicted? How Social Media Affects RelationshipsDokumen10 halamanIs Generation Y Addicted? How Social Media Affects RelationshipsYamuna GovindarajBelum ada peringkat
- Test Bank For Merrills Atlas of Radiographic Positioning and Procedures 14th Edition by LongDokumen5 halamanTest Bank For Merrills Atlas of Radiographic Positioning and Procedures 14th Edition by LongMarcus Gorman100% (29)
- PGMI Digital Image Reference Set: Version 1, February 2011Dokumen28 halamanPGMI Digital Image Reference Set: Version 1, February 2011Yamuna GovindarajBelum ada peringkat
- Top Radiologists and Medical Clinics in CoimbatoreDokumen6 halamanTop Radiologists and Medical Clinics in CoimbatoreshahulBelum ada peringkat
- Ionizing RadiationDokumen112 halamanIonizing RadiationYamuna GovindarajBelum ada peringkat
- Facebook Addiction Among Malaysian StudentsDokumen6 halamanFacebook Addiction Among Malaysian StudentsYamuna GovindarajBelum ada peringkat
- The Use of Facebook For Educational Purposes in EFL ClassroomsDokumen7 halamanThe Use of Facebook For Educational Purposes in EFL ClassroomsYamuna GovindarajBelum ada peringkat
- Facebooking in Today's Net Generation Prospects and ChallengesDokumen16 halamanFacebooking in Today's Net Generation Prospects and ChallengesYamuna GovindarajBelum ada peringkat
- Students' Opinions On Facebook Supported Blended Learning EnvironmentDokumen8 halamanStudents' Opinions On Facebook Supported Blended Learning EnvironmentYamuna GovindarajBelum ada peringkat
- 2011 Relationship Maintenance and FacebookDokumen52 halaman2011 Relationship Maintenance and FacebookYamuna GovindarajBelum ada peringkat
- 2016 Gender and Facebook Motives As Predictors of Specific Types of Facebook Use A Latent Growth Curve Analysis in Adolescence PDFDokumen9 halaman2016 Gender and Facebook Motives As Predictors of Specific Types of Facebook Use A Latent Growth Curve Analysis in Adolescence PDFYamuna GovindarajBelum ada peringkat
- 2011 Facebook Addiction Factors Influencing An Individuals AddictionDokumen29 halaman2011 Facebook Addiction Factors Influencing An Individuals AddictionYamuna GovindarajBelum ada peringkat
- 2016 Social Networking, A New Online Addiction A Review of Facebook and Other Addiction DisordersDokumen6 halaman2016 Social Networking, A New Online Addiction A Review of Facebook and Other Addiction DisordersYamuna GovindarajBelum ada peringkat
- Facebook Addiction Among Malaysian StudentsDokumen6 halamanFacebook Addiction Among Malaysian StudentsYamuna GovindarajBelum ada peringkat
- 2008 Student Favorite Facebook and Motives For Its UseDokumen16 halaman2008 Student Favorite Facebook and Motives For Its UseYamuna GovindarajBelum ada peringkat
- 2011 Facebook Addiction Factors Influencing An Individuals AddictionDokumen29 halaman2011 Facebook Addiction Factors Influencing An Individuals AddictionYamuna GovindarajBelum ada peringkat
- A Case Study of Preschool Children Exhibiting Prosocial and Empathy Toldo 2014Dokumen184 halamanA Case Study of Preschool Children Exhibiting Prosocial and Empathy Toldo 2014Yamuna GovindarajBelum ada peringkat
- 2008 Student Favorite Facebook and Motives For Its UseDokumen16 halaman2008 Student Favorite Facebook and Motives For Its UseYamuna GovindarajBelum ada peringkat
- A Sociocultural Perspective On Childrens Early Language A Family StudyDokumen18 halamanA Sociocultural Perspective On Childrens Early Language A Family StudyYamuna GovindarajBelum ada peringkat
- Assessment of The Psychosocial Development Refugee in ThailandDokumen28 halamanAssessment of The Psychosocial Development Refugee in ThailandYamuna GovindarajBelum ada peringkat
- A Cultural-Historical Reading of The Emotional Development of Young ChildrenDokumen21 halamanA Cultural-Historical Reading of The Emotional Development of Young ChildrenYamuna GovindarajBelum ada peringkat
- Artifact AvoidanceDokumen4 halamanArtifact AvoidanceYamuna GovindarajBelum ada peringkat
- Attachment Stability and EmotionalDokumen22 halamanAttachment Stability and EmotionalYamuna GovindarajBelum ada peringkat
- A Cultural-Historical Reading of The Emotional Development of Young ChildrenDokumen21 halamanA Cultural-Historical Reading of The Emotional Development of Young ChildrenYamuna GovindarajBelum ada peringkat
- Example Independent Sample T Test PDFDokumen3 halamanExample Independent Sample T Test PDFYamuna GovindarajBelum ada peringkat
- GPCALMA A Grid Approach To Mammographic ScreeningDokumen5 halamanGPCALMA A Grid Approach To Mammographic ScreeningYamuna GovindarajBelum ada peringkat
- Dr. Sumait Hospital: Final Investigation ReportDokumen10 halamanDr. Sumait Hospital: Final Investigation ReportShafici CqadirBelum ada peringkat
- Jurnal Vaksin HPVDokumen9 halamanJurnal Vaksin HPVlitaayuningdyahBelum ada peringkat
- Mamografia Vs TomosintesisDokumen9 halamanMamografia Vs TomosintesisAndreaCostalesBelum ada peringkat
- Complete Blood Picture (CBC) PDFDokumen1 halamanComplete Blood Picture (CBC) PDFRizwan yousafBelum ada peringkat
- Cardiac Silhouette Is Normal. Rib Cage Appears NormalDokumen2 halamanCardiac Silhouette Is Normal. Rib Cage Appears Normalsumit1234ggBelum ada peringkat
- Balio Ox-580 Brochure enDokumen4 halamanBalio Ox-580 Brochure enMo AlyBelum ada peringkat
- LaparosDokumen3 halamanLaparosMurtaz BokhuaBelum ada peringkat
- Radiography SafetyDokumen45 halamanRadiography SafetyErland A. Rukka100% (1)
- Approach To ProteinuriaDokumen14 halamanApproach To ProteinuriaRishi ShresthaBelum ada peringkat
- Jurnal Pelyanana RadiologiDokumen8 halamanJurnal Pelyanana RadiologiAdeanisa FiqriBelum ada peringkat
- Hepatic Cysts Workup Guide for Healthcare ProfessionalsDokumen4 halamanHepatic Cysts Workup Guide for Healthcare ProfessionalsMariska JuanitaBelum ada peringkat
- Rapid T2-Weighted Turbo Spin Echo MultiVane Brain MRI Using Compressed SENSE A Qualitative AnalysisDokumen8 halamanRapid T2-Weighted Turbo Spin Echo MultiVane Brain MRI Using Compressed SENSE A Qualitative AnalysisBella YulandaBelum ada peringkat
- Control assay ranges for hematology parametersDokumen9 halamanControl assay ranges for hematology parameterslccaelusBelum ada peringkat
- Fathur Rahman PDFDokumen1 halamanFathur Rahman PDFRSCERIA KANDANGANBelum ada peringkat
- A3 1 2Dokumen4 halamanA3 1 2meowBelum ada peringkat
- 30.apai .14 MalDokumen28 halaman30.apai .14 MalThit Htoo LwinBelum ada peringkat
- Laporan Kinerja Lab Per Pasien Pemeriksaan 2022-10-09 S - D 2022-10-09Dokumen72 halamanLaporan Kinerja Lab Per Pasien Pemeriksaan 2022-10-09 S - D 2022-10-09LaboratoriumBelum ada peringkat
- HRCT Thorax Protocol Vs Low Dose CTDokumen21 halamanHRCT Thorax Protocol Vs Low Dose CTchristianhasudungan319Belum ada peringkat
- Imaging Request: Diagnostic ProcedureDokumen4 halamanImaging Request: Diagnostic ProcedureMarielle ChuaBelum ada peringkat
- Research Center in Gastroenterology and HepatologyDokumen12 halamanResearch Center in Gastroenterology and Hepatologynihilx27374Belum ada peringkat
- Radiography and Imaging Technology Question PaperDokumen6 halamanRadiography and Imaging Technology Question PaperMohd ShmlBelum ada peringkat
- RadiologyDokumen2 halamanRadiologyImrose MahineBelum ada peringkat
- Daftar PustakaDokumen2 halamanDaftar PustakaMeiBelum ada peringkat
- MR Scanning - Questions and Answers in MRIDokumen2 halamanMR Scanning - Questions and Answers in MRIआयुष चौधरीBelum ada peringkat
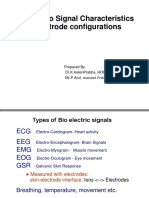
- Bio Signal Characteristics and Electrode ConfigurationsDokumen54 halamanBio Signal Characteristics and Electrode Configurationspriya dharshiniBelum ada peringkat
- List of AbbreviationsDokumen6 halamanList of Abbreviationsdeni2razmoskiBelum ada peringkat