Anda mungkin juga menyukai
- ECG & EKG Interpretation: How to interpret ECG & EKG, including rhythms, arrhythmias, and more!Dari EverandECG & EKG Interpretation: How to interpret ECG & EKG, including rhythms, arrhythmias, and more!Belum ada peringkat
- Electrocardiography in Emergency, Acute, and Critical Care, 2nd EditionDari EverandElectrocardiography in Emergency, Acute, and Critical Care, 2nd EditionPenilaian: 5 dari 5 bintang5/5 (1)
- ECG InterpretationDokumen5 halamanECG InterpretationRichelle Dianne Ramos-Giang100% (3)
- ECG InterpretationDokumen95 halamanECG InterpretationShiela Mae Lopez100% (10)
- EKG Pocket GuideDokumen2 halamanEKG Pocket GuideFabian Ramirez HincapiéBelum ada peringkat
- ECG Rhythm Interpretation 2007Dokumen533 halamanECG Rhythm Interpretation 2007user123456798100% (20)
- ECG Mastery Improving Your ECG Interpretation SkillsDokumen23 halamanECG Mastery Improving Your ECG Interpretation SkillsHitesh Deora100% (2)
- ECG Interpretation Cheat SheetDokumen1 halamanECG Interpretation Cheat Sheethirsi20051879% (24)
- Ecg Cheat Sheet 35Dokumen2 halamanEcg Cheat Sheet 35jessjaylee80% (5)
- Basic ECG ReadingDokumen41 halamanBasic ECG ReadingBenj100% (4)
- Recognizing Normal ECGDokumen50 halamanRecognizing Normal ECGJosiephine Bucalon100% (3)
- Ekg Strip NotesDokumen13 halamanEkg Strip NotesNick Loizzo100% (2)
- EKG ExamplesDokumen9 halamanEKG ExamplesMayer Rosenberg99% (235)
- ECG StripsDokumen5 halamanECG StripsNursingSchoolNotes100% (1)
- Easy ECG GuideDokumen17 halamanEasy ECG GuideDr.Chinmay Kulkarni83% (12)
- ECG ReadingDokumen11 halamanECG ReadingSuresh Shrestha100% (1)
- EKG Practice TestDokumen16 halamanEKG Practice TestAbdul Rohim100% (1)
- ArrhythmiaDokumen2 halamanArrhythmiaChris Pritchard93% (30)
- ECG InterpretationDokumen52 halamanECG InterpretationMarcus, RN98% (44)
- Abnormal ECGDokumen55 halamanAbnormal ECGdevilbata50% (2)
- Basic EKG InterpretationDokumen4 halamanBasic EKG InterpretationPRaDo PATBelum ada peringkat
- Basic ECG and Arrhythmia FINALDokumen16 halamanBasic ECG and Arrhythmia FINALCharlotte James100% (5)
- Ecg Made EasyDokumen343 halamanEcg Made EasyAbegail IbañezBelum ada peringkat
- Electrocardiography (Ecg) : Presented By: Fahad I. HussienDokumen102 halamanElectrocardiography (Ecg) : Presented By: Fahad I. HussienMustafa A. DawoodBelum ada peringkat
- Cardiac DysrhythmiasDokumen3 halamanCardiac DysrhythmiasKatherine Santiago92% (62)
- EKG Flash CardsDokumen5 halamanEKG Flash CardsRyann Sampino FreitasBelum ada peringkat
- Acid-Base WorksheetDokumen2 halamanAcid-Base WorksheetMayer Rosenberg100% (18)
- Basic EKG For DummiesDokumen133 halamanBasic EKG For Dummieseduardocmoura86% (7)
- A Simplified ECG GuideDokumen4 halamanA Simplified ECG Guidejalan_z96% (27)
- Basic Arrhythmia RulesDokumen3 halamanBasic Arrhythmia Rulesgreenflames0997% (30)
- Ekg BookDokumen118 halamanEkg BookDenisa Cenaj100% (1)
- Respiratory DysfunctionDokumen1 halamanRespiratory Dysfunctionoxidalaj100% (3)
- Emergency Department Resuscitation of the Critically Ill, 2nd Edition: A Crash Course in Critical CareDari EverandEmergency Department Resuscitation of the Critically Ill, 2nd Edition: A Crash Course in Critical CareBelum ada peringkat
- EKG and ECG Interpretation: Learn EKG Interpretation, Rhythms, and Arrhythmia Fast!Dari EverandEKG and ECG Interpretation: Learn EKG Interpretation, Rhythms, and Arrhythmia Fast!Belum ada peringkat
- The 12-Lead Electrocardiogram for Nurses and Allied ProfessionalsDari EverandThe 12-Lead Electrocardiogram for Nurses and Allied ProfessionalsBelum ada peringkat
- ECG/EKG Interpretation: An Easy Approach to Read a 12-Lead ECG and How to Diagnose and Treat ArrhythmiasDari EverandECG/EKG Interpretation: An Easy Approach to Read a 12-Lead ECG and How to Diagnose and Treat ArrhythmiasPenilaian: 5 dari 5 bintang5/5 (2)
- EKG/ECG Interpretation Made Easy: A Practical Approach to Passing the ECG/EKG Portion of NCLEXDari EverandEKG/ECG Interpretation Made Easy: A Practical Approach to Passing the ECG/EKG Portion of NCLEXPenilaian: 5 dari 5 bintang5/5 (2)
- FRCEM FINAL: Critical Appraisal Made Easy e-BookDari EverandFRCEM FINAL: Critical Appraisal Made Easy e-BookPenilaian: 5 dari 5 bintang5/5 (1)
- EKG | ECG: An Ultimate Step-By-Step Guide to 12-Lead EKG | ECG Interpretation, Rhythms & Arrhythmias Including Basic Cardiac DysrhythmiasDari EverandEKG | ECG: An Ultimate Step-By-Step Guide to 12-Lead EKG | ECG Interpretation, Rhythms & Arrhythmias Including Basic Cardiac DysrhythmiasPenilaian: 3 dari 5 bintang3/5 (5)
- Advance Cardiac Life Support: Short, Sweet and to the PointDari EverandAdvance Cardiac Life Support: Short, Sweet and to the PointPenilaian: 3 dari 5 bintang3/5 (2)
- With A Pulse and Poor Perfusion: Pediatric TachycardiaDokumen1 halamanWith A Pulse and Poor Perfusion: Pediatric TachycardiaIin-Ignasia Diahayujulindah Mujiman0% (1)
- NCM 112 MSN Prelim Topic 4 Cardiac Rhythm DisordersDokumen5 halamanNCM 112 MSN Prelim Topic 4 Cardiac Rhythm DisordersKim Erida QuezonBelum ada peringkat
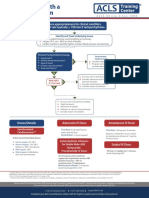
- Assess Appropriateness For Clinical Condition. Heart Rate Typically 150/min If TachyarrhythmiaDokumen1 halamanAssess Appropriateness For Clinical Condition. Heart Rate Typically 150/min If TachyarrhythmiaSiti Nur R Firda FauziyahBelum ada peringkat
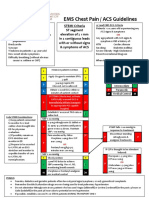
- EMS Chest Pain / ACS GuidelinesDokumen1 halamanEMS Chest Pain / ACS GuidelinesJuanaly BadiolaBelum ada peringkat
- Format in Drug StudyDokumen14 halamanFormat in Drug StudyShenielyn Bartolome NapolitanoBelum ada peringkat
- G2015 Adult Tachycardia PDFDokumen1 halamanG2015 Adult Tachycardia PDFPlabber JuneBelum ada peringkat
- G2015 Adult Tachycardia PDFDokumen1 halamanG2015 Adult Tachycardia PDFibbs91Belum ada peringkat
- AdultTachycardiaWithPulse AlgorithmDokumen1 halamanAdultTachycardiaWithPulse AlgorithmIsmail SlimBelum ada peringkat
- ACLS Algorithm Pulse No Yes: Stable Patient Unstable Patient Stable PatientDokumen1 halamanACLS Algorithm Pulse No Yes: Stable Patient Unstable Patient Stable PatientAhmed AlkhaqaniBelum ada peringkat
- Peri-Arrest ArrythmiaDokumen14 halamanPeri-Arrest Arrythmiamohamed mowafeyBelum ada peringkat
- Drug Study ErDokumen3 halamanDrug Study ErZheyrille A. ArevaloBelum ada peringkat
- Simplified ACLS AlgorithmDokumen1 halamanSimplified ACLS AlgorithmBrianBelum ada peringkat
- Critical Care Drug Reference SheetDokumen12 halamanCritical Care Drug Reference SheetYanina CoxBelum ada peringkat
- Drug StudyDokumen5 halamanDrug Studyeduardbaldoz69Belum ada peringkat
- Drug 3Dokumen8 halamanDrug 3Lorenzo LiteBelum ada peringkat
- Sinus Bradycardia: o No TX If AsymptomaticDokumen3 halamanSinus Bradycardia: o No TX If Asymptomaticelle50% (2)
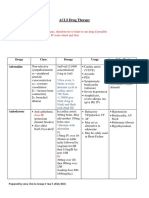
- ACLS Drug Therapy RevisedDokumen4 halamanACLS Drug Therapy RevisedpaveethrahBelum ada peringkat
- Mind Maping MIDokumen1 halamanMind Maping MIimambiyono9728Belum ada peringkat
- Generic Name: Action: Indications: Adverse Effects:: Injection, OTC Nasal SolutionDokumen20 halamanGeneric Name: Action: Indications: Adverse Effects:: Injection, OTC Nasal SolutionBhupesh PatidarBelum ada peringkat
- EpinephrineDokumen1 halamanEpinephrineGreshil Castro IgtanlocBelum ada peringkat
- Intro Research Study IIDokumen1 halamanIntro Research Study IIAnton LaurencianaBelum ada peringkat
- Cholecystitis Case PresDokumen103 halamanCholecystitis Case PresAnton LaurencianaBelum ada peringkat
- Topic Outline OF Functional Health Pattern Assessment: Early ChildhoodDokumen3 halamanTopic Outline OF Functional Health Pattern Assessment: Early ChildhoodAnton LaurencianaBelum ada peringkat
- Tidal ModelDokumen2 halamanTidal ModelAnton LaurencianaBelum ada peringkat
- Chest Trauma Concept MapDokumen10 halamanChest Trauma Concept MapAnton Laurenciana100% (1)
- Multiple Physical Injuries Secondary To Vehicular AccidentDokumen31 halamanMultiple Physical Injuries Secondary To Vehicular AccidentAnton Laurenciana50% (2)
- Electrocardiography II StudentDokumen20 halamanElectrocardiography II StudentArmando Valdez ZamoranoBelum ada peringkat
- Acls DrugsDokumen5 halamanAcls DrugsDebby Christiana SBelum ada peringkat
- Learning Plan Medsurg Clinical RotationDokumen7 halamanLearning Plan Medsurg Clinical Rotationapi-275795160100% (2)
- Palpitations AND Heartbeat Disorders: By: Aisha Sara Tasnim Physician: DR SsebulibaDokumen22 halamanPalpitations AND Heartbeat Disorders: By: Aisha Sara Tasnim Physician: DR SsebulibaNinaBelum ada peringkat
- Tachyarrhythmia SDokumen46 halamanTachyarrhythmia SAsif HameedBelum ada peringkat
- Abnormal EcgDokumen8 halamanAbnormal EcgM.DalaniBelum ada peringkat
- Ecg Pathology 02Dokumen95 halamanEcg Pathology 02Andi MP Manurung100% (1)
- Basic Arrhythmia RulesDokumen3 halamanBasic Arrhythmia Rulesgreenflames0997% (30)
- Atropine Sulfate 1 mg/5 ML: Aguettant SystemDokumen2 halamanAtropine Sulfate 1 mg/5 ML: Aguettant Systemsandeep thakurBelum ada peringkat
- Intrinsic Conduction System of Heart: Setting The Basic RhythmDokumen3 halamanIntrinsic Conduction System of Heart: Setting The Basic RhythmDeniebev'z OrillosBelum ada peringkat
- BAV 1-S2.0-S1443950623043585-MainDokumen4 halamanBAV 1-S2.0-S1443950623043585-MainconstanzacaceresgalvezBelum ada peringkat
- Mastering Temporary Invasive Cardiac Pacing: ClinicalDokumen8 halamanMastering Temporary Invasive Cardiac Pacing: ClinicaldenokBelum ada peringkat
- The Six Second ECG: Annotated Answer KeyDokumen9 halamanThe Six Second ECG: Annotated Answer KeyRaquel GirónBelum ada peringkat
- Cardiology - ArrhythmiaDokumen18 halamanCardiology - Arrhythmiadrfabianomarins100% (1)
- Precedex Dosing GuidelinesDokumen15 halamanPrecedex Dosing GuidelinesemonhalimBelum ada peringkat
- Anaesthesia Management of Patient of PacemakerDokumen92 halamanAnaesthesia Management of Patient of PacemakerSiva KrishnaBelum ada peringkat
- Harrison Self-Assessment and Board Review (1) - 403-490Dokumen88 halamanHarrison Self-Assessment and Board Review (1) - 403-490Cristobal Andres Fernandez Coentrao100% (2)
- EKGDokumen137 halamanEKGGbariel100% (3)
- Pharmacology List of DrugsDokumen66 halamanPharmacology List of DrugsSohail Adnan100% (2)
- Complete Heart BlockDokumen13 halamanComplete Heart BlockSubhranil MaityBelum ada peringkat
- 2021 ESC Guidelines On Cardiac Pacing and Cardiac Resynchronization TherapyDokumen107 halaman2021 ESC Guidelines On Cardiac Pacing and Cardiac Resynchronization TherapyLourdes FrancoBelum ada peringkat
- Daftar PustakaDokumen3 halamanDaftar Pustakabalthier37Belum ada peringkat
- DR Yassir Javaid Interpreting The 12 Lead ECGDokumen28 halamanDR Yassir Javaid Interpreting The 12 Lead ECGTirtha TaposhBelum ada peringkat
- Lanoxin: (Digoxin) InjectionDokumen35 halamanLanoxin: (Digoxin) InjectionZainBelum ada peringkat
- Handbook Drugs in Intensive Care (6 Pages)Dokumen6 halamanHandbook Drugs in Intensive Care (6 Pages)ardriangollerBelum ada peringkat
- GP Emergency Manual PDFDokumen72 halamanGP Emergency Manual PDFRumana Ali100% (2)
- Drugs NclexDokumen30 halamanDrugs Nclexawuahboh100% (1)
- EKG StripsDokumen10 halamanEKG StripsSaidel ElizondoBelum ada peringkat
- Pulse Diagnosis of Chinese MedicineDokumen69 halamanPulse Diagnosis of Chinese MedicineYanikdj100% (3)
- Azure™ XT DR MRI SureScan™ W2DR01Dokumen44 halamanAzure™ XT DR MRI SureScan™ W2DR01mytake100Belum ada peringkat