Anda mungkin juga menyukai
- WHO Vaccine Manual PDFDokumen112 halamanWHO Vaccine Manual PDFRagel CorpsBelum ada peringkat
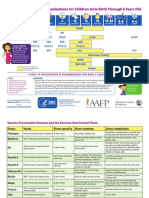
- Parent Ver SCH 0 6yrs AafpDokumen2 halamanParent Ver SCH 0 6yrs AafpcicitBelum ada peringkat
- MMC Med Cert 4 Rabies Shots Melissa FerrerDokumen4 halamanMMC Med Cert 4 Rabies Shots Melissa FerrerNadia ZialcitaBelum ada peringkat
- DEE EHU 4-2-4 Risk RegisterDokumen36 halamanDEE EHU 4-2-4 Risk RegisterJonasBelum ada peringkat
- The Public Health System in Afghanistan: Current Issues: January 2002Dokumen47 halamanThe Public Health System in Afghanistan: Current Issues: January 2002جاهد نبیل100% (1)
- Conflicts of Interest - Undermine Children's HealthDokumen42 halamanConflicts of Interest - Undermine Children's HealthSeth Alexander WoodBelum ada peringkat
- Health 1Dokumen3 halamanHealth 1api-354040213Belum ada peringkat
- Pre-Placement Immunization Form (June 2017) BrockDokumen2 halamanPre-Placement Immunization Form (June 2017) BrockroldinpgBelum ada peringkat
- Health and Safety PassportDokumen3 halamanHealth and Safety Passportapi-660085924Belum ada peringkat
- Sars-Cov-2 RT PCR Testing: Test Description Method ResultDokumen1 halamanSars-Cov-2 RT PCR Testing: Test Description Method ResultMAYUR PATELBelum ada peringkat
- Activity in EPI and MCHDokumen5 halamanActivity in EPI and MCHHazel MarananBelum ada peringkat
- Wil Document Requirements Passport 1Dokumen3 halamanWil Document Requirements Passport 1api-283084320Belum ada peringkat
- Hasil Pemeriksaan Laboratorium: Laboratory Test ResultDokumen1 halamanHasil Pemeriksaan Laboratorium: Laboratory Test ResultAmoy Ida Royani NababanBelum ada peringkat
- AnthonyDokumen1 halamanAnthonyJ D PatelBelum ada peringkat
- Singh: COVID19 Qualitative by Real Time PCRDokumen1 halamanSingh: COVID19 Qualitative by Real Time PCRPushpendra SinghBelum ada peringkat
- Genomics COVID19 Qualitative by Real Time PCR (ICMR No. SUPRA001f)Dokumen1 halamanGenomics COVID19 Qualitative by Real Time PCR (ICMR No. SUPRA001f)adityaBelum ada peringkat
- Mobile No.: Real Time PCRDokumen1 halamanMobile No.: Real Time PCRsunil singh raghavBelum ada peringkat
- Hasil Pemeriksaan Laboratorium: Laboratory Test ResultDokumen1 halamanHasil Pemeriksaan Laboratorium: Laboratory Test ResultEdwin EdwinBelum ada peringkat
- Maklumat Penting - Atau Hospital/Klinik Swasta. - : Form Pd1Dokumen9 halamanMaklumat Penting - Atau Hospital/Klinik Swasta. - : Form Pd1Syazwi BaharuddinBelum ada peringkat
- ParthDokumen1 halamanParthJ D PatelBelum ada peringkat
- Sars-Cov-2: Empowers To Live WellDokumen2 halamanSars-Cov-2: Empowers To Live WellAkhil KBelum ada peringkat
- MBA07032 Daksh RTPCRDokumen1 halamanMBA07032 Daksh RTPCRDakshBelum ada peringkat
- Investigation Report: Type of Sample: Nasopharyngeal Swab Test ResultDokumen1 halamanInvestigation Report: Type of Sample: Nasopharyngeal Swab Test ResultNazim Uddin MahmudBelum ada peringkat
- Draft of Research ToolDokumen18 halamanDraft of Research Toolmayur.polBelum ada peringkat
- Molecular Biology Sars-Cov-2 (Covid 19) Detection by Real Time PCRDokumen2 halamanMolecular Biology Sars-Cov-2 (Covid 19) Detection by Real Time PCRMithileshBelum ada peringkat
- CGH202008000915 - Lab A2 2020 2231 - Laboratory - Covid PCR Test PDFDokumen2 halamanCGH202008000915 - Lab A2 2020 2231 - Laboratory - Covid PCR Test PDFMichael JonasanBelum ada peringkat
- Test Report: Orf 1ab Negative N Gene Negative Internal Control Pass 2019-Ncov NegativeDokumen1 halamanTest Report: Orf 1ab Negative N Gene Negative Internal Control Pass 2019-Ncov NegativeNilotpal RaiBelum ada peringkat
- Vidit Sudani 2Dokumen1 halamanVidit Sudani 2malvisha jadejaBelum ada peringkat
- Hasil Pemeriksaan Laboratorium: Laboratory Test ResultDokumen1 halamanHasil Pemeriksaan Laboratorium: Laboratory Test ResultRomi Apriansyah1Belum ada peringkat
- ArvindbhaiDokumen1 halamanArvindbhaiJ D PatelBelum ada peringkat
- Covid-19 by Real Time RT PCRDokumen2 halamanCovid-19 by Real Time RT PCRArun AntonyBelum ada peringkat
- Laboratory Report /:: Dis. At:::::: 31 Years 0122201673 Male Mr. Shakti Singh GaurDokumen2 halamanLaboratory Report /:: Dis. At:::::: 31 Years 0122201673 Male Mr. Shakti Singh GaurShakti singh gaur100% (1)
- Health Booklet 2014Dokumen68 halamanHealth Booklet 2014Tan KMBelum ada peringkat
- Department of Laboratory SciencesDokumen1 halamanDepartment of Laboratory SciencesYolopoloBelum ada peringkat
- C284146 Covidtempl Abdul 050821164842Dokumen1 halamanC284146 Covidtempl Abdul 050821164842Sarhm SevenBelum ada peringkat
- TB ReportDokumen1 halamanTB ReportkishoreBelum ada peringkat
- Sars-Cov-2 RT PCR Testing: Test Description Method ResultDokumen1 halamanSars-Cov-2 RT PCR Testing: Test Description Method ResultRitesh RanjanBelum ada peringkat
- Covid-19 Test Report: PATIENT NAME: Indu Gupta Raj BalaDokumen1 halamanCovid-19 Test Report: PATIENT NAME: Indu Gupta Raj BalaTarun BhatnagarBelum ada peringkat
- Department of Microbiology: Ispat General HospitalDokumen1 halamanDepartment of Microbiology: Ispat General HospitalNamrata JhaBelum ada peringkat
- Mobile No.: Real Time PCRDokumen1 halamanMobile No.: Real Time PCRPushpendra SinghBelum ada peringkat
- Prachi S Patel Sex/Age: Female / 25 Years: Real Time PCRDokumen1 halamanPrachi S Patel Sex/Age: Female / 25 Years: Real Time PCRprachi patelBelum ada peringkat
- Hasil Pemeriksaan Laboratorium: Laboratory Examination ResultDokumen1 halamanHasil Pemeriksaan Laboratorium: Laboratory Examination ResultMukhammad FakhriBelum ada peringkat
- Hasil Pemeriksaan Laboratorium: Laboratory Test ResultDokumen1 halamanHasil Pemeriksaan Laboratorium: Laboratory Test Resultazzahra fotocopiBelum ada peringkat
- Covid-19 by Real Time RT PCRDokumen2 halamanCovid-19 by Real Time RT PCRArun AntonyBelum ada peringkat
- PSW6 - PPHFDokumen16 halamanPSW6 - PPHFanishthBelum ada peringkat
- Emt Physical FormDokumen1 halamanEmt Physical FormLeeann LopezBelum ada peringkat
- Philippine Red Cross Molecular Laboratory Result Form: Date: NameDokumen1 halamanPhilippine Red Cross Molecular Laboratory Result Form: Date: NamePatrick John Estrada GayoBelum ada peringkat
- 2103060187B 0009 Mypd.0000499140 Opv2103060335.2728457 1132939.ior2103060248 20210306215330Dokumen1 halaman2103060187B 0009 Mypd.0000499140 Opv2103060335.2728457 1132939.ior2103060248 20210306215330Nadya Salsabila FrendytaBelum ada peringkat
- Report 3Dokumen2 halamanReport 3kazimkureshiBelum ada peringkat
- Revisi STANDAR PELAYANAN LABORATORIUM EditDokumen47 halamanRevisi STANDAR PELAYANAN LABORATORIUM EditMuhamad SetoBelum ada peringkat
- Max Lab ReportDokumen1 halamanMax Lab ReportKallu PrasadBelum ada peringkat
- Hasil Pemeriksaan Laboratorium: Laboratory Test ResultDokumen1 halamanHasil Pemeriksaan Laboratorium: Laboratory Test ResultDwi SaputroBelum ada peringkat
- 4th Generation HIV TestingDokumen31 halaman4th Generation HIV TestingSC SCBelum ada peringkat
- 021 Mononucleosis Rapid Test DeviceDokumen6 halaman021 Mononucleosis Rapid Test DeviceEslam NassarBelum ada peringkat
- Text Instruction 3Dokumen1 halamanText Instruction 3kutukucinkBelum ada peringkat
- Rituj Covid ReportDokumen1 halamanRituj Covid ReportRituj ShahBelum ada peringkat
- Molecular Biology: Client Name and AddressDokumen1 halamanMolecular Biology: Client Name and AddressRituj ShahBelum ada peringkat
- Rituj Covid ReportDokumen1 halamanRituj Covid ReportRituj ShahBelum ada peringkat
- Real Time PCR: ICMR No. SUPRA001fDokumen1 halamanReal Time PCR: ICMR No. SUPRA001fPushpendra Singh100% (1)
- Hasil A.N Dadang Amor KuswaraDokumen1 halamanHasil A.N Dadang Amor KuswaraRoy Bin AgustinBelum ada peringkat
- Government of Telangana Covid Interim Test Report CCMB, HyderabadDokumen2 halamanGovernment of Telangana Covid Interim Test Report CCMB, HyderabadNagarjunaBelum ada peringkat
- Interpretation: Index Value Result: Immunology Test Name Result Bio. Ref. Range MethodDokumen2 halamanInterpretation: Index Value Result: Immunology Test Name Result Bio. Ref. Range MethodMithlesh YadavBelum ada peringkat
- (FORM) Medical Report AllDokumen2 halaman(FORM) Medical Report AllIndah AcphBelum ada peringkat
- Agenda Pediatrica Baby WinnieDokumen22 halamanAgenda Pediatrica Baby WinniepapergraficolorBelum ada peringkat
- MR Amit Thakkar - 7028246333Dokumen5 halamanMR Amit Thakkar - 7028246333Mahesh PallaviBelum ada peringkat
- Advances in PET: The Latest in Instrumentation, Technology, and Clinical PracticeDari EverandAdvances in PET: The Latest in Instrumentation, Technology, and Clinical PracticeBelum ada peringkat
- The Factors Affecting The Covid 19 Vaccine Acceptability To The Grade 12 Gas StudentsDokumen21 halamanThe Factors Affecting The Covid 19 Vaccine Acceptability To The Grade 12 Gas StudentsJane182004Belum ada peringkat
- Ockovaci CertifikatDokumen1 halamanOckovaci CertifikatEvaBelum ada peringkat
- Doh ProgramDokumen8 halamanDoh ProgramSheril Sularte CasanesBelum ada peringkat
- Ajnr 7 5 5Dokumen16 halamanAjnr 7 5 5Irma NugraheniBelum ada peringkat
- Enrolment Form: Delhi Public SchoolDokumen6 halamanEnrolment Form: Delhi Public SchoolMRITYUNJAY KUMARBelum ada peringkat
- OPT B1plus CLIL Units5-6 WorksheetDokumen2 halamanOPT B1plus CLIL Units5-6 WorksheetOksana ErmBelum ada peringkat
- VIII Science Sampel PaperDokumen4 halamanVIII Science Sampel PaperTaranjeet SinghBelum ada peringkat
- Travel Zoo Bangladesh LTD: 3 Star PackageDokumen2 halamanTravel Zoo Bangladesh LTD: 3 Star PackageRafan HussainBelum ada peringkat
- Research Proposal MatrixDokumen2 halamanResearch Proposal MatrixReuben Jr UmallaBelum ada peringkat
- Vol. 69, No. 02, February 2019Dokumen4 halamanVol. 69, No. 02, February 2019Rahma ArsytaBelum ada peringkat
- Term PaperDokumen8 halamanTerm Paperever mitcBelum ada peringkat
- Before You Leave 2013 Final VersionDokumen48 halamanBefore You Leave 2013 Final VersionMarthaConstantinouBelum ada peringkat
- Adult CardDokumen4 halamanAdult CardagelsantosBelum ada peringkat
- Medical Certificate For TravelDokumen5 halamanMedical Certificate For TravelAugust Cherry MabbyBelum ada peringkat
- FDA Briefing Document: Future Vaccination Regimens Addressing COVID-19Dokumen25 halamanFDA Briefing Document: Future Vaccination Regimens Addressing COVID-19Jackson SinnenbergBelum ada peringkat
- Syllabus EPIDokumen8 halamanSyllabus EPIOrlino PeterBelum ada peringkat
- Study: COVID Booster Effectiveness Wanes But Remains Strong: Credit: Unsplash/CC0 Public DomainDokumen2 halamanStudy: COVID Booster Effectiveness Wanes But Remains Strong: Credit: Unsplash/CC0 Public DomainShiny LuNaBelum ada peringkat
- Hubungan Tingkat Pengetahuan Kanker Serviks Dengan Minat Untuk Vaksinasi HPV Pada Mahasiswi Fakultas Kedokteran Universitas HKBP Nommensen MedanDokumen4 halamanHubungan Tingkat Pengetahuan Kanker Serviks Dengan Minat Untuk Vaksinasi HPV Pada Mahasiswi Fakultas Kedokteran Universitas HKBP Nommensen Medanintan fairuzBelum ada peringkat
- Research Article Assessment of Parents' Knowledge, Attitude and Practice About Child Vaccination in Rural AreasDokumen8 halamanResearch Article Assessment of Parents' Knowledge, Attitude and Practice About Child Vaccination in Rural AreaskrishnasreeBelum ada peringkat
- Immunization Outreach Form 2023Dokumen1 halamanImmunization Outreach Form 2023Ignatius KashumeBelum ada peringkat
- Text Book of Microbiology (221-330)Dokumen110 halamanText Book of Microbiology (221-330)Jamila ridaBelum ada peringkat
- Tetanus Toxoid Immunization Schedule For WomenDokumen4 halamanTetanus Toxoid Immunization Schedule For WomenEdwin Delos Reyes AbuBelum ada peringkat
- NCIRD - Immunization SchedulerDokumen3 halamanNCIRD - Immunization Schedulerramprasad.raghavanBelum ada peringkat