Anda mungkin juga menyukai
- Mathers Clinic Dysfunctional Attitude ScaleDokumen6 halamanMathers Clinic Dysfunctional Attitude ScaleGraça Maria Ferreira CarvalhoBelum ada peringkat
- Day 7-12 Rules For LifeDokumen26 halamanDay 7-12 Rules For LifeLuna DonjuánBelum ada peringkat
- International Personality Item Pool (English)Dokumen4 halamanInternational Personality Item Pool (English)Sami Ullah Khan Niazi100% (1)
- DersDokumen5 halamanDersbilliam123100% (1)
- Trauma Checklist (PCL-C)Dokumen4 halamanTrauma Checklist (PCL-C)Mayzie MayBelum ada peringkat
- Rosenfield & Mouzon (2013) - Gender and Mental HealthDokumen20 halamanRosenfield & Mouzon (2013) - Gender and Mental HealthAlejandro CBelum ada peringkat
- GE073DL GE7 Voyager ManualDokumen12 halamanGE073DL GE7 Voyager ManualEvan Schow100% (1)
- Psychodiagnostics Lab RecordsDokumen132 halamanPsychodiagnostics Lab Recordsdhanpati sahu100% (1)
- Ways of Coping Questionnaire WCQ ToadDokumen15 halamanWays of Coping Questionnaire WCQ ToadIeva BagataBelum ada peringkat
- Sroufe&Rutter1984. The Domain of Development PsychopathologyDokumen15 halamanSroufe&Rutter1984. The Domain of Development PsychopathologyAndrés EstradéBelum ada peringkat
- International Personality Item PoolDokumen3 halamanInternational Personality Item PoolVincent ChanBelum ada peringkat
- Mini Screen: P N: - D B: - D IDokumen2 halamanMini Screen: P N: - D B: - D IDaniel DascaluBelum ada peringkat
- Unit 18 Learning Aim ADokumen5 halamanUnit 18 Learning Aim Achristian dawitBelum ada peringkat
- MBTI - GenderDokumen2 halamanMBTI - GenderDianaCastleBelum ada peringkat
- NEO PI SummaryDokumen12 halamanNEO PI SummaryRoseNTolentinoBelum ada peringkat
- HBS107 AT1 Skills AuditDokumen5 halamanHBS107 AT1 Skills Auditcaleb mwanziaBelum ada peringkat
- HUMANISTIC PSYCHOLOGY: A NEW BREAK-THROUGHDokumen5 halamanHUMANISTIC PSYCHOLOGY: A NEW BREAK-THROUGHMarcelo Vial RoeheBelum ada peringkat
- Brief Screening Tool Detects Mild Cognitive ImpairmentDokumen5 halamanBrief Screening Tool Detects Mild Cognitive ImpairmentSarah Nova GradiskaBelum ada peringkat
- FSFI Questionnaire2000Dokumen5 halamanFSFI Questionnaire2000Dewi AsmalindaBelum ada peringkat
- Luyten2017 Parental Reflective FunctioningDokumen27 halamanLuyten2017 Parental Reflective FunctioningDiogo OliveiraBelum ada peringkat
- The Terman Merril TestDokumen4 halamanThe Terman Merril TestannatbBelum ada peringkat
- Recommended Test For Scientific Validity: AboutDokumen4 halamanRecommended Test For Scientific Validity: AboutivanquisherBelum ada peringkat
- Revista Mexicana de Trastornos Alimentarios Mexican Journal of Eating DisordersDokumen11 halamanRevista Mexicana de Trastornos Alimentarios Mexican Journal of Eating DisordersItzeel MtzBelum ada peringkat
- Project Title: Want To Be Successful?: Test Your AmbitionDokumen2 halamanProject Title: Want To Be Successful?: Test Your Ambitionibrahim mohamedBelum ada peringkat
- SPSI R BrochureDokumen2 halamanSPSI R BrochureNoreen Choudhri0% (1)
- Scoring the Adolescent Dissociative Experiences ScaleDokumen6 halamanScoring the Adolescent Dissociative Experiences ScaleКонстантин КрахмалевBelum ada peringkat
- PCASS 10 Item - 2-5itemsubscalesDokumen4 halamanPCASS 10 Item - 2-5itemsubscalesCyrene GarciaBelum ada peringkat
- ID The Window of Tolerance 20 06 16Dokumen12 halamanID The Window of Tolerance 20 06 16Ling Kang OngBelum ada peringkat
- Barrat ColombiaDokumen18 halamanBarrat ColombiaAntorcha CABelum ada peringkat
- Neo Ffi Reporte de Interpretacion PDFDokumen16 halamanNeo Ffi Reporte de Interpretacion PDFSalvador Machaca100% (1)
- Marital Satisfaction Scale analysis reliability validity Mexican supervisorsDokumen27 halamanMarital Satisfaction Scale analysis reliability validity Mexican supervisorsSantiago BohórquezBelum ada peringkat
- Rehabilitation Centre Helps Mental Patients ReintegrateDokumen8 halamanRehabilitation Centre Helps Mental Patients ReintegrateSaki Saki SakiBelum ada peringkat
- Introduction to Personality Theories and the Myers-Briggs Type Indicator (MBTIDokumen6 halamanIntroduction to Personality Theories and the Myers-Briggs Type Indicator (MBTIAiswarya VenkataramananBelum ada peringkat
- The Differentiation-Relatedness ScaleDokumen42 halamanThe Differentiation-Relatedness ScaleNatalia KopyakovaBelum ada peringkat
- Thought ControlDokumen3 halamanThought ControlJulianna Bartalus0% (1)
- The Influence of Bion On My Research (Rene Käes)Dokumen14 halamanThe Influence of Bion On My Research (Rene Käes)JuanOrtiz44Belum ada peringkat
- MMPI 2 y MCMI IIDokumen10 halamanMMPI 2 y MCMI IIErika Arroyo100% (1)
- WebpdfDokumen195 halamanWebpdf谭硕Belum ada peringkat
- The Mindful Attention Awareness Scale - TraitDokumen1 halamanThe Mindful Attention Awareness Scale - TraitMuhdHishamuddinBelum ada peringkat
- Asch, S. E., & Zukier, H. (1984) - Thinking About PersonsDokumen11 halamanAsch, S. E., & Zukier, H. (1984) - Thinking About PersonsGabriel Fernandes Camargo RosaBelum ada peringkat
- Emotion Regulation Taking Stock and Moving Forward (Gross, 2013)Dokumen7 halamanEmotion Regulation Taking Stock and Moving Forward (Gross, 2013)Rocío Donaire CortésBelum ada peringkat
- The EPQRDokumen1 halamanThe EPQRRayenne ENBelum ada peringkat
- Parental Attachment Questionnaire InsightsDokumen10 halamanParental Attachment Questionnaire InsightsajengBelum ada peringkat
- Evaluación Del Autoconcepto - Una Escala MultidimencionalDokumen20 halamanEvaluación Del Autoconcepto - Una Escala Multidimencionalyurit_020% (1)
- Wolgast (2014) : What Does The Acceptance and Action Questionnaire (AAQ-II) Really Measure?Dokumen9 halamanWolgast (2014) : What Does The Acceptance and Action Questionnaire (AAQ-II) Really Measure?Pablo Valencia MeléndezBelum ada peringkat
- Machiavellianism scale measures manipulationDokumen2 halamanMachiavellianism scale measures manipulationmanojBelum ada peringkat
- BprsDokumen7 halamanBprsamyljf100% (1)
- Hogan Flash ReportDokumen2 halamanHogan Flash Reportapi-382854758Belum ada peringkat
- PsycapDokumen21 halamanPsycapMirta YolandaBelum ada peringkat
- Modern Cave Living: Comforts of the PastDokumen4 halamanModern Cave Living: Comforts of the PastcarmenbergsancBelum ada peringkat
- A Life Position ScaleDokumen5 halamanA Life Position ScaleLatha Dona VenkatesanBelum ada peringkat
- Personality Assessment ScreenerDokumen11 halamanPersonality Assessment ScreenerMay-Anne VillamorBelum ada peringkat
- Emotional Intelligence Quiz Greater GoodDokumen1 halamanEmotional Intelligence Quiz Greater Goodapi-5139389010% (1)
- Apathy BI Asessment ToolsDokumen3 halamanApathy BI Asessment ToolsCarol ArtigasBelum ada peringkat
- Psychosis Screening QuestionnaireDokumen1 halamanPsychosis Screening QuestionnaireMeer Arsalan KhanBelum ada peringkat
- IPO-artikel MenningerBulletin 2009Dokumen17 halamanIPO-artikel MenningerBulletin 2009Feras ZidiBelum ada peringkat
- NEO PI-R Personality Assessment SummaryDokumen12 halamanNEO PI-R Personality Assessment Summaryanitnerol0% (1)
- Valorando La Psicopatología Desde Una Perspectiva Estructural, Un Modelo Psicodinámico BMCDokumen30 halamanValorando La Psicopatología Desde Una Perspectiva Estructural, Un Modelo Psicodinámico BMCDaypsiBelum ada peringkat
- Practical 2 UdpdDokumen11 halamanPractical 2 Udpdidonttttknowww1234567890Belum ada peringkat
- DomainsofPsychologicalAssessments Docx1Dokumen21 halamanDomainsofPsychologicalAssessments Docx1Sri Nurcahaya HabibaBelum ada peringkat
- Assessing The Structure of The Five Factor Model of Personality (IPIP-NEO-120) in The Public DomainDokumen16 halamanAssessing The Structure of The Five Factor Model of Personality (IPIP-NEO-120) in The Public DomainAcrismaritei BogdanBelum ada peringkat
- The Experiences in Close Relationship Scale (ECR) - Short Form: Reliability, Validity, and Factor StructureDokumen18 halamanThe Experiences in Close Relationship Scale (ECR) - Short Form: Reliability, Validity, and Factor Structurelobont nataliaBelum ada peringkat
- The COPE revised: Proposing a 5-factor model of coping strategiesDokumen36 halamanThe COPE revised: Proposing a 5-factor model of coping strategiesugur sayginBelum ada peringkat
- Social Psych Construct ValidationDokumen9 halamanSocial Psych Construct ValidationnilaBelum ada peringkat
- The Relationship Between Core Self Evaluations Individual Level Job Performance and Its ComponentsDokumen16 halamanThe Relationship Between Core Self Evaluations Individual Level Job Performance and Its ComponentsIAEME PublicationBelum ada peringkat
- Personal Inteligence StudyDokumen17 halamanPersonal Inteligence Studyrkocgana1975Belum ada peringkat
- A Nonlinear Mixed Model Framework For Item Response TheoryDokumen26 halamanA Nonlinear Mixed Model Framework For Item Response TheoryOscar Tlatempa NavaBelum ada peringkat
- Do Personality Scal Items Function Differently in People With High and Low IQDokumen11 halamanDo Personality Scal Items Function Differently in People With High and Low IQOscar Tlatempa NavaBelum ada peringkat
- Psychometric Properties of The Coping Inventory For Stressful Situations (CISS) in Patients With Acquired Brain Injury PDFDokumen9 halamanPsychometric Properties of The Coping Inventory For Stressful Situations (CISS) in Patients With Acquired Brain Injury PDFOscar Tlatempa NavaBelum ada peringkat
- El Uso Del Rio Oq45Dokumen5 halamanEl Uso Del Rio Oq45Manuel Enrique Ravanal Perez100% (1)
- Fobia SocialDokumen16 halamanFobia SocialJoseLuisRojasCiudadBelum ada peringkat
- Psychometric Properties of The Spanish Validation of The Five Facets of Mindfulness QuestionnaireDokumen9 halamanPsychometric Properties of The Spanish Validation of The Five Facets of Mindfulness QuestionnaireOscar Tlatempa NavaBelum ada peringkat
- Evaluación Del Acoso Psicológico en El Trabajo - Desarrollo y Estudio Exploratorio de Una Escala de MedidaDokumen12 halamanEvaluación Del Acoso Psicológico en El Trabajo - Desarrollo y Estudio Exploratorio de Una Escala de MedidaOscar Tlatempa NavaBelum ada peringkat
- An Abbreviated Version of The Brief Assessment of Cognition in SchizophreniaDokumen4 halamanAn Abbreviated Version of The Brief Assessment of Cognition in SchizophreniaOscar Tlatempa NavaBelum ada peringkat
- A Measurement Scale For Indecesiveness and Its Relationship To Career Indecision and Other Types of IndecisionDokumen10 halamanA Measurement Scale For Indecesiveness and Its Relationship To Career Indecision and Other Types of IndecisionOscar Tlatempa NavaBelum ada peringkat
- Reliability and Validity of The Persian Version of Templer Death Anxiety Scale-Extended in Veterans of Iran-Iraq Warfare PDFDokumen9 halamanReliability and Validity of The Persian Version of Templer Death Anxiety Scale-Extended in Veterans of Iran-Iraq Warfare PDFOscar Tlatempa NavaBelum ada peringkat
- A Measurement Scale For Indecesiveness and Its Relationship To Career Indecision and Other Types of IndecisionDokumen10 halamanA Measurement Scale For Indecesiveness and Its Relationship To Career Indecision and Other Types of IndecisionOscar Tlatempa NavaBelum ada peringkat
- A Comparison of Reliability and Construct Validity Between The Original and Revised Versions of The Rosenberg Self-Steem ScaleDokumen5 halamanA Comparison of Reliability and Construct Validity Between The Original and Revised Versions of The Rosenberg Self-Steem ScaleOscar Tlatempa NavaBelum ada peringkat
- A Compatison of Reliability and Construct Validity Between The Original and Revised Versions of The Rosenberg Self-Steem Scale PDFDokumen5 halamanA Compatison of Reliability and Construct Validity Between The Original and Revised Versions of The Rosenberg Self-Steem Scale PDFOscar Tlatempa NavaBelum ada peringkat
- CatR - An R Package For Computerized Adaptive TestingDokumen2 halamanCatR - An R Package For Computerized Adaptive TestingOscar Tlatempa NavaBelum ada peringkat
- Brief CV - RASHEDA AKHTAR (Edited)Dokumen3 halamanBrief CV - RASHEDA AKHTAR (Edited)Mossabber HossainBelum ada peringkat
- Healing Racial Trauma ResourcesDokumen4 halamanHealing Racial Trauma ResourcesZishan JiwaniBelum ada peringkat
- Tell Me About YourselfDokumen2 halamanTell Me About YourselfCjeanvaeb Dwynn ApidBelum ada peringkat
- Essay Competition 2022 QuestionsDokumen4 halamanEssay Competition 2022 QuestionsMaria Clara Machado CorrêaBelum ada peringkat
- Types of Amnesia Explained in DetailDokumen4 halamanTypes of Amnesia Explained in DetailHsnysbvBelum ada peringkat
- Nurse As EducatorDokumen28 halamanNurse As Educatornaelnael chaaBelum ada peringkat
- Case Study1 - Corporate GovernanceDokumen3 halamanCase Study1 - Corporate GovernanceCarmella DismayaBelum ada peringkat
- According To David Hawkins' in Power Vs Force - C.ymcdn - Com (PDFDrive)Dokumen12 halamanAccording To David Hawkins' in Power Vs Force - C.ymcdn - Com (PDFDrive)Jwan DelawiBelum ada peringkat
- ID Hubungan Antara Self Efficacy Dengan Bur PDFDokumen7 halamanID Hubungan Antara Self Efficacy Dengan Bur PDFIron PalayukanBelum ada peringkat
- Five Stages of Violent CrimeDokumen2 halamanFive Stages of Violent CrimeMuthamizh MaranBelum ada peringkat
- Federal Lawsuit Against Social Media CompaniesDokumen107 halamanFederal Lawsuit Against Social Media CompaniesBenjamin DuerBelum ada peringkat
- Sylabus TempDokumen6 halamanSylabus TempblairBelum ada peringkat
- Lawrence Green ModelDokumen5 halamanLawrence Green ModelarasoBelum ada peringkat
- Stress JournalDokumen2 halamanStress JournalYaba Brixzel F.Belum ada peringkat
- Early Childhood Development Iec Material DevelopmentDokumen22 halamanEarly Childhood Development Iec Material DevelopmentNAMANYA ASA MUHOOZIBelum ada peringkat
- Ped 101 Module 1314 Shara1Dokumen11 halamanPed 101 Module 1314 Shara1Shara mae BangeroBelum ada peringkat
- Course No: Hum 2224 Course Title: English Language Practice Assignment No: 01Dokumen2 halamanCourse No: Hum 2224 Course Title: English Language Practice Assignment No: 01Shoumik DassBelum ada peringkat
- Significance of Sex Education in Gen ZDokumen8 halamanSignificance of Sex Education in Gen ZIvan CapiralBelum ada peringkat
- Lesson 3: Reading A Text Critically: Unit 1: The Nature of Academic TextsDokumen22 halamanLesson 3: Reading A Text Critically: Unit 1: The Nature of Academic TextsHanna MendozaBelum ada peringkat
- User-Centered Lighting Solution for MigrainesDokumen48 halamanUser-Centered Lighting Solution for MigrainesMoon LightBelum ada peringkat
- My Portfolio in Work Immersion: University of Santo TomasDokumen7 halamanMy Portfolio in Work Immersion: University of Santo TomasKentfhil Mae AseronBelum ada peringkat
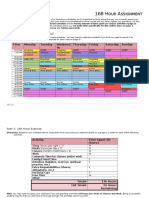
- 168 Hour Assignment Revised 2Dokumen3 halaman168 Hour Assignment Revised 2api-354712085Belum ada peringkat
- ApplicationList 934 Submitter 3 09 2023Dokumen6 halamanApplicationList 934 Submitter 3 09 2023Dr.PRABHA.RBelum ada peringkat
- PsychotherapyDokumen110 halamanPsychotherapyrovenBelum ada peringkat