Anda mungkin juga menyukai
- Endotracheal Intubation Learning MaterialDokumen8 halamanEndotracheal Intubation Learning MaterialLouie ParillaBelum ada peringkat
- Tonsillectomy 200829131303Dokumen102 halamanTonsillectomy 200829131303deptanaesaiimsgkpBelum ada peringkat
- Basic Airway Management in AdultsDokumen7 halamanBasic Airway Management in AdultsBereket temesgenBelum ada peringkat
- Airway ManagementDokumen28 halamanAirway ManagementghazyBelum ada peringkat
- Functional Endoscopic Sinus SurgeryDokumen11 halamanFunctional Endoscopic Sinus SurgeryIrene Natalia SihombingBelum ada peringkat
- ENDOTRACHEAL INTUBATIOn SandeepDokumen17 halamanENDOTRACHEAL INTUBATIOn SandeepSimran JosanBelum ada peringkat
- Tonsillectomy: Anatomy and PhysiologyDokumen5 halamanTonsillectomy: Anatomy and PhysiologyAgung Choro de Obes100% (1)
- Ear, Nose and Throat EmergenciesDokumen3 halamanEar, Nose and Throat Emergenciesfmta100% (1)
- Ent Explain Why and Short Notes by Shuvro DaDokumen37 halamanEnt Explain Why and Short Notes by Shuvro DaSumanBelum ada peringkat
- Surgical Treatment of Snoring & Obstructive Sleep Apnoea: Review ArticleDokumen10 halamanSurgical Treatment of Snoring & Obstructive Sleep Apnoea: Review ArticleSiddharth DhanarajBelum ada peringkat
- 03-Surgical Correction of Nasal ObstructionDokumen16 halaman03-Surgical Correction of Nasal ObstructionGloriaCorredorBelum ada peringkat
- RAPID SEQUENCE INTUBATION TECHNIQUEDokumen55 halamanRAPID SEQUENCE INTUBATION TECHNIQUElorkan19100% (1)
- Chapter 5 - Adenoidectomy: Suman GollaDokumen7 halamanChapter 5 - Adenoidectomy: Suman GollaGloriaCorredorBelum ada peringkat
- Tonsilectomy and AdenoidectomyDokumen7 halamanTonsilectomy and AdenoidectomySabella Gustika VernandaBelum ada peringkat
- OverviewDokumen3 halamanOverviewAngela MertesBelum ada peringkat
- E T IntubationDokumen15 halamanE T Intubationjtalan9Belum ada peringkat
- Ent Throat 1Dokumen58 halamanEnt Throat 1ميمونه عبدالرحيم مصطفىBelum ada peringkat
- Basic Airway ManagementDokumen24 halamanBasic Airway ManagementFELIPE MEDINABelum ada peringkat
- Local Anaesthetic Thoracoscopy For Intractable Pneumothorax in A High-Risk PatientDokumen2 halamanLocal Anaesthetic Thoracoscopy For Intractable Pneumothorax in A High-Risk PatientUkh ChyBelum ada peringkat
- NEJM VICM Viewers ChoiceDokumen19 halamanNEJM VICM Viewers ChoiceAnonymous cQWavnBelum ada peringkat
- Occurs Most Often In:: Muscular DystrophyDokumen4 halamanOccurs Most Often In:: Muscular DystrophyJiezl Abellano AfinidadBelum ada peringkat
- Overview of TonsillectomyDokumen8 halamanOverview of TonsillectomyMaya PutriBelum ada peringkat
- Functional Endoscopic Sinus Surgery - Overview, Preparation, TechniqueDokumen10 halamanFunctional Endoscopic Sinus Surgery - Overview, Preparation, TechniqueHendra SusantoBelum ada peringkat
- Final Content ET Intubation 1Dokumen27 halamanFinal Content ET Intubation 1Debipriya MistryBelum ada peringkat
- Choanal Atresia1Dokumen5 halamanChoanal Atresia1anurajoneBelum ada peringkat
- Surgical Options for Treating Obstructive Sleep ApneaDokumen37 halamanSurgical Options for Treating Obstructive Sleep ApneaAlbert GheorgheBelum ada peringkat
- Bronchospasm During Anaesthesia Update 2011Dokumen5 halamanBronchospasm During Anaesthesia Update 2011hy3pjb1984Belum ada peringkat
- Deviated Nasal SeptumDokumen15 halamanDeviated Nasal SeptumSrinivas Sukhavasi50% (2)
- Basic Airway Management in Adults - UpToDateDokumen28 halamanBasic Airway Management in Adults - UpToDateGia Villavicencio BoniniBelum ada peringkat
- TracheostomyDokumen4 halamanTracheostomymindreader19Belum ada peringkat
- File 18584Dokumen12 halamanFile 18584Mohammed MuthanaBelum ada peringkat
- EPISTAXIS LectureDokumen30 halamanEPISTAXIS LectureDhienWhieBelum ada peringkat
- Pneumothorax, Tension and TraumaticDokumen24 halamanPneumothorax, Tension and TraumaticSatria WibawaBelum ada peringkat
- Airway and Ventilatory ManagementDokumen8 halamanAirway and Ventilatory ManagementAshen DissanayakaBelum ada peringkat
- Endotracheal TubeDokumen19 halamanEndotracheal TubeSarvess Muniandy100% (1)
- Airway Management: Intensive Care Unit, Prince of Wales Hospital, Chinese University of Hong KongDokumen9 halamanAirway Management: Intensive Care Unit, Prince of Wales Hospital, Chinese University of Hong KongErwinRamadhaniBelum ada peringkat
- Maxillofacial Trauma: Dr. Azher A. Auda Bds CabsDokumen17 halamanMaxillofacial Trauma: Dr. Azher A. Auda Bds CabsHaider F YehyaBelum ada peringkat
- Nursing DiagnosisDokumen4 halamanNursing DiagnosisKrizzia CarlosBelum ada peringkat
- AnesthesiaDokumen42 halamanAnesthesiauzma aijazBelum ada peringkat
- Paediatric TonsillectomyDokumen9 halamanPaediatric TonsillectomyAlbert GheorgheBelum ada peringkat
- EPISTAXIS-bleeding From The Nose (Most Common) Etiology (Cause)Dokumen34 halamanEPISTAXIS-bleeding From The Nose (Most Common) Etiology (Cause)Julliza Joy PandiBelum ada peringkat
- 16 Complications in Anaesthesia PDFDokumen0 halaman16 Complications in Anaesthesia PDFjuniorebindaBelum ada peringkat
- TonsillectomyDokumen27 halamanTonsillectomyRho Vince Caño MalagueñoBelum ada peringkat
- Complications of Endotracheal Intubation and Other Airway Management ProceduresDokumen11 halamanComplications of Endotracheal Intubation and Other Airway Management ProceduresSuresh Kumar100% (1)
- Complications of Endotracheal Intubation and Other Airway Management ProceduresDokumen11 halamanComplications of Endotracheal Intubation and Other Airway Management ProceduresashajangamBelum ada peringkat
- Otitis Media AkutDokumen30 halamanOtitis Media Akutindah sariBelum ada peringkat
- Anatomy of Nasopharynx & AdenoidsDokumen3 halamanAnatomy of Nasopharynx & AdenoidsAmy KochBelum ada peringkat
- Airway TraumaDokumen73 halamanAirway TraumaSarah BirechBelum ada peringkat
- General Anesthesia Intubation GuideDokumen44 halamanGeneral Anesthesia Intubation GuideMiezu CosminBelum ada peringkat
- Airway ManagementDokumen11 halamanAirway Managementmegayani santosoBelum ada peringkat
- Intubation: ProcedureDokumen2 halamanIntubation: ProcedureKat AlaBelum ada peringkat
- Anaesthesia.: IV Induction Agents AreDokumen4 halamanAnaesthesia.: IV Induction Agents AreUzma KhanBelum ada peringkat
- Surgical Nursing (III)Dokumen32 halamanSurgical Nursing (III)Opio MosesBelum ada peringkat
- Managing NosebleedsDokumen7 halamanManaging NosebleedsHasbiallah YusufBelum ada peringkat
- Epistaxis: Ms. Shital BhutkarDokumen37 halamanEpistaxis: Ms. Shital BhutkarSuhas IngaleBelum ada peringkat
- Airway Obstruction Final2Dokumen33 halamanAirway Obstruction Final2Mahindra KumarBelum ada peringkat
- Key Notes Adapted From Smeltzer Medical Surgical Nursing 11 EditionDokumen5 halamanKey Notes Adapted From Smeltzer Medical Surgical Nursing 11 EditionKarla LopezBelum ada peringkat
- Diagnosis and Treatment of Neurogenic Oropharyngeal DysphagiaDari EverandDiagnosis and Treatment of Neurogenic Oropharyngeal DysphagiaBelum ada peringkat
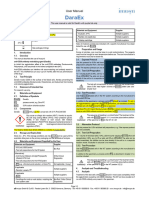
- Imusyn DaraEx v21.1 EN RUODokumen2 halamanImusyn DaraEx v21.1 EN RUONedelcu CarmenBelum ada peringkat
- Medical Assistant Grades Need ClarificationDokumen1 halamanMedical Assistant Grades Need ClarificationNedelcu CarmenBelum ada peringkat
- Images Ems AirwaytodayDokumen42 halamanImages Ems AirwaytodayNedelcu CarmenBelum ada peringkat
- Br. J. Anaesth.-1968-WATERS-259-64Dokumen6 halamanBr. J. Anaesth.-1968-WATERS-259-64Nedelcu CarmenBelum ada peringkat
- ANES2014 Abstract Guide OnlineDokumen169 halamanANES2014 Abstract Guide OnlineNedelcu Carmen0% (1)
- Medical Assistant Grades Need ClarificationDokumen1 halamanMedical Assistant Grades Need ClarificationNedelcu CarmenBelum ada peringkat
- Airway 19 9 11Dokumen49 halamanAirway 19 9 11Nedelcu CarmenBelum ada peringkat
- Difficult Airway ManagementDokumen78 halamanDifficult Airway ManagementNedelcu Carmen100% (1)
- Chicago Case InterviewsDokumen20 halamanChicago Case Interviewschakradhar.dandu@gmail.comBelum ada peringkat
- Soal EnglishDokumen7 halamanSoal EnglishRieZky RamadhaniBelum ada peringkat
- q4 Mapeh 7 WHLP Leap S.test w1 w8 MagsinoDokumen39 halamanq4 Mapeh 7 WHLP Leap S.test w1 w8 MagsinoFatima11 MagsinoBelum ada peringkat
- Pan or The DevilDokumen8 halamanPan or The DevilMarguerite and Leni Johnson100% (1)
- Strategy Map - Visualize Goals & ObjectivesDokumen22 halamanStrategy Map - Visualize Goals & ObjectivesNitin JainBelum ada peringkat
- Ore Pass Design and Placement Koivisto Mikko PDFDokumen105 halamanOre Pass Design and Placement Koivisto Mikko PDFasepdayat100% (1)
- Updated Syllabus - ME CSE Word Document PDFDokumen62 halamanUpdated Syllabus - ME CSE Word Document PDFGayathri R HICET CSE STAFFBelum ada peringkat
- 2004 Swamee, Prabhata K. Rathie, Pushpa N. - Exact Solutions For Normal Depth ProblemDokumen9 halaman2004 Swamee, Prabhata K. Rathie, Pushpa N. - Exact Solutions For Normal Depth Problemjosue.angelo9459Belum ada peringkat
- Psychological Assessment Chapter 4 - of Tests and Testing PDFDokumen7 halamanPsychological Assessment Chapter 4 - of Tests and Testing PDFSam CruzBelum ada peringkat
- Computerised Accounting SystemDokumen14 halamanComputerised Accounting SystemramneekdadwalBelum ada peringkat
- RLE107MCF - REVISED Case Study (OB - CENTERED) (Henderson A - Group 1)Dokumen37 halamanRLE107MCF - REVISED Case Study (OB - CENTERED) (Henderson A - Group 1)Abigail RegaladoBelum ada peringkat
- Academic TranscriptDokumen6 halamanAcademic Transcriptapi-450491493Belum ada peringkat
- Internship ReportDokumen24 halamanInternship ReportFaiz KhanBelum ada peringkat
- Women &literatureDokumen54 halamanWomen &literatureAicha ZianeBelum ada peringkat
- Ashida Relay Operating ManualDokumen16 halamanAshida Relay Operating ManualVivek Kakkoth100% (1)
- CANON KABUSHIKI KAISHA vs. COURT OF APPEALSDokumen2 halamanCANON KABUSHIKI KAISHA vs. COURT OF APPEALSJUAN REINO CABITACBelum ada peringkat
- DeVry ACCT 505 Final Exam 2Dokumen12 halamanDeVry ACCT 505 Final Exam 2devryfinalexamscomBelum ada peringkat
- Quantum Mechanics and PeriodicityDokumen51 halamanQuantum Mechanics and Periodicitynxumalopat2Belum ada peringkat
- Homework #3 - Coursera CorrectedDokumen10 halamanHomework #3 - Coursera CorrectedSaravind67% (3)
- Raa' - Tafkheem & Tarqeeq - Tajweed MeDokumen11 halamanRaa' - Tafkheem & Tarqeeq - Tajweed MeClass DocumentBelum ada peringkat
- Ning™: The Six Cs of Effective MessagesDokumen40 halamanNing™: The Six Cs of Effective MessagestbnjhjlkkkkkkBelum ada peringkat
- UBD PlantDokumen8 halamanUBD PlantMahmoud DibBelum ada peringkat
- Chap 006Dokumen50 halamanChap 006Martin TrịnhBelum ada peringkat
- Person On The StreetDokumen12 halamanPerson On The StreetalyssajdorazioBelum ada peringkat
- How The Government Was Formed After Prophet MuhammadDokumen48 halamanHow The Government Was Formed After Prophet MuhammadMUSALMAN BHAIBelum ada peringkat
- G11 F2F ScheduleDokumen3 halamanG11 F2F ScheduleQueenie Marie Obial AlasBelum ada peringkat
- Letters and Treaties by Mohammad PBUH-3 PDFDokumen19 halamanLetters and Treaties by Mohammad PBUH-3 PDFAbdulaziz Khattak Abu FatimaBelum ada peringkat
- Prambanan Temple LegendDokumen1 halamanPrambanan Temple LegendClara NadaBelum ada peringkat
- Grade 8 Lesson on "The Filipino is Worth Dying ForDokumen5 halamanGrade 8 Lesson on "The Filipino is Worth Dying ForHanna ManiteBelum ada peringkat
- Comparative Summary of 5 Learning TheoriesDokumen2 halamanComparative Summary of 5 Learning TheoriesMonique Gabrielle Nacianceno AalaBelum ada peringkat