Anda mungkin juga menyukai
- Motions, Affidavits, Answers, and Commercial Liens - The Book of Effective Sample DocumentsDari EverandMotions, Affidavits, Answers, and Commercial Liens - The Book of Effective Sample DocumentsPenilaian: 4.5 dari 5 bintang4.5/5 (13)
- Sniper2 mq4Dokumen8 halamanSniper2 mq4Juraizam Fazlen JafarBelum ada peringkat
- DSWD - Forms For Minors Travelling ABroadDokumen3 halamanDSWD - Forms For Minors Travelling ABroadKAKKAMPI92% (62)
- WWW - Passport.gc - CA Form Pdfs Pptc153Dokumen7 halamanWWW - Passport.gc - CA Form Pdfs Pptc153Rob GchukBelum ada peringkat
- Axa Travel Claims Form Uae 1.1Dokumen1 halamanAxa Travel Claims Form Uae 1.1Baptiste ElliasBelum ada peringkat
- Supplementary Join Family Application Form: New Delhi Visa Office, Embassy of IrelandDokumen6 halamanSupplementary Join Family Application Form: New Delhi Visa Office, Embassy of Irelandkalligadu_143Belum ada peringkat
- Family Health Questionnaire Form (FHQ) : Allianz EFU Health Insurance Limited Window Takaful OperationsDokumen2 halamanFamily Health Questionnaire Form (FHQ) : Allianz EFU Health Insurance Limited Window Takaful OperationsnomiabbasiBelum ada peringkat
- Claim Form AustraliaDokumen8 halamanClaim Form AustraliarosemcdoBelum ada peringkat
- Travel Claim Form (NEW)Dokumen5 halamanTravel Claim Form (NEW)HihiBelum ada peringkat
- Fogg Travel Insurance Medical Expenses Claim FormDokumen3 halamanFogg Travel Insurance Medical Expenses Claim FormDiana PanteaBelum ada peringkat
- Fogg Travel Insurance Services Limited: Personal Liability Claim FormDokumen2 halamanFogg Travel Insurance Services Limited: Personal Liability Claim FormDiana PanteaBelum ada peringkat
- Commonwealth of Australia Statutory Declaration: Purpose of This Form For More InformationDokumen4 halamanCommonwealth of Australia Statutory Declaration: Purpose of This Form For More InformationOm KarnBelum ada peringkat
- Claim Form 1Dokumen14 halamanClaim Form 1Michael MandlerBelum ada peringkat
- D StatmentDokumen8 halamanD StatmentHihiBelum ada peringkat
- STARR Travel Insurance Application FormDokumen1 halamanSTARR Travel Insurance Application Formsheila coloradaBelum ada peringkat
- NTUC Pa Paid Claim Form (08 2017)Dokumen5 halamanNTUC Pa Paid Claim Form (08 2017)pat5355Belum ada peringkat
- Apply for funding with ID numberDokumen2 halamanApply for funding with ID numberThubelihle HadebeBelum ada peringkat
- Claimant's Statement FormDokumen2 halamanClaimant's Statement FormRiza Zausa CuarteroBelum ada peringkat
- Application - Regency For Expats Essential FullDokumen2 halamanApplication - Regency For Expats Essential FullLucas GomezBelum ada peringkat
- Health Statement FormDokumen2 halamanHealth Statement FormRose Ann DuqueBelum ada peringkat
- HSBC - Guranteed Pricing SchemeDokumen4 halamanHSBC - Guranteed Pricing SchemekrishkpeBelum ada peringkat
- Consent To Grant An Australian Visa To A Child Under The Age of 18 YearsDokumen4 halamanConsent To Grant An Australian Visa To A Child Under The Age of 18 YearsStefani Hermione WindaBelum ada peringkat
- Apply for funding with IDDokumen2 halamanApply for funding with IDAmanda MalingaBelum ada peringkat
- Nomination Form-NCT - 29th October-22Dokumen2 halamanNomination Form-NCT - 29th October-22pmBelum ada peringkat
- Claimant'S Statement - Death ClaimDokumen2 halamanClaimant'S Statement - Death ClaimChristian DazaBelum ada peringkat
- Vision Benefits Claim Form: To Be Completed by The CardholderDokumen2 halamanVision Benefits Claim Form: To Be Completed by The CardholderSam DipBelum ada peringkat
- Apply Birth Certificate OnlineDokumen2 halamanApply Birth Certificate OnlineLAJOVI COMPUTERSBelum ada peringkat
- Travel Claim FormDokumen9 halamanTravel Claim Formraokirtan6Belum ada peringkat
- Activity Permission SlipDokumen1 halamanActivity Permission SlipchristiehobsonBelum ada peringkat
- NZ Police Vetting Service Request and Consent Form - 1Dokumen5 halamanNZ Police Vetting Service Request and Consent Form - 1Kenny XBelum ada peringkat
- College CFDokumen2 halamanCollege CFPeter IgnacioBelum ada peringkat
- SLOCPI Death Claimant Statement 10may2016 2Dokumen3 halamanSLOCPI Death Claimant Statement 10may2016 2Marc Benedict TalamayanBelum ada peringkat
- Horizon Medical Health Insurance Claim Form: Please Read This Important InformationDokumen2 halamanHorizon Medical Health Insurance Claim Form: Please Read This Important InformationBrianReagerBelum ada peringkat
- OMA OM en Claims TravelDelayDokumen4 halamanOMA OM en Claims TravelDelayreshwan aliBelum ada peringkat
- Optima Restore Proposal Form OfflineDokumen9 halamanOptima Restore Proposal Form OfflinemanohargudBelum ada peringkat
- Form I National Cadet Corps SENIOR DIVISION/WING ENROLMENT FORM (See Rules 7 and 11 of NCC Act 1948)Dokumen8 halamanForm I National Cadet Corps SENIOR DIVISION/WING ENROLMENT FORM (See Rules 7 and 11 of NCC Act 1948)Suresh Sankara NarayananBelum ada peringkat
- Regency For Expats - Essential Health - Application FormDokumen2 halamanRegency For Expats - Essential Health - Application FormGuillaume VingtcentBelum ada peringkat
- Hospital Admission Application Form and Declaration FormDokumen2 halamanHospital Admission Application Form and Declaration Formelmore kakaBelum ada peringkat
- 11 State of New Hampshire Petition For AdoptionDokumen3 halaman11 State of New Hampshire Petition For AdoptionMarcus Skookumchuck VanniniBelum ada peringkat
- Ir595d 2019Dokumen2 halamanIr595d 2019Fuckyou I'mnotsubscribingBelum ada peringkat
- Birth Affidavit: Last Suffix First MiddleDokumen2 halamanBirth Affidavit: Last Suffix First Middlesidiki millimonoBelum ada peringkat
- Affivadit CSGDokumen1 halamanAffivadit CSGjeswynnemartin67Belum ada peringkat
- Accident/Hospital Indemnity Wellness Benefit Claim Form: CW 061999 Page 1 of 2 02/14Dokumen2 halamanAccident/Hospital Indemnity Wellness Benefit Claim Form: CW 061999 Page 1 of 2 02/14Stam AnBelum ada peringkat
- BooksDokumen7 halamanBooksHITMANLEGEND LimitedBelum ada peringkat
- Embassy of India-1C New Born Baby Passport FormDokumen5 halamanEmbassy of India-1C New Born Baby Passport Formpl_rajaBelum ada peringkat
- Group Insurance ApplicationDokumen1 halamanGroup Insurance Applicationジョン ジーBelum ada peringkat
- Change Name Adult Over 18 YearsDokumen7 halamanChange Name Adult Over 18 Yearssjsmith03051968Belum ada peringkat
- WestJet ReligiousExemption-Form enDokumen4 halamanWestJet ReligiousExemption-Form enDean AminBelum ada peringkat
- Personal Accident Claim Form: Particulars of Insured (Company / Individual)Dokumen2 halamanPersonal Accident Claim Form: Particulars of Insured (Company / Individual)Robbie Chan100% (1)
- CA APP Blank FormDokumen4 halamanCA APP Blank FormChristine Irish GoyenaBelum ada peringkat
- PPTC 153Dokumen7 halamanPPTC 153filipamaltezBelum ada peringkat
- Agreement Pertaining To Loss or Destruction of PolicyDokumen2 halamanAgreement Pertaining To Loss or Destruction of PolicyjedBelum ada peringkat
- Personal Accident InsuranceDokumen3 halamanPersonal Accident InsuranceSwiftBelum ada peringkat
- 1.5 Star Learners Centre Registration Form Vmar 2023Dokumen4 halaman1.5 Star Learners Centre Registration Form Vmar 2023Brandon TanBelum ada peringkat
- UM - Service Waiver Form - 20210828Dokumen1 halamanUM - Service Waiver Form - 20210828Unique Toys CollectionBelum ada peringkat
- Refund Request: Home Page General Enquiry LineDokumen6 halamanRefund Request: Home Page General Enquiry LineJamal BukhariBelum ada peringkat
- Cancellation of Removal for Lawful Permanent ResidentsDari EverandCancellation of Removal for Lawful Permanent ResidentsBelum ada peringkat
- A Safe and Sensible Return To Work For Essential WorkersDokumen2 halamanA Safe and Sensible Return To Work For Essential WorkersPat NolanBelum ada peringkat
- Table of RestrictionsDokumen4 halamanTable of RestrictionsPat NolanBelum ada peringkat
- Recommendation For Lake WendoureeDokumen56 halamanRecommendation For Lake WendoureePat NolanBelum ada peringkat
- Pandemic Code Brown To Support HospitalsDokumen1 halamanPandemic Code Brown To Support HospitalsPat NolanBelum ada peringkat
- 8.16. Advisory Committees Division: Director: Author/Position: Sophie Constable - Administration Officer StatutoryDokumen268 halaman8.16. Advisory Committees Division: Director: Author/Position: Sophie Constable - Administration Officer StatutoryPat NolanBelum ada peringkat
- RestrictionsDokumen6 halamanRestrictionsPat Nolan100% (1)
- More Freedoms To Come As Victoria Hits 90 Per Cent Vax RateDokumen2 halamanMore Freedoms To Come As Victoria Hits 90 Per Cent Vax RatePat NolanBelum ada peringkat
- Keeping Victorian Workers in Key Sectors SafeDokumen2 halamanKeeping Victorian Workers in Key Sectors SafePat NolanBelum ada peringkat
- EcologyofthePlatypus PosterDokumen1 halamanEcologyofthePlatypus PosterPat NolanBelum ada peringkat
- Ballarat ELS Final Draft 31 July 2021Dokumen182 halamanBallarat ELS Final Draft 31 July 2021Pat NolanBelum ada peringkat
- Following The Three Vs For A Safe Return To SchoolDokumen2 halamanFollowing The Three Vs For A Safe Return To SchoolPat NolanBelum ada peringkat
- 23 June 2021 Council Meeting Agenda With Attachments - Part 1Dokumen223 halaman23 June 2021 Council Meeting Agenda With Attachments - Part 1Pat NolanBelum ada peringkat
- Regional RoadmapDokumen11 halamanRegional RoadmapKyra GillespieBelum ada peringkat
- CB Booklet 20 SEP 21Dokumen19 halamanCB Booklet 20 SEP 21Pat NolanBelum ada peringkat
- Table of RestrictionsDokumen12 halamanTable of RestrictionsPat Nolan100% (1)
- Restriction ChangesDokumen8 halamanRestriction ChangesPat NolanBelum ada peringkat
- Table of Restrictions, Released June 2, 2021Dokumen9 halamanTable of Restrictions, Released June 2, 2021Pat NolanBelum ada peringkat
- Leawarra Neighbourhood Delacombe Draft MasterplanDokumen12 halamanLeawarra Neighbourhood Delacombe Draft MasterplanPat NolanBelum ada peringkat
- Anthony Prebble Murder Coverage in The CourierDokumen10 halamanAnthony Prebble Murder Coverage in The CourierPat NolanBelum ada peringkat
- 7 Day Circuit Breaker RestrictionsDokumen7 halaman7 Day Circuit Breaker RestrictionsPat NolanBelum ada peringkat
- SKM Ballarat Heritage ValueDokumen117 halamanSKM Ballarat Heritage ValuePat NolanBelum ada peringkat
- Table of RestrictionsDokumen4 halamanTable of RestrictionsPat NolanBelum ada peringkat
- Table of RestrictionsDokumen5 halamanTable of RestrictionsPat NolanBelum ada peringkat
- 2021 AEC Victoria A4 Hawke ProposedDokumen1 halaman2021 AEC Victoria A4 Hawke ProposedPat NolanBelum ada peringkat
- WVTNP Corridors Map February 2021Dokumen1 halamanWVTNP Corridors Map February 2021Pat NolanBelum ada peringkat
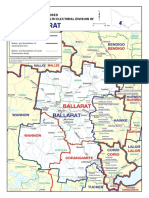
- 2021 AEC Victoria A4 Ballarat ProposedDokumen1 halaman2021 AEC Victoria A4 Ballarat ProposedPat NolanBelum ada peringkat
- WVTNP Corridors Map February 2021Dokumen1 halamanWVTNP Corridors Map February 2021Pat NolanBelum ada peringkat
- 27 January 2021 Council Meeting Agenda With Attachments - Part1Dokumen114 halaman27 January 2021 Council Meeting Agenda With Attachments - Part1Pat NolanBelum ada peringkat
- Confidential: Governance & Culture ReviewDokumen60 halamanConfidential: Governance & Culture ReviewPat NolanBelum ada peringkat
- Sovereign Hill Masterplan Executive Summary LR WebDokumen36 halamanSovereign Hill Masterplan Executive Summary LR WebPat NolanBelum ada peringkat
- A Self-help App for Syrian Refugees with PTSDDokumen51 halamanA Self-help App for Syrian Refugees with PTSDMiguel SobredoBelum ada peringkat
- Qad Erp Solutions GuideDokumen121 halamanQad Erp Solutions GuideLuis LezamaBelum ada peringkat
- Ujian SPSS TatiDokumen21 halamanUjian SPSS TatiLina NaiwaBelum ada peringkat
- Narrow Band Powerline Communication Module With Simple MAC User Narrow Band Powerline Communication Module With Simple MAC User Manual Narrow Band Powerline CommunicationDokumen8 halamanNarrow Band Powerline Communication Module With Simple MAC User Narrow Band Powerline Communication Module With Simple MAC User Manual Narrow Band Powerline CommunicationAle NqnBelum ada peringkat
- PrefaceDokumen2 halamanPrefaceAKSBelum ada peringkat
- ISO27001:2013 Information Technology, Security Techniques & Management Systems Self Assessment ChecklistDokumen23 halamanISO27001:2013 Information Technology, Security Techniques & Management Systems Self Assessment Checklistmilind2100675% (4)
- AWS Simple-Icons v2.0Dokumen10 halamanAWS Simple-Icons v2.0jonbaerBelum ada peringkat
- Ecological Bin Packing SolutionDokumen2 halamanEcological Bin Packing SolutionHello misterBelum ada peringkat
- IEWB-RS Technology Labs Eigrp: Brian Dennis, CCIE # 2210 (R&S / ISP Dial / Security / Service Provider)Dokumen51 halamanIEWB-RS Technology Labs Eigrp: Brian Dennis, CCIE # 2210 (R&S / ISP Dial / Security / Service Provider)Nandan BishtBelum ada peringkat
- LDA KNN LogisticDokumen29 halamanLDA KNN Logisticshruti gujar100% (1)
- Top Deals on OnePlus MobilesDokumen8 halamanTop Deals on OnePlus MobilesParinita PariharBelum ada peringkat
- A Simple and Effective Method For Filling Gaps in Landsat ETM+ SLC-off ImagesDokumen12 halamanA Simple and Effective Method For Filling Gaps in Landsat ETM+ SLC-off ImagesJanos HidiBelum ada peringkat
- Certified Ethical Hacker: Ceh V10Dokumen10 halamanCertified Ethical Hacker: Ceh V10Pragati sisodiyaBelum ada peringkat
- 2016-Db-Nigel Bayliss-The Oracle Optimizer - Upgrading Without Pain-PraesentationDokumen64 halaman2016-Db-Nigel Bayliss-The Oracle Optimizer - Upgrading Without Pain-Praesentationsmishra_97Belum ada peringkat
- 436Dokumen18 halaman436Nikhil Sharma MadhuBelum ada peringkat
- Ergonomic Analysis of Motor VehiclesDokumen14 halamanErgonomic Analysis of Motor VehiclesdeyeBelum ada peringkat
- Request For ProposalDokumen216 halamanRequest For ProposalGilbert KamanziBelum ada peringkat
- Book S Curve For Construction Sample Excel Bing PDFDokumen4 halamanBook S Curve For Construction Sample Excel Bing PDFmy.nafi.pmp5283Belum ada peringkat
- Ht905ta-Al 5B1 5d.dirndlk lh-t778hts DeilamiDokumen25 halamanHt905ta-Al 5B1 5d.dirndlk lh-t778hts DeilamifatiBelum ada peringkat
- 22a Um001e en eDokumen108 halaman22a Um001e en eNelson ContrerasBelum ada peringkat
- C 680 - 03 Qzy4mc0wmwDokumen16 halamanC 680 - 03 Qzy4mc0wmwB rgBelum ada peringkat
- Wimax System Performance StudiesDokumen10 halamanWimax System Performance StudiesFelix GatambiaBelum ada peringkat
- SQLDokumen71 halamanSQLDrKrishna Priya ChakireddyBelum ada peringkat
- I, Robot - Future (Will)Dokumen2 halamanI, Robot - Future (Will)CarolinaDeCastroCerviBelum ada peringkat
- Install Ansible On Mac OSXDokumen5 halamanInstall Ansible On Mac OSXNagendraBelum ada peringkat
- Deck Machinery BrochureDokumen18 halamanDeck Machinery BrochureSigit Yoga PBelum ada peringkat
- Thesis Progress TrackerDokumen4 halamanThesis Progress Trackerheatherbeninatianchorage100% (2)
- FPGA Xilin XcellDokumen68 halamanFPGA Xilin XcellJustin JenningsBelum ada peringkat
- TM-T20X Utility - Setting Utility For Products - Thermal Line Printer - Download - POS - EpsonDokumen1 halamanTM-T20X Utility - Setting Utility For Products - Thermal Line Printer - Download - POS - EpsonVictor HenriqueBelum ada peringkat