Anda mungkin juga menyukai
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
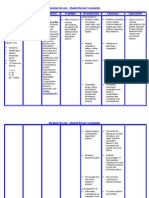
- NURSING CARE PLAN - Liver CirrhosisDokumen2 halamanNURSING CARE PLAN - Liver Cirrhosisderic100% (27)
- The Psychology of Pain: George R. Hansen, MD, Jon Streltzer, MDDokumen10 halamanThe Psychology of Pain: George R. Hansen, MD, Jon Streltzer, MDRobi Maulana100% (1)
- Visual ImpairmentDokumen7 halamanVisual ImpairmentShirley Briagas50% (2)
- Acid Base Balance Pathophysiology NursingDokumen7 halamanAcid Base Balance Pathophysiology Nursinggrad_nurse_2015100% (2)
- High Risk NewbornDokumen20 halamanHigh Risk Newborndmrdy50% (2)
- Diabetes & Clinic Organisation ENGDokumen28 halamanDiabetes & Clinic Organisation ENGdrsaleemBelum ada peringkat
- Denham Fatigue Facilitator's ManualDokumen27 halamanDenham Fatigue Facilitator's Manualsergentul -Belum ada peringkat
- Catatonia Revived. A Unique Syndrome UpdatedDokumen10 halamanCatatonia Revived. A Unique Syndrome UpdatedElisa PavezBelum ada peringkat
- Digestive Care - ADVEN BIOTECH GURGAONDokumen7 halamanDigestive Care - ADVEN BIOTECH GURGAONmljaininsulationBelum ada peringkat
- 12b1705 Andrographis Paniculata SambilotoDokumen2 halaman12b1705 Andrographis Paniculata Sambilotofajar1987Belum ada peringkat
- Nutrition For HoneyDokumen13 halamanNutrition For Honeydrsnair78Belum ada peringkat
- Answer Key Practice NeuroDokumen11 halamanAnswer Key Practice NeuroAnonymous iG0DCOfBelum ada peringkat
- Age ( 55 Years Old) - Female Sex - BMI: 28 (Overweight) - Alcohol Consumption - Uncontrolled Hypertension - High Fat DietDokumen3 halamanAge ( 55 Years Old) - Female Sex - BMI: 28 (Overweight) - Alcohol Consumption - Uncontrolled Hypertension - High Fat DietelleBelum ada peringkat
- Unit 11 Role of Fungi in Human Welfare: ObjectivesDokumen12 halamanUnit 11 Role of Fungi in Human Welfare: Objectivessivaram888Belum ada peringkat
- Hypolipidemic DrugsDokumen5 halamanHypolipidemic Drugsapi-3810976Belum ada peringkat
- Edema: Ahammed Naseem Roll No: 3 Second Year BSC Nursing Al-Mas College of NursingDokumen24 halamanEdema: Ahammed Naseem Roll No: 3 Second Year BSC Nursing Al-Mas College of NursingNaseem Bin YoosafBelum ada peringkat
- Chapter 33: Atopic, Rheumatic, and Immunodeficiency Disorders Garzon Maaks: Burns' Pediatric Primary Care, 7th EditionDokumen8 halamanChapter 33: Atopic, Rheumatic, and Immunodeficiency Disorders Garzon Maaks: Burns' Pediatric Primary Care, 7th EditionHelen UgochukwuBelum ada peringkat
- CatalogDokumen212 halamanCataloggeoffismBelum ada peringkat
- 03 Handout 1Dokumen9 halaman03 Handout 1genesis nadonggaBelum ada peringkat
- Scleroderma: Bagian Ilmu Kesehatan Kulit Dan Kelamin Fakultas Kedokteran Universitas Pattimura Referat Agustus 2019Dokumen17 halamanScleroderma: Bagian Ilmu Kesehatan Kulit Dan Kelamin Fakultas Kedokteran Universitas Pattimura Referat Agustus 2019Lhia PrisciliiaBelum ada peringkat
- Radiology DVTDokumen90 halamanRadiology DVTDhruv KushwahaBelum ada peringkat
- MIcrobiology Experiment 12 15Dokumen14 halamanMIcrobiology Experiment 12 15Christina SantosBelum ada peringkat
- NCMB312 RLE-Burn Injuries-Group 3Dokumen56 halamanNCMB312 RLE-Burn Injuries-Group 3Maica LectanaBelum ada peringkat
- Pancreatic Cancer Early Detection, Diagnosis, and StagingDokumen29 halamanPancreatic Cancer Early Detection, Diagnosis, and StagingDokter LinggauBelum ada peringkat
- Protein C & S DeficiencyDokumen20 halamanProtein C & S DeficiencyAhmad Ariff Azmer MunshiBelum ada peringkat
- Group 1,2,4 QuizDokumen221 halamanGroup 1,2,4 QuizPaulBelum ada peringkat
- Appendicitis (History & Examination)Dokumen6 halamanAppendicitis (History & Examination)Doctor Saleem Rehman75% (4)
- Dr. Rosario R. Trifiletti M.D. PH.D.: Date of Preparation May 1, 2010 Personal DataDokumen15 halamanDr. Rosario R. Trifiletti M.D. PH.D.: Date of Preparation May 1, 2010 Personal Dataapi-28616529Belum ada peringkat
- Nutritional Guidelines COPDDokumen2 halamanNutritional Guidelines COPDRod Rafael De LeonBelum ada peringkat
- Castle Connolly Graduate Board Review SeriesDokumen63 halamanCastle Connolly Graduate Board Review SeriesCCGMPBelum ada peringkat