Clinical and Experimental Optometry
Diunggah oleh
Habib SalimHak Cipta
Format Tersedia
Bagikan dokumen Ini
Apakah menurut Anda dokumen ini bermanfaat?
Apakah konten ini tidak pantas?
Laporkan Dokumen IniHak Cipta:
Format Tersedia
Clinical and Experimental Optometry
Diunggah oleh
Habib SalimHak Cipta:
Format Tersedia
OPTOMETRY
REVIEW I
What causes steroid cataracts? A review of
steroid-induced posterior subcapsular cataracts
Clin Exp Optom 2002; 85: 2: 61-75
Andrew I Jobling BScHons PhD Prolonged use of glucocorticoids is a significant risk factor for the development of
Robert C Augusteyn BScHons PhD posterior subcapsular cataract. This places restrictions on the use of glucocorticoids in
DipEd FVCO the treatment of systemic and/or ocular inflammatory conditions as well as in organ
National Vision Research Institute of transplantation.
Australia The mechanisms responsible for the opacification are unknown and no effective treat-
ment, other than surgical removal of the lens, is available. Difficulties in establishing
suitable in vivo or in vitro models have limited research in this area. Nevertheless, sev-
eral mechanisms, based on observations with other types of cataracts, have been pro-
posed. In this review, these mechanisms are evaluated in light of the evidence available.
Accepted for publication: 7 February A novel mechanism is also proposed, in which steroids do not directly act on the lens
2002 but rather affect the balance of ocular cytokines and growth factors.
Key words: cataract, growth factors, PSC mechanisms, steroids
The proper understanding of any biologi- in the developing nations. Breitenkamp*and Hardingl and a specific
cal system is important, not only from a The condition was recognised as long as review on steroid cataract by Urban and
pure knowledge viewpoint but also in pro- 6,000 years ago and many different theo- Cotlier4 are recommended for further
moting the development of therapies to ries and treatments have been offered, information).
combat disease. In this context, the visual tested and abandoned. However, we are no Several mechanisms have been pro-
system has always been of special inter- closer to understanding the changes in the posed for the changes leading to lens
est, because of the importance of vision lens, which lead to this most common vi- opacification. These are listed in Table 1
for our interactions with each other and sion disorder, nor do we have any effective together with brief summaries of their
our environment, yet there are still many non-surgical treatments. Epidemiological major features. Each has been invoked to
visual and ocular functions and disorders studies and clinical observations have iden- explain every form of cataract observed to
that remain a mystery. Loss of lens trans- tified a large number of possible risk fac- date, but none provides a satisfactory ex-
parency, cataract, which is the major tors for cataract, ranging from the absurd, planation of cataract development with
cause of world blindness, is one of these. such as marital status or educational level, increasing age or offers hope for the de-
The World Health Organisation has re- to the more credible, such as cigarette velopment of prophylactic measures. The
cently estimated that cataract accounts smoking or U V exposure. Aging is the most situation could be different for steroid-
for 42 per cent of bilateral blindness in common risk factor, accounting for 75 per induced cataracts because the specific ini-
the world, in more than 20 million peo- cent of cataracts. Other significant risk fac- tiating agent is known but too little defini-
ple. While the incidence of blindness due tors include myopia, diabetes and the long- tive research has been done on possible
to cataract is relatively low in developed term use of steroids. (General reviews on mechanisms. Nevertheless, several theo-
countries, it can be as high as 72 per cent cataracts by Ohrloff, Hockwin and Muller- ries have been advanced.
Clinical and Experimental Optometry 85.2 March 2002
61
Steroid cataracts Jobling and Augustqn
tex, just within the posterior capsule, sometimes
Osmotic Failure of osmotic regulatory systems due to Na,K-ATPase inactivation,
apparently invading it and usually obliterat-
increased membrane leakiness or increased osmolality, gives rise to
localised water accumulation and refractive index fluctuations, which ing the postm'or zone of disjunction; it ex-
produce light scatter. tended forward into the cortex in an irregular
Oxidative Free radical damage, especially by oxygen radicals, is caused by fashion. Its borders were usually sharp, but
increased radical production, antioxidant shortage or protective occasionally surrounded by a faint grey haze.
mechanism failure. Membrane and protein damage follows. The fine structure consisted of tiny whitish-
Protein modification Oxidation, covalent addition of metabolites or other small molecules, yellow crystalline opacities separated by equally
proteolysis and/or alterations in the environment produce conforma- small vacuoles, together appearing as a granu-
tional changes which lead to denaturation, aggregation and lar conglomerate, which occasionally showed
insolubilisation of the lens proteins. linear markings or a few larger vacuoles.
Metabolic disturbance Inadequate energy production, altered protein synthesis cytokine Iridescent blue, green, or red particles appeared
fluctuations can lead to breakdown in protective mechanisms, including frequently within the mass.'
ion pumps and antioxidant pathways, and prevent proper cell matura- Black and colleagues5 noted a definite
tion. dose dependent effect: the higher the ster-
oid dose, the greater the prevalence of
Table 1. Universal theories for cataract formation PSC. Also, it was observed that PSC devel-
oped only after a patient had been on high
dose steroid treatment for longer than one
year, whereas those on doses of less than
10 mg/day of prednisone or equivalent
were unlikely to develop lenticular
changes.
Since this report, numerous studies have
been made of patients with diseases such
as rheumatoid arthritis and asthma, as well
as renal and kidney transplant recipients.
All found a link between systemic steroid
use and PSC de~elopment,"'~ convincingly
refuting some early studies to the con-
t r a ~ y . ' ~The
, ' ~ direct link between steroids
and PSC is now generally accepted. How-
ever, the dosedependent nature of these
cataracts is more controversial, with some
researchersI6'* confirming Black and col-
leagues' ob~ervations,~ while others have
observed no relationship between dosage
and either the incidence or severity of
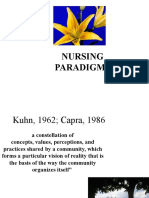
Figure 1. Red reflex slitlamp photograph of PSC.IS2'This has led some authors to sug-
a steroid-inducedPSC. Notice the granular gest that, while the dose of steroid is im-
appearance on the right side of the lens. portant, susceptibility of the individual or
genetic effects may also play a role in the
development of PSC.16.22
A 'safe' dose regimen of 10 mg/day
prednisone for one year was originally sug-
gested as a way of avoiding steroid-induced
subcapsular cataract (PSC) (Figure 1). PSC. However, because of the variability
STEROID CATARACT
The steroid-induced cataract appears bi- in the responses of individuals to various
The relationship between steroid use and laterally and is distinguishable from the steroids, there can be no really 'safe' dos-
cataract was first noted by Black and col- more common types of cataract. OglesbyG age. Regular ophthalmic examinations
leagues in 1960.3In a study of 44 rheuma- described the clinical features of the cata- would seem to be prudent.
toid arthritis sufferers, they observed that ract in a subsequent paper. Cataract development is not restricted
39 per cent of those who had been on sys- 'The characteristic cataract in these patients to systemic steroid use. In 1963, Valerio2'
temic steroid therapy developed posterior occupied the polar region of the postm'or cor- showed that topically applied steroids
Clinical and Experinlentdl Optometry 85.2 March 2002
62
Steroid cataracts Jobling and Augustqn
CI$OH CH20H
I
28
I
c= 0
I
c= 0
H* CH,
HO
cortisol dexamethasone
Figure 2. The structure of cholesterol showing the ring Figure 3. Natural (cortisol) and synthetic (dexamethasone)
designations and the numbering of carbon atoms glucocorticoids
could also result in PSC. This was of par- that steroid therapy had become the a myriad biological functions. In animals,
ticular interest to ophthalmologists and fourth leading risk factor for cataract for- they comprise five groups: progestagens,
optometrists, as topical steroids are widely mation, with only diabetes, myopia and androgens, estrogens, mineralocorticoids
used in the treatment of anterior ocular glaucoma presenting greater risks.3 Ster- and glucocorticoids. All are derived from
infectionsand trauma. Several studies have oids were estimated to be responsible for cholesterol (Figure 2) but they have dif-
confirmed this ob~ervation.~~ Inhaled 4.7 per cent of all cataracts removed in ferent functions and are produced in dif-
steroids, such as those taken for asthma, Oxford. ferent tissues. Progestagens are synthe-
have also been implicated in PSC forma- The incidence of steroid-induced cata- sised in the corpus luteum, androgens and
tionZa3 but careful, long-term monitoring ract is expected to increase further as life oestrogens in the testis and ovary, respec-
of asthmatic patients is needed to evalu- expectancy increases and more people tively, and mineralocorticoids and
ate this possibility. develop conditions that can benefit from glucocorticoids in the adrenal cortex.
Steroid therapy can have a more pro- steroid therapy. To minimise the impact (For more detailed descriptions, see
nounced effect on children, with PSC de- on the quality of life in the elderly, treat- SchroepfeP and Harnm~nd.~)
velopment occurring at a faster rate and ments have to be developed to prevent or The mechanisms by which steroids me-
at a lower dosage than with ad~lts.,:~~For reverse cataract development. However, diate alterations in normal cell function-
example, PSC has been observed in young this will only be possible when we have a ing are complex in nature and, to date,
patients after only six months of glucocor- thorough understanding of the mecha- are not fully elucidated. It is probable that
ticoid ~ e a t m e n t . ~ nism involved in the cataract formation. steroids, being lipid soluble, passively dif-
There have been reports of cataract re- We are still a long way from achieving this fuse through the plasma membranes of
versal following cessation of the steroid and substantial research is required. Un- target cells. Once in the cell, they bind to
treatment, especially in ~hildren.~ How- fortunately, very little research is being receptor complexes, which consist of one
ever, these are rare and once vision has conducted now on steroid cataracts or two specific receptor protein molecules
been affected, complete resolution of the In this article, we examine possible rea- associated with a variety of other proteins.
opacity is ~ n l i k e l y . ~ ~ ~ sons for cataract formation associated with One such complex, the glucocorticoid
The incidence of PSC in the population prolonged steroid treatment. We will be- receptor, will be discussed later. The vari-
in 1966 was estimated by Spaeth and von gin with a brief overview of steroids and ous molecules associated with the complex
Sallrnann to be 0.2 per cent in young attempts to establish model systems for are critical in mediating the binding of
adults, rising to 0.6 per cent in the fifth to studying steroid cataracts. Thereafter, we steroid to the receptor and DNA, as well
sixth decades. This suggests that steroid- will consider possible mechanisms as the translocation of the steroid-receptor
induced PSC was of minor significance whereby steroids generate cataract. complex to the nucleus.
around that time. However, the use of ~~ ~ ~
Binding of the steroid to its specific
glucocorticoids has since become much receptor results in a conformational
STEROIDS
more widespread and the incidence of (shape) change to the receptor, so that it
steroid cataracts is expected to rise as a Steroids are widespread throughout the can now interact with DNA. The steroid-
result. A 1985 Oxfordshire study found animal and plant world, where they have containing complex then binds to specific
Clinical and Experimental Optometry 85.2 March 2002
63
Steroid cataracts Jobling and Augusteyn
nucleotide sequences in the cell genome,
known as hormone responsive elements Drug Relative Equivalent Mineraiocorticoid
anti-inflammatory dose (mg) potency relative to
(HREs). Subsequent interaction of the potency Hydrocortisone
hormone with nearby DNA regulatory
elements can increase or decrease the Hydrocortisone 1 20 1
transcription and expression of specific Prednisone 4 5 0.8
genes. There may be many steroid HREs Cortisone 0.8 25 0.8
on many genes and some may also be re-
Prednisolone 4 5 0.8
sponsive to other hormones or affector
molecules. Methylprednisoione 5 4 0.5
Triamcinolone 5 4 0
GLUCOCORTICOIDS Paramethasone 10 2 0
The major naturally occurring glucocor- Betamethasone 25 0.6 0
ticoid is cortisol, also known as hydrocor- Dexamethasone 25 0.75 0
tisone (Figure 3), but metabolic deriva-
tives, such as cortisone and corticosterone
also function as hormones. Their function Table 2. Relative properties of some anti-inflammatory gluco-
appears to be in stimulating gluconeogen- corticoids*
esis, the production of glucose from non- * Taken from Hammondsg
carbohydrate carbon sources such as
amino acids. This involves promoting the
catabolism of muscle proteins, increasing
the transport of amino acids into the cell
and stimulating the syntheses of gluconeo-
genic enzymes and trans-aminases. The
glucocorticoids also have some mineralo- inflammatory properties and reduced Models for steroid cataract
corticoid activity, promoting renal sodium mineralocorticoid activity. In particular, One of the most useful tools in biological
reten tion. introduction of a second double bond in research is an animal model and, because
In addition, the glucocorticoids are very Ring A (Figure 2) and substituents on car- of this, in the past significant resources
powerful anti-inflammatory and immuno- bon atoms 9 and 16 substantially altered were directed towards inducing steroid
suppressive agents. This led to their intro- the biological effects. Table 2 lists some of PSC in laboratory animals. Attempts to
duction by Hench and c o - w ~ r k e r sas~an
~ the derivatives and compares them with induce such cataracts have been based on
effective treatment for rheumatoid arthri- the natural glucocorticoids. Of particular the assumption that steroids act directly
tis in 1949. Since then, they have been note are the synthetic glucocorticoids, on the lens. These attempts have been
widely used for controlling inflammation betamethasone and dexamethasone largely unsuccessful.
in various tissues, including the eye.414In (Figure 3), which have very high anti- In 1960, von Sallmann and colleagues5r
more recent times, glucocorticoids have inflammatory activity and little mineralo- injected rats daily with dexamethasone for
become invaluable in helping to control corticoid activity. They provide much more 16 weeks but found no indications of lens
rejection of organs in transplant recipi- effective alternatives to the naturally opacification. No opacities were observed
e n t ~The. ~ ~choice of glucocorticoid de- occurring hydrocortisone. by Spencer and Andelman,5*after treat-
pends not only on the efficacy of its anti- Adverse effects, including several ocu- ing rats for 16 weeks with triamcinolone
inflammatory action but also on its lar manifestations, may result from gluco- acetonide or by B e t ~ n a n , 5who
~ . ~exposed
~
mineralocorticoid activity, which, unless corticoid use.36These are summarised in chickens to prednisolone. A major com-
controlled, can result in unwanted side Table 3. Prolonged steroid use can lead plicating factor in all these studies was the
effects. to diabetes and its ocular complications high number of deaths due to the large
The recognition of the potential ben- as well as elevation of intraocular pressure, steroid doses employed. Wood and co-
efits of glucocorticoids and the subsequent which can lead to optic nerve damage and w o r k e r ~observed
~~ anterior subcapsular
demand for reliable supplies stimulated visual field changes.4M8 Reactivation of the cataracts in rabbits after topical applica-
the production of synthetic glucocorti- herpes simplex virus is a common second- tion of steroids, three times daily for a six-
coids. Although the mechanisms of glu- ary effect of steroid treatment,49as is a re- month period. Cortisone was the most
cocorticoid actions were not understood, duction in corneal wound healing.50How- potent, while dexamethasone and pred-
chemical modification allowed the genera- ever, most common is the development of nisolone were the least. However, since the
tion of derivatives with improved anti- posterior subcapsular catara~t."~ cataracts occurred in the anterior subcap
Clinical and Experimental Optometry 85.2 March 2002
64
Steroid cataracts Jobling and Augustqrn
sular area, they could hardly be considered
COMPLICATION MORE COMMON suitable as models for the human poste-
VEHICLE
rior subcapsular cataracts.
Gastrointestinal Oral or intravenous Only a small number of investigatorshas
gastritis ulcers succeeded in producing posterior subcap
visceral perforation sular cataract in laboratory animals.
pancreatitis
Tarkkanen and co-workerP observed PSC
nausea
increased appetite after 41 weeks subconjunctival injection of
betamethasone in two of four rabbits that
Central nervous system Oral or intravenous
headache survived out of an original cohort of seven.
convulsions However, from week 28, the rabbits devel-
pseudotumour cerebri oped diabetes, which may have been re-
psychiatric disturbances: anxiety, psychosis sponsible for the cataract formation.
Cardiovascular Oral or intravenous Bucala and colleagues58also succeeded in
hypertension producing steroid-induced PSC in rabbits
Ophthalmological Topical or oral by intravitreal injection of glucocorticoids.
glaucoma The lenticular effects were observed at
herpes simplex keratitis activation concentrations as low as 2x104 M and de-
posterior subcapsular cataracts veloped 48 to 72 hours after the injection.
central serous retinopathy
The opacities were said to be similar in
fungal or viral infection
appearance to those observed in human
Renal Oral or intravenous arthritis sufferers, as reported in the origi-
sodium retention, potassium loss
nal Black and colleagues study. N o fur-
hypokalaemic alkalosis
fluid retention ther investigations appear to have been
conducted by these authors and their
Murculoskeletal Oral or intravenous
distal wasting and weakness observations have not been reproduced
myopathy elsewhere.
osteoporosis Cataract can also be induced in the
fractures chicken, mouse, rabbit and rat foetus by
aseptic necrosis of the femur prenatal administration of glucocortic-
tendon rupture
o i d ~However,
. ~ ~ ~this is unlikely to be of
Metabolic Oral or intravenous any relevance to human postnatal steroid-
glucose intolerance induced cataract. The opacities are neither
hyperosmolar nonketotic coma
hyperlipidaemia posterior nor subcapsular but appear as
obesity supranuclear rings before engulfing the
nucleus. Furthermore, in the chick em-
Endocrine Oral or intravenous
retardation of growth in children bryo, the opacity forms 24 hours after a
secondary amenorrhoea single injection of glucocorticoid and dis-
hypothalamic-pituitary axis suppression appears 72 hours later. The transitory na-
Cushingoid state ture of this cataract makes it unlike true
glucose intolerance
steroid cataracts, which are very rarely, if
General Oral or intravenous ever, reversible.
weight gain Similar difficulties have been encoun-
hirsutism
tered in attempts to establish in nitro model
decreased wound healing
increased sweating systems, even when very high concentra-
easy bruisability tions of steroid are used. Sivak and col-
subcutaneous tissue atrophy leaguestismaintained bovine lenses in me-
increased bacterial, viral and parasitic infections dium containing 3x10. M prednisone for
three weeks. Examination with an auto-
Table 3. Complications associated with glucocorticoid treatment * mated scanning laser revealed no altera-
* Taken from Rubm and Palestine tion in focal characteristics or light scat-
ter of the lens. N o opacities were observed
by Haddad, Furman and Bella Shoreti4
after an eight-day incubation of bovine
Clinical and Experimental Optometry 85.2 March 2002
65
Steroid cataracts Jobling and Augustqrn
lenses with 1O'M methylprednisolone has concentrated on the metabolic effects mediate their effects via the antagonism
acetate. By contrast, Miller, Tijerina and of glucocorticoids in the lens. Unfortu- of lens glucose uptake or utilisation. Such
Maymad5 reported cortical changes in nately, a plethora of contradictory results glucocorticoid induced decreases i n
bovine lenses incubated for three days with makes it difficult to come to any signifi- glucose uptake have been observed in
104M dexamethasone-21-phosphate. How- cant conclusions. This may, in part, be due other tissue^.'^^^^ However, Jobling and
ever, the changes did not resemble those to the use of animals and tissues of vari- Augusteyn" found that neither dexam-
of the human steroid PSC, but were simi- ous ages. It has been reported that ethasone nor prednisolone had any effect
lar to those found when the lens was incu- glucocorticoids affect lens metabolism on glucose uptake by cultured bovine lens
bated with ouabain, a potent Na+,K+-AT- only in young lenses.67 epithelial cells.
Pase inhibitor. Rat lenses maintained in a Both increases and decreases have been The protein synthetic machinery of the
medium containing methyl prednisolone reported for the same enzymes and meta- lens also may be altered by glucocorticoids.
developed opacities within 48 hours of bolic intermediates and the effects vary This occurs in other tissues due to the ster-
exposure,66but these were similar to the with the steroid. For example, lactate de- oid limiting the peptide chain initiation
ring cataracts observed in embryonic hydrogenase levels appear to increase with step.76Friedburg, KrBner and Rosenstei17?
lenses.62 dexamethasone treatment, yet remain observed a decrease in lens protein syn-
So far, it has not been possible to de- unaffected by hydroc~rtisone.~~ Hexoki- thesis in the presence of &methyl pred-
velop a reliable model system, animal or nase activity was found to be unaltered by nisolone acetate. However, van Venrooij,
isolated lens, suitable for the study of glucocorticoids in one but inhib- Groeneveld and B l ~ e m e n d anoted
l ~ ~ that
steroid-induced PSC. Cataract induction ited in other^.^^.^^ Glucose-&phosphate dexamethasone, while causing a definite
in vivo is difficult and seems to depend not dehydrogenase (GGPDH), a key enzyme change in cellular morphology, did not
only on the specific glucocorticoid used in the pentose phosphate shunt, is affect the amount of protein synthesised
but also on the schedule, dosage, vehicle inhibited by hydroc~rtisone,~~ but not by or the nature of the proteins produced.
used for administration and the animal prednisolone, d e x a ~ n e t h a s o n eor . ~ ~ Jobling and A ~ g u s t e y nfound
~ ~beta- ~ ~ no altera-
species. Even when lenses are exposed metha~one.~ Some
' of the differences tions in synthesis levels or patterns in cul-
directly to high concentrations of steroids, could be explained by the specificity of tured epithelial cells exposed to dexam-
it has proved difficult to generate opaci- interactions, but most appear to reflect ethasone or prednisolone.
ties similar to those seen in humans. Be- differences and difficulties in experimen- Glucocorticoids can have significant ef-
cause of these difficulties, research on the tal procedures. For example, the epithe- fects on cell growth and DNA/RNA syn-
mechanism of steroid cataracts has flagged lium where most metabolic activity is lo- thesis.79Such alterations have been ob-
in recent years. Only limited information cated represents a very small proportion served in ocular cells, with some cells, such
on the possible molecular events during (less than one per cent) of lens mass. This as retinal endothelial cells, showing growth
cataract formation has been obtained from makes it very difficult to identify specific inhibition, while others seem to be stimu-
laboratory studies with isolated lens con- changes in the epithelium when using lated by glucocorticoids.w2 Lens epithe-
stituents and much of this is contentious. whole lenses. Culturing epithelial cells can lial cells may also be under glucocorticoid
Nevertheless, several molecular explana- overcome this problem but may result in control, with decreases reported in RNA/
tions have been offered for the mechanism uncharacteristic responses. DNA synthesisR3and cell How-
of steroid cataract formation. We will ex- Phosphorus-31 NMR studies have re- ever, this was disputed by van Venrooij,
amine each of these theories. Thereafter, vealed that ATP and dinucleotide levels in Groenveld and Bl0emenda1,~~who saw no
we will explore the increasingly more at- the lens decrease following a 24hour ex- effect of dexamethasone on DNA synthe-
tractive possibility that steroids do not di- posure to d e ~ a m e t h a s o n e This
. ~ ~ would sis in cultured bovine capsule-lens epithe-
rectly affect the lens to generate cataract. impact on the tissue's ability to perform lium. Jobling and Augu~teyn?~ reported
energydependent processes, such as pro- the same for cultured bovine lens epithe-
Metabolic disturbances tein synthesis and ion transport, as well as lial cells.
Glucocorticoids can impact on cellular the ability to maintain antioxidant protec- It is difficult to come to any clear con-
metabolism by interacting directly with tive mechanisms. By contrast, other phos- clusions about the effects of glucocortic-
enzymes, to alter their activities, or phate complexes, such as sugar phos- oids on lens metabolism, because of the
through receptor-mediated pathways to phates, inorganic orthophosphates and variability of the published observations.
change the amount of enzyme being syn- nucleoside diphosphorylsugars have Perhaps there are no significant effects
thesised by the cell. The receptor will be shown glucocorticoid-inducedincreases.72 and the differing observations simply re-
discussed in detail later. What this might mean is not obvious at flect the difficulties in performing these
Many metabolic effects are exerted on present. The overall apparent effect of experiments.
enzymes involved in carbohydrate metabo- glucocorticoids on lens organophosphates
lism and, in particular, gluconeogenesis. observed by Greiner, Kopp and G10nek'~ Osmotic failure
For this reason a number of investigations led them to suggest that steroids may The appearance of intercellular clefts,
Clinical and Experimental Optometry 85.2 March 2002
66
Steroid cataracts Jobling and Augustqrn
/ oxidtion
Figure 4. Pumpleak model for maintenance of ionic balance in Figure 5. Universal mechanism for cataract formation.
the lens. K+ions diffuse out of and Na' ions into the lens. They Conformational changes in lens proteins (unfolding), due to a
are pumped in or out again, respectively, by the Na+,K+-ATPase variety of factors, can expose thiol groups, which become oxidised
located in the anterior epithelium. Inhibition of the pump or to disulphides. This, together with non-specific hydrophobic
increased ion fluxes due to membrane damage will lead to Na' interactions,is believed to generate large protein aggregates that
and water accumulation and cataract. scatter light.
vacuoles and swollen cells in some steroid non-physiological concentrations of ster- tor and resulted in a reduction in light
cataracts has led to the suggestion that oid (greater than 10-3M)and could be due transmission by the lens.
there may be glucocorticoid-induced al- to the disruption of the lipid bilayer By contrast, there are several reports
teration in lens hydration. However, again, through the incorporation of the hydro- indicating steroids d o not influence lens
the data are less than convincing. phobic steroid molecules. Intravitreal in- ion levels. T h e steroid derivative, 9-a-
As with other tissues, the lens maintains jection of 6methyl-prednisolone acetate fluorohydrocortisone, which is known to
ion differentials between the intra- and (final concentration approximately 104M) have considerable impact on ionic flow in
extracellular fluids (high K+and low Na', in guinea pigs has been found to produce the kidney, has no effect on the lens. Topi-
internally; low K , high Na', externally) variable alterations in ion levels." cal betamethasone does not alter the
via the action of the sodium-potassium ad- Glucocorticoid-induced modulation of pump as measured via H6Rbuptake.y4(Rb
enosine triphosphatase, Na+,K-ATPase the Na+,K'-ATPase has been observed in can replace Kand be pumped into the lens
(Figure 4;for a review of the Na+,K+-AT- many tissues. For example, prednisolone epithelium by the Na+,K-ATPase). Simi-
Pase pump, the reader is directed to an inhibits the activity in the choroid plexus:9 larly, several steroids, including pred-
article by Skoun5).The maintenance of while dexamethasone appears to activate nisolone hemisuccinate and dexametha-
ionic balance has been shown to be cru- the pump in rat kidney.9"This latter effect sone produced n o alteration in n6Rb
cial for lens transparency and alterations is probably due to effects on gene expres- uptake by isolated lenses, even at concen-
in the ionic composition of the lens have sion, mediated through the glucocorticoid trations as high as 10" M.y5,96
been associated with ~ a t a r a c t . ~ ~ Saltera-
uch receptor?' Mayman, Miller and TijerinaW Whether steroids can inhibit lens Na+,K'-
tions could arise from failure of the AT- in 1979 reported an 80 per cent inhibi- ATPase activity remains to be established.
Pase pump or from increased membrane tion of calf lens Na+,Kt-ATPaseby 10"M However, in the absence of a clearly iden-
permeability. dexamethasone. This can be attributed to tifiable effect, it seems unlikely that this is
Early reports on the effects of steroids a direct effect of the dexamethasone on responsible for cataract. Furthermore, the
on lens ion levels were equivocal. In 1962, the pump, because the decrease in activ- morphology of the steroid cataract, with
Harris a n d GruberH8reported that ity occurs long before any new protein its localised light scatter, is unlike that of
glucocorticoids made the rabbit lens more could be synthesised.93 The inhibition osmotic cataracts, which are characterised
'leaky', allowing more Na' to enter. Some showed a dose dependence similar to that by the presence of water clefts and light
of the effects were observed at very high, of ouabain, a potent Na+,K-ATPaseinhibi- scatter throughout the lens.
Clinical and Experimental Optometry 85.2 March 2002
67
Steroid cataracts Jobling and Augusteyn
Oxidation/conformational could contribute to the development of
change the disease. Lens protein adducts have
The most commonly offered explanation been implicated in cataracts associated
for development of any type of cataract, with diabetes (reducing sugars), renal fail-
the 'universal' cataract mechanism, is that ure (cyanate, generated from urea) and
conformational change, due to some form ageing (photo-oxidation products) .'04-'06
of stress (oxidative, osmotic, metabolic), They have also been invoked as the cause
makes lens proteins susceptible to of steroid cataract.
oxidative modification. This is postulated Bucala, Fishman and CeramilO' discov-
to result in disulphide bond formation, ered that steroids, containing both a G20
pigmentation and other oxidative change carbonyl and a G21 hydroxyl group, could
as well as the generation of non-specific react with proteins to form stable adducts.
hydrophobic interactions to produce large The reaction involves formation of a Schiff
protein aggregates,which scatter light and base between amino groups in the protein
become insoluble (Figure 5). and the G20 carbonyl bond of the ster-
The oxidation explanation has been in- oid. This is followed by a Heyns rearrange-
voked for steroid cataracts, based on the ment involving the G21 hydroxyl group
idea that glucocorticoids may affect the to form a stable ketoamine product
activities of mechanisms involved in pro- (Figure 6).
tection of the lens from oxidative stress. The steroid-protein adduct reaction is
The lens contains a variety of such protec- very slow and follows first order kinetics.
tive mechanisms, including the glutath- Therefore, for a n y significant modification
ione/glutathione reductase and free
radical scavenging systems.y7Some inves-
to take place, the target proteins must be
long-lived and at high concentration. I ?
+I
M
tigators have reported decreases in the These criteria are met in the lens, leading
Lysirs f-amlrm
levels of the antioxidants, glutathione and to the suggestion that steroid adducts may
ascorbic acid, in both the lens and the accumulate and contribute to the cataract
aqueous humour, followingglucocorticoid development. The 'universal' mechanism
treatment62~y6*yRbut others have found no for cataract formation has been invoked
effect.55Loss of GSH is observed whenever to explain the subsequent opacification
the lens is stressed, in uztro or in uiuo. process, that is, the formation of steroid-
Whether the observed decrease (20 per protein adducts result in an alteration in
cent in uitro,9651 per cent in uiuo ") is re- normal protein structure (conformational Figure 6. Formation of steroid-protein
sponsible for steroid cataract remains to change), thus exposing sulphydrylgroups, adduct. The amino group in the side chain
be established. Increased lipid peroxide which are subsequently oxidised to form of lysine in the protein reacts with the ketone
has been reported in the chick embryonic intermolecular disulphide bonds. The group at carbon-20 in the steroid to form a
lens but this is probably not relevant to disulphide bonds as well as non-specific Schiff's base. The reaction is reversible but
the human condition.w Interestingly, the hydrophobic interactions are postulated becomes irreversible following a Heyns
free radical scavengers vitamin E66and to result in the formation of high molecu- rearrangement. This generates a new
N-( 2-mercaptopropionyl) glycineloOare lar weight aggregates that become insolu- aldehyde group that can react with another
known to slow steroid-induced alterations ble and produce light scatter. amino group to form a second Schiffs base.
but how they act is unclear. Some support for this idea comes from This reaction can result in crosslinking of
the observations that in uitm exposure of protein molecules.
Protein adduct formation rat and rabbit lenses to steroids results in
The nonenzymatic addition of small mol- adduct formation and o p a c i f i c a t i ~ n . ~ ~ ~ ~ ~ ~
ecules to proteins (generating protein The opacities observed in the rabbit were
adducts) is frequently observed, especially very similar to those seen in humans by
in disease.'0'J02The reaction of glucose Black and colleague^.^ Prednisolone and
with haemoglobin A to produce the modi- cortisol adducts generated in the lens were
fied haemoglobin Alc is an example of insoluble~lOsJw whereas dexamethasone
such an addition and can be used to moni- adducts are soluble.5RIncubation of iso-
tor the progress of diabetes.lo5The addi- lated rabbit lens proteins with pred-
tion of small molecules can alter the func- nisolone has been reported to generate
tion or properties of a protein and this disulphide linked, high molecular weight
Clinical and Experimental Optometry 85.2 March 2002
68
Steroid cataracts Jobling and Augustqrn
Receptor mediated effects
Glucocorticoid effects on some cellular
activities are mediated through the gluco-
corticoid receptor, a cytosolicprotein com-
plex that binds the steroid and translocates
it to the nucleus. A diagram illustrating
the translocation mechanism is shown in
Figure 7."' Establishing if such a receptor
is in the lens is critical in evaluating the
mechanism responsible for steroid-
induced PSC. Observations in one labora-
tory have indicated that such a receptor is
Figure 7. The glucocorticoid receptor complex, which is found found in the lens and other ocular tissues
in the cytoplasm of the cell, consists of one molecule of receptor but other laboratories have been unable
protein (GR) associated with several other proteins including two to reproduce these observations.
molecules of hsp90 and one of p59. On binding of steroid, the It was reported by Weinstein and co-
complex dissociates, the receptor protein plus steroid forms a workers112.115 in the 1970s that several ocu-
dimer and this dimer translocates to the nucleus, where it binds lar tissues, including retina, iris-ciliary
to specific hormone responsive elements in the genomic DNA. body, outflow pathway and sclera exhib-
This modifies the expressionof specific genes and the subsequent ited glucocorticoid binding and cellular
synthesis of protein on the ribosomes. (Adapted from Muller and localisation consistent with the presence
Renkawitz"') of a glucocorticoid receptor. In 1978,
Southren and colleague^^'^ showed that
bovine lens epithelial extracts bound dex-
amethasone with high affinity (Kd =
8x1OY)and low capacity (550 fmoles/mg
protein). The steroid binding showed simi-
larities in temperature lability and com-
petition patterns to those of the classical
aggregates which scatter light.98However, tain insoluble steroid-protein adducts.Iog glucocorticoid receptors described in
and Jobling and Augusteynllohave shown It has been estimated that between 0.1 other tissue^."^ By contrast, bovine lens
that exposure of bovine lens proteins to and 1.34 millimoles of adduct per mole nuclear extracts exhibited saturable and
dexamethasone or prednisolone has no of polypeptide may be the pathological heat stable association of the steroid with
discernible effect on their solubility, level of adduct formation in the human protein. A later report from the same labo-
molecular weight, sulphydryl content or and result in PSC formation.5RIt is hard ratory presented autoradiographic data
conformation even though adducts were to understand how a maximum of only showing glucocorticoid binding and ap-
formed. It has also been reported that one adduct per 750 protein molecules parent localisation in the nuclei of cells in
opacities can be induced, in uitm or in uivo, could lead to large scale insolubilisation the anterior epithelium and bow regions
only if the steroid contains both the C-20 of the proteins. Much higher ratios would of the bovine lens,Il5again consistent with
carbonyl and G21 hydroxyl groups, which obtain if one assumed that the adduct is the behaviour of the classical receptor and
were considered to be necessary for located only in the region affected by the the accepted mechanism whereby gluco-
steroid-protein adduct f o r m a t i ~ n . ~ ~ ~ . "cataract,
' ~ ~ ' " ~ say one per cent of the lens, but corticoids regulate cell metabolism.
However, Dickerson, Dotzel and Clarkgfi even then the proposition is not compel- However, other observations indicate
and Jobling and Augusteynll" have ques- ling. Furthermore, it is even harder to un- that there is no receptor in the lens.
tioned these observationsand conclusions. derstand how adduct formation could be Tetrahydrocortisol, an inactive metabolite
Dickerson, Dotzel and ClarkMshowed that restricted to a small region of the lens and of cortisol, competes with dexamethasone
steroids lacking the C-21 OH group still to the posterior ends of the fibre cells to for the lens binding sitesIl5whereasit does
bound covalently to lens proteins, prob- produce the posterior subcapsular not for the glucocorticoid receptor.l16Tri-
ably through an amino group. Further- opacities. amcinolone, which is known to compete
more, they showed that non-glucocortic- There is no doubt that some steroids can for receptor sites,l"does not compete for
oids also bound to the proteins but did form adducts with lens proteins in uivo. the lens sites."5 The nuclear localisation
not cause opacities. However, it seems unlikely that this is of steroid, as described by Wenk and co-
Lenses from patients with steroid- responsible for gross alterations in lens worker~"~ was not observed in lens epithe-
induced PSC have been reported to con- proteins or in PSC. lial cells following intravenous administra-
Clinical and Experimental Optometry 85.2 March 2002
69
Steroid cataracts Jobling and Augustqrn
to anteriar chamber cell proliferation tion of dexamethasone.Il8 Recently,
f Jobling and Aug~steyn'~ showed that there
was very weak binding of dexamethasone
to soluble proteins, but this did not exhibit
the heat lability typical of receptor pro-
teins.
It was later shown that the binding was
due to non-specific interaction of steroid
with a-cry~tallin."~ Although receptor
mRNA can be detected in the
no receptor protein could be found using
specific antibodies.'lg
From the currently available data, it
would appear that there is no classical glu-
Figure 8. Lens architecture and growth: Nucleated and cocorticoid receptor in the lens, but that
metabolically active cells are found only in the anterior, equatorial non-specific binding of steroids can take
and bow regions of the lens. The majority of the tissue comprises place with some of the lens proteins. This
elongated fibre cells that lack cellular organelles, Growth factors, binding appears unlikely to have any physi-
such as FGF, in the aqueous humour induce proliferation and ological role.
migrationof anterior epithelialcells to the equatorialzone where
they differentiate into fibre cells. The fibre cells are gradually Aberrant cell behaviour
compressedinto the centre of the lens by new overlying cells and The lack of a glucocorticoid receptor and
lose their organelles in the process. the inconclusive observations on the ef-
@ epithelial cell cell migration fects of steroids on the lens have led us to
@growth factors + aqueous humour flow the idea that steroids may not act directly
on the lens to generate cataract.
One of the features of steroid cataract
appears to be the accumulation of undif-
ferentiated epithelial cells just under the
capsule at the posterior pole of the lens.
to anterbr chamber cell DrolNeratiin Such cells should be found only on the
f anterior surface of the lens mass. This sug-
gests that aberrant cell behaviour may be
involved in cataract formation. To explore
this possibility,some understanding of the
anatomy and growth of the normal lens is
required.
A simple diagram illustrating lens archi-
tecture and growth is presented in Figure
8. All lens cells are epithelial in origin.
They occur in two morphological forms,
'\
the cuboidal cells and the elongated fibre
\ undlfferentietedcells cells, reflecting two stages of cell develop-
ment. The cuboidal cells are found in a
Figure 9. Proposed mechanism for steroid cataract formation. single layer at the anterior surface of the
Reduced FGF levels and/or altered levels of other growth factors lens, directly underneath the capsule.
in the aqueoushumour,due to the effects of steroidson the ciliary They are nucleated and are the only ac-
epithelium, prevent the normal differentiation of epithelial cells tively dividing cells present in the lens.
into fibre cells. The undifferentiated cells are not packed into Apart from providing new cells, the epi-
the fibre cell mass but continue to migrate along the capsule past thelium accounts for almost all the meta-
the equatorial zone until they reach the posterior pole of the lens bolic activity required for normal lens
where they form irregular clumps of cells that scatter light. functioning. The only other nucleated and
epithelial cell cell migration metabolically active cells in the lens are
0 growth factors + aqueous humour flow those in the process of differentiating into
Clinical and Experimental Optometry 85.2 March 2002
70
Steroid cataracts Jobling and Augustqn
fibre cells. These are located in the equa- (TGF-P) and other members of the FGF differentiation. When aqueous humour
torial zone and bow region. The fibre cells, family involved in these processes. The containing the altered complement of
which lack nuclei and cellular organelles sites where the growth factors originate growth factors acts on the lens, prolifera-
and are essentially metabolically dead, have not yet been established but they are tion and migration of anterior epithelial
constitute the vast bulk of the lens volume. present in the aqueous humour and have cells occurs, as normal, but no differen-
Lens growth takes place through prolif- been localised in the ciliary epithelia.Iz6 tiation takes place in the equatorial zone.
eration of the cuboidal epithelial cells and Alterations in the complement of As a result, cells are not incorporated into
continues throughout the life of the or- growth factors impacting on the lens could the fibre cell mass but, instead, continue
ganism, slowing with age. As new cells are lead to aberrant cell behaviour and cata- their migration until they reach the pos-
formed near the equator, the adjoining ract development. This is what one might terior pole of the lens, where they accu-
epithelial cells gradually migrate (or are expect in a situation where the concen- mulate forming clumps which scatter light.
displaced) towards the equatorial regions tration of FGF was not high enough to The proposed mechanism is illustrated in
of the lens.Iz1Here, they undergo termi- stimulate differentiation of the epithelial Figure 9.
nal differentiation and elongation into cells into fibre cells in the equatorial zone Further work is required to establish if
fibre cells, which are forced towards the or if differentiation were inhibited by an- this is the mechanism for steroid cataract
interior of the lens and compressed (Fig- other cytokine. The undifferentiated cells formation. If this turns out to be the case,
ure 8) as new cells are deposited over would continue to receive signals to mi- it may be possible to design drugs to
them.Iz2The cells gradually lose their nu- grate and would pass through the equato- modify the ciliary body's response to ster-
clei and all other intracellular organelles, rial zone. Eventually, the cells would end oids and thereby prevent or reverse the
such as mitochondria, as they pass through up in the centre of the posterior pole, steroid cataract.
the bow region of the lens. Consequently, where they would have maximum impact
the mature fibre cells lack the ability to on light scatter. It was shown by Hales and Possible drugs
perform metabolic functions such as the co-worker~'~' that alterations in growth fac- As with most types of cataract, several sub-
synthesis of proteins and production of tors such as TGF-P will alter lens epithe- stances have been investigated for their
energy. lial behaviour and give rise to cataract-like ability to slow or halt steroid-induced PSC
The proliferation and differentiation of changes in capsular explants. Alternatively, formation.
the epithelial cells are under the control posterior lens cells could be induced to Antioxidants and/or free radical scav-
of growth factors present in the ocular create epithelial cells by retinal factors, as engers are commonly believed to offer
media that bathe the lens. McAvoy and shown by Coulombre and Coulombre in protection from cataract, including those
ChamberlainIz3in Sydney have identified their classic lens reversal experiments.lzZ due to steroids. Creighton and co-work-
fibroblast growth factor-2 (bFGF) as a It is our hypothesis that steroid cataract ers&showed that vitamin E caused not only
major affector of lens growth and have is due to an alteration in growth factors a decrease in the incidence of steroid-
shown that there is a gradient of increas- reaching the lens and that this follows ster- induced cataract in rats but also a decrease
ing concentration of bFGF in the aqueous oid-induced alterations in the production in the severity of opacification. The im-
humour from the anterior to the poste- of these growth factors in other ocular tis- plied reason was that free radicals were
rior of the eye. This gradient is critical for sues. It is probable that the ciliary body is being scavenged by vitamin E, thus pre-
controlling lens cell behaviour. The low the site of steroid action. The tissue pos- venting oxidative damage in the lens.
bFGF concentration in the aqueous hu- sesses an extensive network of capillaries, Whether this was due to a direct effect on
mour flowing over the anterior surface of which ensures that systemic as well as topi- the pathway leading to steroid cataract
the lens is sufficient to stimulate epithe- cal steroids will be delivered to the site of remains to be established. Nishigori and
lial cell proliferation and migration (to- aqueous production, the non-pigmented co11eagues'"OJZR found that the free radi-
wards the equator), while the higher con- epithelium, where they can affect the syn- cal scavenger N-( 2-mercaptopropionyl)
centrations around the equatorial region thesis of proteins being produced for ex- glycine (MPG) as well as compounds such
will induce differentiation into fibre cells. port. The epithelium contains a glucocor- as ascorbic acid and polyethylene glycol
It is of interest to note that the vitreous ticoid receptor and it is known to produce delayed the appearance of glucocorticoid-
humour also contains high concentrations a number of growth factors that are im- induced cataracts in chick embryos. How-
of bFGF, which will cause differentiation portant for maintaining ocular tissues. ever, as indicated earlier, the chick embry-
of anterior epithelial cells if the lens is re- Production of these growth factors has onic cataract is not a suitable model for
v e r ~ e d . ' ~More
~ . ' ~ recent
~ work has indi- been shown to be affected by steroids. It steroid cataract in mammals.
cated that there may be several other is proposed that steroids cause a reduc- Aspirin (acetylsalicylic acid) has also
growth factors, such as epidermal growth tion in the growth factors such as FGF, been proposed as a way of limiting steroid
factor (EGF), insulin-like growth factor which stimulate differentiation of lens induced opalescence.'" Aspirin is thought
(IGF), platelet-derived growth factor epithelial cells or an increase in growth to acetylate the lysine residues in lens pro-
(PDGF), transforming growth factor factors such as TGF-P, which inhibit this teins, thereby preventing the binding of
Clinical and Experimental Optometry 85.2 March 2002
71
Steroid cataracts Jobling and Augustqrn
glucocorticoids through their (2-20 carbo- an intervention strategy for preventing Oczna 1991; 93: 332-333.
nyl bond and stopping the eventual disul- cataract, thereby permitting more exten- 14. Abrahamson IA Jnr, Abrahamson IA Snr.
Cataracta complicata and corticosteroids.
phide bond formation and light scatter. sive use of steroids.
The question of a possible relationship be-
This type of protective effect has also been tween posterior subcapsular cataracts and
suggested for other cataracts.i30However, ACKNOWLEDGEMENTS corticosteroids. Eye Ear Nose Throat Month
the justification of aspirin as a treatment Preparation of this review and some of the 1961; 40: 266269.
for any form of cataract has been ques- research, discussed herein, were sup- 15. Hart FD, Casey TA, ORiordan MD. Cata-
ract and steroids. Br MedJ 1961; 1 : 1680-
tioned. It is highly unlikely that sufficient ported, in part, by the Cooperative Re-
1681.
aspirin can reach the lens without being search Centre for Eye Research and Tech- 16. Skalka HW, Prchal JT. Effect of corticoster-
hydrolysed to salicylic acid. It is also highly nology. AIJ acknowledges receipt of an oids on cataract formation. Arch Ophthalmol
unlikely that lens proteins could remain Australian Postgraduate Research Award. 1980; 98: 1773-1777.
soluble following extensive loss of the 17. Bihari M, Grossman BJ. Posterior subcap-
REFERENCES sular cataracts. Related to long-term corti-
charged amino groups due to acetylation.
1. Thylefors B, NCgrel AD, Pararajasegaram costeroid treatment in children. AmerJDis
Furthermore, as mentioned earlier, it is R, Dadzie W,Global data on blindness. Bull Child 1968; 1 16: 604-608.
highly unlikely that protein modification W O 1995; 73: 115121. 18. Hardie I, Matsunami C, Hilton A, Dyer J,
is the cause of steroid cataract. 2. Ohrloff C, Hockwin 0,Muller-Breitenkamp Rumbach 0. Ocular complications in re-
Although there is a great need to de- U. Cataract. Aspects of physiology pathol- nal transplant recipients. Trans A o r 1992;
velop a treatment for steroid-induced PSC ogy and epidemiology. Med Monastsschr 24: 177.
Pham 1993; 1 6 162-171. 19. Kollaritis CR, Swann ER, Shapiro RS,
or a means for preventing this unwanted
3. Harding J. The epidemiology of cataract. Gillespie CM, Shealy TA. HLA-AI and ster-
side-effect by modification of the steroid In: Harding J, ed. Cataract: Biochemistry oid induced cataracts in renal transplant pa-
or its vehicle, this seems a considerable way Epidemiology and Pharmacology.London: tients. Ann Ophthalmol1982; 14: l 1 1 6 1 118.
off.Furthermore, despite the enthusiastic Chapman and Hall, 1991; 83-124. 20. BrocklebankJT, Harcourt RB, Meadow SR.
claims by some researchers and market- 4. Urban RC Jnr, Cotlier E. Corticosteroid- Corticosteroid induced cataracts in idi-
induced cataracts. Sun,Ophthalmol1986;31: opathic nephrotic syndrome. ArchDzs Child
ing agencies, no effective treatments,
102-110. 1982; 57: 30-34.
other than surgical removal of the lens, 5. Black RL, Oglesby RB, von Sallmann L, 21. Donshik PC, Cavanaugh HD, Boruchoff SA,
are available for treating any form of cata- Bunim JJ. Posterior subcapsular cataracts Dohlman CH. Posterior subcapsular cata-
ract. induced by corticosteroids in patients with racts induced by topical corticosteroids fol-
rheumatoid arthritis. J A M 1960; 174 150- lowing keratoplasty for keratoconus. Ann
155. OPhthalmol1981; 13: 29-32.
CONCLUSION 6. Oglesby RB, Black RL, von Sallmann L, 22. Llmaye SR, Pillai S, Tina LU. Relationship
~
Bunim JJ. Cataracts in rheumatoid arthri- of steroid dose to degree of posterior sub-
The development of steroid-induced pos- tis patients treated with corticosteroids. capsular cataracts in nephrotic syndrome.
terior subcapsular cataract is complex and Arch Ophthalmoll961;66: 519-523. Ann Ophthalmoll988; 20: 225227.
much work is needed to elucidate the 7. Crews SJ. Posterior subcapsular lens opaci- 23. Valerio M. Les dangers de la cortisono-
mechanism. Attempts have been made to ties in patients on long-term corticosteroid thirapie locale prolongie. Bull Mem Sor Fr
therapy. Br MedJ 1963; 5346: 16441647. Ophtalmoll963; 76: 572-580.
adapt mechanisms, such as oxidation, os- 24. McLean CJ, Lob0 RF, Brazier DJ. Cataracts
8. Fryer JP, Granger DK, Leventhal JR,
motic change and conformational change, Gillingham K, Najarian JS, Matas AJ. glaucoma and femoral avascular necrosis
I
proposed for other types of cataract. How- Steroid-related complications in the caused by topical corticosteroid ointment.
ever, the unique clinical manifestations of cyclosporine era. Clin Transplant 1994; 8: Lancet 1995; 345: 330.
steroid cataracts make it unlikely that any 224229. 25. Renfro L, Snow JS. Ocular effects of topi-
9. Spencer RW, Andelman W. Steroid cata- cal and systemic steroids. Dermatol Clin
of these would be applicable. Most of the
racts. Posterior subcapsular cataract forma- 1992; 10: 505-512.
more specific theories proposed lack con- tion in rheumatoid arthritis patients on 26. Costagliola C, Cati-GiovannelliB, Piccirillo
vincing experimental or clinical support- long-term steroid therapy. Arch Ophthalmol A, Delfino M. Cataracts associated with
ing evidence. 1965; 74: 38-41. long-term topical steroids. Er J Dmatol
A promising new possibility is that of 10. Lindholm B, Linner E, Tengroth B. Effects 1989; 120: 472-473.
of long-term systemic steroids on cataract 27. Gasset AR, Bellows RT. Posterior subcapsu-
ocular growth factor imbalance leading to
formation and on aqueous humour dynam- lar cataracts after topical corticosteroid
aberrant cell behaviour. It is only in recent ics. Acta Ophthalmol1965; 43: 120-127. therapy. Ann Ophthalmoll974; 6: 1263-1265.
years that the importance of growth fac- 11. Kennedy I. Cortisone-induced opacities of 28. Abuekteish F, Kirkpatrick J N , Russell G.
tors in normal eye development and the crystalline lens. Trans Aust Coll Posterior subcapsular cataract and inhaled
growth has been recognised. The specific Ophthalmoll970;2: 28-32. corticosteroid therapy. Thorax 1995; 50:
factors that may be involved in cataract 12. Leroux RC, Biojout G, Meyrier A, SraerJD. 674676.
Ocular complications in renal transplanta- 29. Fraunfelder FT,Meyer SM. Posterior sub-
formation remain to be determined. In- tion. Br MedJ 1972; 3: 586. capsular cataracts associated with nasal or
vestigations on the role of various growth 13. Drobecka BE. Effect of immunosuppressive inhalation corticosteroids. AmJ Ophthalmol
factors and combinations of factors are treatment on the crystalline lenses of pa- 1990; 109: 489-490.
needed. It may then be possible to develop tients after kidney transplantation. Klin 30. Barnes NC. Safety of high-dose inhaled
Clinical and Experimental Optometry 85.2 March 2002
72
Steroid cataracts Jobling and Augusteyn
corticosteroids. Respir Med 1993; 87 (Suppl 1972; 88: 439-460. 65. Miller D, Tijerina ML, Mayman C. In uitm
A): 27-31. 49. Wander AH. Herpes simplex virus and re- production of steroid cataract in bovine
31. Taub SJ. The incidence of cataracts in ster- current corneal disease. Int Ophthalmol Clin lens. Part 1: measurement of optical
oid treated children. Eye Ear Nose Throat 1984; 24: 27-38. changes. Arta Ophthalmol 1979; 57: 1101-
Month 1968; 47: 133-134. 50. Fechner PU, Wishmann W. Retarded 1106.
32. Sevel D, Weinberg EG, van-Niekerk CH. corneosceral wound healing associated 66. Creighton MO, Sanwal M, Stewart-DeHaan
Lenticular complications of long-term ster- with high postoperative doses of systemic PJ, Trevithick JR. Modeling cortical
oid therapy in children with asthma and steroids in glaucoma surgery. Refract Corneal cataractogenesis V. Steroid cataracts in-
eczema. J A l k g y Clin Immunoll977; 60: 215- Surg1991; 7 : 174176. duced by Solumedrol partially prevented
217. 51. von Sallmann L, Caravaggio LL, Collins by vitamin E in vitm. Exp Eye Res 1983; 37:
33. Kaye LD, Kalenak JW, Price RL, EM, Weaver K. Examination of lenses of 65-75.
Cunningham R. Ocular implications of steroid treated rats. Am J Ophthalmol 1960; 67. Korte I , Hockwin 0, Fischer H, Klemm H,
long-term prednisone therapy in children. 50: 1147-1151. Kraft U. Studies o n the influence of
JPediatr OphthalmolStrab 1993; 30: 142-144. 52. Spencer RW, Andelman SY. Steroid cata- corticosteroids o n the carbohydrate me-
34. Dikshit SK, Avasthi PN. Posterior lenticu- racts. Posterior subcapsular cataract forma- tabolism of calf and bovine lenses in uitm.
lar opacities in children on corticosteroid tion in rheumatoid arthritis patients on Jap JOphthalmol1976; 20: 20421 1.
therapy. Indian J Pediatr 1965; 32: 93-96. long-term steroid therapy. Arch Ophthalmol 68. Nishigori H, Lee JW, Yamauchi Y,
35. Forman AR, Loreto JA, Tina LU. Revers- 1965; 74: 38-41. Maruyama K, Iwatsuru M. Analysis of glu-
ibility of corticosteroid-associated cataracts 53. Bettman JW, Thompson F, d e Baskey R. cose levels during glucocorticoid-induced
in children with the nephrotic syndrome. Cataractogenic effect of steroids. Invest formation in chick embryos. Invest
Am J Ophthahol1977; 84: 75-78. Ophthalmoll963; 2: 101. Ophthalmol Vis Sci 1987; 28: 168-174.
36. Rubin B, Palestine AG. Complications of 54. Bettman JW, Noyes P, de Baskey R. The 69. Hockwin 0 ,Ohrloff C, Koch H.R. Licht W,
corticosteroid a n d immunosuppressive potentiating action of steroids in cataracto- No11 E. Effects of several corticosteroids on
drugs. Int Ophthalmol Clin 1989;29: 159-171. genesis. Invest Ophthalmoll964; 3: 459. enzymes of the carbohydrate metabolism
37. Spate GL, von Sallmann L. Corticosteroids 55. Wood DC, Contaxis I, Sweet D, Smith JC, of the lens. Pror European Sor Drug 7oxicily
and cataracts. Int Ophthalmol Clin 1966; 6: van Dolah J . Response of rabbits to 1973; 15: 59-62.
91 5-929. corticosteroids. Am J Ophthalmol 1967; 63: 70. Raineri R, L e y HR. On the specificity of
38. Schroepfer GJ Jnr. Sterol biosynthesis. Ann 841-856. steroid interaction with mammary glucose
Rev Biochem 1982; 51: 555-585. 56. Tarkkanen A, Esili R, Liesmaa M. Experi- 6phosphate dehydrogenase. Biorhem 1970;
39. Hammond EW. General principles of mental cataracts following long-term ad- 9: 2233-2243.
corticosteroids. In: Freeman JS Jnr, ed. ministration of corticosteroids. Arch 71. Charlton JM, van Heyningen R. Glucose-6
Clinical Optometric Pharmacology and Ophthalmol1966; 44: 665668. phosphate dehydrogenase in the mamma-
Therapeutics. Philadelphia: JB Lippincott 57. Leske MC, Chylack LTJnr, Wu SY.The lens lian lens. Exp Eye Res 1971; l l : 147-160.
Company, 1993; 1-1 1. opacities case control study. Risk factors for 72. Greiner JV. Kopp SJ, Glonek T. Dynamic
40. Hench PS, Kendall EC, Slocumb CH, Polley cataract. Arch Ophthalmol 1991; 109: 2 4 4 changes in the organophosphate profile
HS. Effect of hormone of adrenal cortex 251. upon treatment of the crystalline lens with
17- hydroxy-1 Id-hydro corticosterone com- 58. Bucala R, Gallati M, Manabe S, Cotlier E, dexamethasone. Invest Ophthalmol Vis Sri
pound E and of pituitary adrenocortico- Cerami A. Glucocorticoid-lens protein ad- 198'2; 23: 1422.
tropic hormone on rheumatoid arthritis. ducts in experimentally induced steroid 73. Olgemdller B, Schleicher ED, Gerbitz KD.
Preliminary report. Mayo Clinic Pror 1949; cataracts. Exp Eye Res 1985; 40: 853-863. Differential kinetics of glucose metabohsm
24: 181-197. 59. Rogoyski A, Trzcinska-Dabrowska Z. Corti- in porcine retinal and aortic endothelial
41. Oksala A. Treatment of traumatic costeroid induced cataract and palato- cells. JClin Chem Biorhem 1990; 28: 15-17.
hyphaema. Er J Ophthalmol 1967; 51: 315- schisis in the mouse foetus. AmJOphthalmol 74. OlgemBller B, Schdn J , Wieland OH.
320. 1969; 68: 128133. Endothelial plasma membrane is a gluco-
42. Laatikainen L, Tarkkanen A. Management 60. H a u m o n t ST. Effets d e la cortisone corticoid-regulated barrier for the uptake
of purulent postoperative endophthalmitis. administrie pendant la gestation. A n n of glucose into the cell. Mol Cell Endorrinol
Ophlhalmologira 1986; 193: 3438. d'Endom'no 1958; 19: 442-445. 1985; 43: 165-171.
43. Herbort CP. Uveoscleritis after excessive 61. Koksma JMA, Hoyng PFJ, Willekens BW. 75. Jobling AI, Augusteyn RC. Is there a gluco-
neodymium: YAG laser posterior capsu- Lens deviations in rabbit offspring after corticoid receptor in the bovine lens? Exp
lotomy. J Cat Refrart Surg 1994; 20: 80-81. short-term prenatal exposure to dexam- Eye Re$ 2001; 72: 687-694.
44. Corboy JM. Corticosteroid therapy for the ethasone: A light microscopic study. Exp Eye 76. Fussel JC, Kelly FJ. Effects of dexametha-
reduction of postoperative inflammation Res 1984; 39: 195-206. sone on lung protein turnover. Biochem J
after cataract extraction. Am J Ophthalmol 62. Nishigori H, Lee J, Iwatsuru M. An animal 1991; 273: 93-97.
1976; 82: 923-927. model for cataract research: cataract forma- 77. Friedburg D, KrBner H, Rosenstiel L. In
45. Barry JM. Immunosuppressive drugs in re- tion in the developing chick embryo by glu- uivo action ofcorticosteroids on the guinea
nal transplantation. A review of the regi- cocorticoid. Exp Eye Res 1983; 36: 617-622. pig lens. Ophthal Res 1974; 6: 131-137.
mens. Drugs 1992; 44: 554566. 63. SivakJG,Yoshimura M, Weerheim J, Dorvat 78. van Venrooij WJ, Groeneveld AA,
46. Arrnaly MA. Corticosteroid glaucoma. In: A. Effect of hydrogen peroxide DL- Bloemendal H. Cultured calf lens epithe-
Cairns JE, ed. Glaucoma vol 11. London: propranolol and prednisone on bovine lens lium. 11. The effect of dexametliasone. Exp
Grune and Stratton Ltd, 1986; 697-710. optical function in culture. Invest Eye Res 1974; 18: 527-536.
47. Renfro L, Snow JS. Ocular effects of topi- Ophthahol Vis Sci 1990; 3 1: 954963. 79. Arase S , Nagai R, Nakanishi H, Takeda K.
cal and systemic steroids. Dermatol Clin 64. Haddad HM, Furman M, Bella Shore MS. Effects of six topical corticosteroids on DNA
1992; 10: 505-512. Lens organ culture 11. Pharmacological ewlu- synthesis of normal human skin fibroblasts.
48. Armaly MF. Glaucoma. Arch Ophthalmol ation. Am JOphthalmol1967; 63: 1737-1743. Tokushima,]Med 1988; 35: 1-4.
Clinical and Experimental Optometry 85.2 March 2002
73
Steroid cataracts Jobling and Augusteyn
80. HeffernanJT, Futterman S, Kalina RE. Dex- 1997; 65: 507-516. Optom 1999; 82:130-135
amethasone inhibition of experimental 97. Richer S. Antioxidants and the eye. Int 111. Muller M, Renkawitz R. The glucocorti-
endothelial cell proliferation in retinal Ophthalmol Clin 2000; 40: 1-16. coid receptor. Biochim Biophys Acta 1991;
venules. Invest Ophthalmol Vis Sci 1978; 17: 98. Costagliola C, Iuliano G, Menzione M, 1088: 171-182.
565-568. Apponi-Battini G, Auricchio G. Effect of 112. Weinstein BI, Altman K, Gordan GG,
81. Boneham GC, Collin HB. Steroid inhibi- topical glucocorticoid administration on Dunn M, Southren AL. Specific glucocor-
tion of limbal blood and lymphatic vascu- the protein and nonprotein sulfhydryl ticoid receptor in the irisciliary body of the
lar cell growth. Curr Eye Res 1994; 1 4 1-10, groups of the rabbit lens. OphthalRes1987; rabbit. Invest Ophthalmol Vis Sci 1977; 16:
82. He S, Wang H, Ye J, Ogden TE, Ryan SJ, 19: 351-356. 973-976.
Hinton DR. Dexamethasone induced pro- 99. Nishigori H, LeeJW, Yamauchi Y, Iwatsuru 13. Southren AL, Gordan GG,Yeh HS, Dunn
liferation of cultured retinal pigment epi- M. The alteration of lipid peroxide in M, Weinstein BI. Nuclear translocation of
thelial cells. CurrEyeRes 1994; 13: 257-261. glucocorticoid-inducedcataract of develop the cytoplasmic glucocorticoid receptor in
83. Hirano H. In vitro effects of flavin adenine ing chick embryos and the effect of ascor- the iris-ciliary body of the rabbit. Invest
dinucleotide and dexamethasone phos- bic acid. Curr Eye Res 1986 5: 37-40. Ophthalmol Vis Sci 1979; 18: 517-521.
phate on high molecular weight phosphate 100. Nishigori H. Hayashi R, LeeJW, Iwatsuru 14. Southren AL, Gordan GG,Yeh HS, Dunn
compounds in the rat lens. ZntJ Vit Nutr M. Effect of MPG on glucocorticoid in- M, Weinstein BI. Receptors for gluco-
R ~ 1977;
s 47: 151-156. duced cataract formation in developing corticoids in the lens epithelium of the calf.
84. Jacob TJC, Karim AKA, Thompson GM. chickembryo. Invest OphthalmolVisSci 1984; Science 1978; 200 1177-1178.
The effects of steroids on human lens epi- 25: 1051-1055. 115. Wenk EJ, Hernandez MR, Weinstein BI,
thelium. Eye 1987; 1: 722-727. 101. Koenig RJ, Cerami A. Haemoglobin A,c Gordan GG, Dunn M, Southren AL. Glu-
85. Skou JC. The Na K-Pump. Meth Enzymology and diabetes mellitus. Ann Reu Med 1980; cocorticoid receptor binding in the bovine
1988; 156: 1-25. 31: 29-34. lens. Invest Ophthalmol Vis Sci 1982; 22: 599-
86. Bonting SL, Caravaggio LL, Hawkins NM. 102. Stevens VJ,Fantl WJ, Newman CB, Sims 605.
Studies on sodium-potassiumactivated ad- RV, Cerami A, Peterson CM. Acetylal- 116. BaxterJD, Tomkins GM. Specific cytoplas-
enosine triphosphatase VI:its role in cation dehyde adducts with haemoglobin. J Clin mic glucocorticoid hormone receptors in
transport in the cat calf and rabbit. Arch Invest 1981; 67: 361-369. hepatoma tissue culture cells. Cardiovasr Res
Biochem 1963; 101: 47-55. 103. Koenig RJ, Peterson CM, Jones RL, 1971; 33: 272-283.
87. BellowsJG. Cataract and Abnormalities of Saudek C, Lehrman M, Cerami A. Correla- 117. Funder JM, BarlowJW. Heterogeneity of
the Lens. St Louis: CV Mosby, 1944; 147- tion of glucose regulation and haemo- glucocorticoid receptors. Circ Res 1980; 46:
153. globin A,<in diabetes mellitus. NEnglJMed 1-83.
88. Harris JE, Gruber L. The electrolyte and 1976; 295: 417-420. 118. Tchernitchin A, Wenk EJ, Hernandez MR,
water balance of the lens. Exp Eye Res 1962; 104. Stevens VJ, Rouzer C, Monnier VM, Weinstein BI, Dunn M, Gordan GG et al.
1: 372-384. Cerami A. Diabetic cataract formation: Glucocorticoid localisation by radioautog-
89. Mayman CI. Inhibitory effect of dexametha- potential role of glycosylation of lens raphy in the rabbit eye following systemic
sone on sodium-potassiumactivated adeno- crystallins. Proc NatlAcad Sci 1978; 75: 2918 administration of SHdexamethasone. Invest
sine triphosphatase of choroid plexus in cat 2922. Ophthalmol Vis Sci 1980; 19: 1231-1236.
and rabbit. Fed Aoc 1972; 31: 591693. 05. Beswick H, Harding J. Conformational 119. Jobling AI, Stevens A, Augusteyn RC.
90. Rodriguez H, Sinha S, Starling J, Klahr S. changes induced in alphacrystallins by pro- Binding of dexamethasone by a-crystallin.
Regulation of Na-K-ATPase in the rat by tein carbamylation.BiochemJ1984; 223 221- Invest Ophthal Vis Sci 2001; 42: 1829-1832.
adrenal steroids. AmJPhysiol1981; 241: 186- 227. 120. StokesJ, NobleJ, Brett L, Phillips C, Seckl
195. 06. Garner B, Shaw DC, Lindner RA, Carver JR, OBrien C et al. Distribution of gluco-
91. Celsi G, Wang ZM, Akusjirvi G, Aperia A. JA, Truscott RJ. Non-oxidative modification corticoid and mineralocorticoid receptors
Sensitive periods for glucocorticoidsregu- of lens crystallins by kynurenine: a novel and beta-hydroxysteroid dehydrogenases in
lation of Na+K-ATPasemRNA in the devel- post-translational protein modification with human and rat ocular tissues. Invest
oping lung and kidney. Pediatr Res 1993;33: possible relevance-to ageing and cataract. Ophthalmol Vis Sa2000; 41: 1629-1638.
5-9. Biochim Biophys Acta 2000; 1476 ~265278. 121. Hanna C, OBrien JE. Cell production
92. Mayman C1, Miller D, Tijerina ML. In vitro 107. Bucala R, Fishman J, Cerami A. Forma- and migration in the epithelial layer of the
production of steroid cataract in bovine tion of covalent adducts between cortisol lens. Arch Ophthalmol1961; 66: 103-107.
lens. Part 11: Measurement of sodium- and 16a-hydroxyestrone and protein: Pos- 122. Coulombre JL, Coulombre AJ. Lens de-
potassium adenosine triphosphatase activ- sible role in the pathogenesis of cortisol velopment: Fibre elongation and lens ori-
ity. Acta Ophthalmoll979;57: 1107-1116. toxicity and systemic lupus erythematosus. entation. Science 1963; 142: 1489-1490.
93. Kana JS, Wiederholt M. Effect of cortico- Proc Natl Acad Sci 1982; 79: 3320-3324. 23. McAvoyJW, Chamberlain CG. Fibroblast
steroids on electrolyte transport of isolated 108. Manabe S, Bucala R, Cerami A. Nonenzy- growth factor (FGF) induces different re-
human and rabbit lens. Curr Eye Res 1985; matic addition of glucocorticoids to lens sponses in lens epithelial cells depending
4: 461-465. proteins in steroid-induced cataracts.J Clin on its concentration. Development 1989; 107:
94. Cotlier E, Becker B. Topical corticosteroids Invest 1984; 74: 1803-1810. 221-228.
and galactose cataracts. Invest Ophthalmol 109. Bucala R, Manabe S, Urban RC, Cerami 24. Schulz M, Chamberlain CG, de longh RU,
1965; 4 806-814. A. Nonenzymatic modification of lens McAvoyJW. Acidic and basic FGF in ocular
95. Becker B, Cotlier E. The efflux of @rubid- crystallins by prednisolone induces media and lens: Implications for lens po-
ium from the rabbit lens. Invest Ophthalmol sulfhydryl oxidation and aggregate forma- larity and growth patterns. Development
1965; 4: 117-121. tion: In vitm and in vivo studies. Exp Eye Res 1993; 118: 117-126.
96. Dickerson JE, Dotzel E, Clark AF. Steroid- 1985; 41: 353-363. 125. Yamamoto Y. Growth of lens and ocular
induced cataract: new perspectives from in 110. Jobling AI, Augusteyn RC. Steroid adduct environment: Role of neutral retina in the
vitro and lens culture studies. Exp Eye Res formation with lens crystallins. Clin Exp growth of mouse lens as revealed by an
Clinical and ExperimentalOptometry 85.2 March 2002
74
Steroid cataracts Jobling and Auguskyn
implantation experiment. Dm Growth Off
1976;18: 273278.
126. Schlotzer-Schrehardt U , Dorfler S.
Immunolocalization of growth factors in
the human ciliary body. Cum Eye Res 1993;
12: 893-905.
127. Hales AM, Chamberlain CG, Dreher B,
McAvoy JW.Intravitreal injection of TGF
beta induces cataract in rats. Invest
Ophlhalmol Vis Sri 1999;40:3231-3236
128. Nishigori H, Lee JW, Iwatsuru M.
Glucocorticoid-induced cataract of the
developing chick embryo-prevention by
polyethylene glycol. Ophlhal Res 1995; 27:
350-355.
129. Cotlier E, Sharma YR. Aspirin and senile
cataracts in rheumatoid arthritis. Lancet
1981;1: 338-339.
130. Crompton M, Rixon KC, HardingJ. As-
pirin prevents carbamylation of soluble lens
proteins and prevents cyanate-induced
phase separation opacities in d r o : A possi-
ble mechanism by which aspirin could pre-
vent cataract. ExpEyeRes 1985;40: 297-31I.
131. Seigel D, Sperduto RD, Ferris ZFL. Is ASA
therapy for cataracts justified? C a n J
Ophthalmoll982;17:135-136.
Authors address:
Professor RC Augusteyn
National Vision Research Institute of
Australia
386 Cardigan Street
Carlton VIC 3053
AUSTRALIA
Clinical and Experimental Optometry 85.2 March 2002
75
Anda mungkin juga menyukai
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5795)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (74)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1091)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- IVT Network - Process Validation - 2014-04-28Dokumen1 halamanIVT Network - Process Validation - 2014-04-28Mina Maher MikhailBelum ada peringkat
- 3304 Part B DCHB Vellore PDFDokumen432 halaman3304 Part B DCHB Vellore PDFrajashekhar asBelum ada peringkat
- SPF 55 BrochureDokumen2 halamanSPF 55 Brochureapi-528907705Belum ada peringkat
- Self Managed TeamsDokumen13 halamanSelf Managed TeamsSiraj SiddiquiBelum ada peringkat
- Nursing TheoryDokumen13 halamanNursing TheoryYana VictyBelum ada peringkat
- 51 - Methemoglobin ProducersDokumen20 halaman51 - Methemoglobin ProducersCabinet VeterinarBelum ada peringkat
- Adoption Authorities and Agencies Under Juvenile Justice Act, 2015Dokumen10 halamanAdoption Authorities and Agencies Under Juvenile Justice Act, 2015DebanjanaChakrabortyBelum ada peringkat
- Nurs 3021 Midterm Evaluation - Blessing Nwogu 1Dokumen17 halamanNurs 3021 Midterm Evaluation - Blessing Nwogu 1api-673227957Belum ada peringkat
- SPA vs. GPADokumen24 halamanSPA vs. GPAYabb TabianBelum ada peringkat
- Accident Cause, Cost & Prevention (Cery Very Good) Final-1Dokumen251 halamanAccident Cause, Cost & Prevention (Cery Very Good) Final-1KezBelum ada peringkat
- Learning Module 4 Layers Bio-Security, Vaccination and Cleaning Poultry HousesDokumen30 halamanLearning Module 4 Layers Bio-Security, Vaccination and Cleaning Poultry HousesTshegofatsoBelum ada peringkat
- WECOC Final Announcement 29th CompressedDokumen32 halamanWECOC Final Announcement 29th CompressedChristabella Natalia WijayaBelum ada peringkat
- UN PolicyDokumen2 halamanUN PolicySomeoneBelum ada peringkat
- FWD Corporate Care Presentation v06Dokumen18 halamanFWD Corporate Care Presentation v06Anonymous 1QUrY04kLw100% (1)
- CSCRDokumen26 halamanCSCRАнагаахын ОрчуулгаBelum ada peringkat
- Risk Management AwarenessDokumen19 halamanRisk Management AwarenessRamalingam ChandrasekharanBelum ada peringkat
- Sensors 22 08161 v2Dokumen20 halamanSensors 22 08161 v2Kristian DokicBelum ada peringkat
- Dalal & MishraDokumen491 halamanDalal & MishraKarthika M TharakanBelum ada peringkat
- Cognitive-Behavioral Therapy: Instructor's ManualDokumen68 halamanCognitive-Behavioral Therapy: Instructor's ManualzingpalmsBelum ada peringkat
- Clinical Evaluation and Management of Spasticity PDFDokumen397 halamanClinical Evaluation and Management of Spasticity PDFRicardo Pedro100% (1)
- Method Statement For Lifting WorksDokumen12 halamanMethod Statement For Lifting WorksRachel Flores85% (26)
- Accreditation Standards For Advanced Dental Education Programs in EndodonticsDokumen30 halamanAccreditation Standards For Advanced Dental Education Programs in Endodonticsjenea tBelum ada peringkat
- Cata 2012Dokumen288 halamanCata 2012kiskalpBelum ada peringkat
- Generalized Anxiety Disorder Case Study 2017Dokumen4 halamanGeneralized Anxiety Disorder Case Study 2017Pratik SinghBelum ada peringkat
- Symposium On Drug Awareness - Narrative ReportDokumen2 halamanSymposium On Drug Awareness - Narrative ReportRey Salomon Vistal100% (9)
- California Retailers Guide To Hazardous Waste ComplianceDokumen4 halamanCalifornia Retailers Guide To Hazardous Waste ComplianceStericycle100% (1)
- Elca/Cspm Final Exam 2007 14 July, 2007Dokumen23 halamanElca/Cspm Final Exam 2007 14 July, 2007Dr Atef Hadedy100% (3)
- Methods of Endotoxin Removal From Biological PreparationsDokumen17 halamanMethods of Endotoxin Removal From Biological PreparationsexecBelum ada peringkat
- Chapter 16, Modern Advanced Accounting-Review Q & ExrDokumen25 halamanChapter 16, Modern Advanced Accounting-Review Q & Exrrlg4814100% (4)
- Emergency HandbookDokumen96 halamanEmergency HandbookZenith Sabando Manawatao100% (1)