Anda mungkin juga menyukai
- Abdominal Organ Transplantation: State of the ArtDari EverandAbdominal Organ Transplantation: State of the ArtNizam MamodeBelum ada peringkat
- Care of The Patient in The Perioperative PeriodDokumen20 halamanCare of The Patient in The Perioperative PeriodMohammed FaragBelum ada peringkat
- Perioperative Management of Patients Receiving Anticoagulants - UpToDateDokumen65 halamanPerioperative Management of Patients Receiving Anticoagulants - UpToDatejames lxBelum ada peringkat
- Neuraxial Anesthesia - Analgesia Techniques in The Patient Receiving Anticoagulant or Antiplatelet Medication - UpToDateDokumen25 halamanNeuraxial Anesthesia - Analgesia Techniques in The Patient Receiving Anticoagulant or Antiplatelet Medication - UpToDatemago1961100% (1)
- Complications of PCNL: DR - Sanjay S Deshpande Sidheshwar Urological Society SolapurDokumen20 halamanComplications of PCNL: DR - Sanjay S Deshpande Sidheshwar Urological Society SolapurAlat MasakBelum ada peringkat
- Conservative Management of Perforated Peptic UlcerDokumen4 halamanConservative Management of Perforated Peptic UlcerAfiani JannahBelum ada peringkat
- Color Code AnesthesiaDokumen6 halamanColor Code AnesthesiaYusnia Gulfa MaharaniBelum ada peringkat
- Initial Management of Trauma in Adults - UpToDateDokumen37 halamanInitial Management of Trauma in Adults - UpToDateAlberto Kenyo Riofrio PalaciosBelum ada peringkat
- Post Op DeliriumDokumen26 halamanPost Op DeliriumKannan GBelum ada peringkat
- Definition, Classification, Etiology, and Pathophysiology of Shock in Adults - UpToDateDokumen20 halamanDefinition, Classification, Etiology, and Pathophysiology of Shock in Adults - UpToDateEstructuración Técnica 2019Belum ada peringkat
- Antimicrobial Prophylaxis For Prevention of Surgical Site Infection in AdultsDokumen59 halamanAntimicrobial Prophylaxis For Prevention of Surgical Site Infection in Adultsbolohan biatriceBelum ada peringkat
- Management of Acute Pancreatitis - UpToDateDokumen33 halamanManagement of Acute Pancreatitis - UpToDateCesar Luna RamirezBelum ada peringkat
- Postcholecystectomy SyndromeDokumen27 halamanPostcholecystectomy SyndromeMonica TurnerBelum ada peringkat
- Overview of Topical Hemostatic Agents and Tissue Adhesives - UpToDateDokumen37 halamanOverview of Topical Hemostatic Agents and Tissue Adhesives - UpToDatePepe P. AlfssonBelum ada peringkat
- Obstetrics AnesthesiaDokumen31 halamanObstetrics AnesthesiaNorfarhanah ZakariaBelum ada peringkat
- Causes of Upper Gastrointestinal Bleeding in Adults - UpToDateDokumen37 halamanCauses of Upper Gastrointestinal Bleeding in Adults - UpToDateAline MoraisBelum ada peringkat
- Atlas of Gastrointestinal Endoscopy and Related PathologyDokumen2 halamanAtlas of Gastrointestinal Endoscopy and Related PathologyMaria PatituBelum ada peringkat
- Perioperative ManagementDokumen3 halamanPerioperative ManagementRaymond De GulaBelum ada peringkat
- Approach To The Adult With Unexplained Thrombocytopenia - UpToDateDokumen65 halamanApproach To The Adult With Unexplained Thrombocytopenia - UpToDateMagdy GabrBelum ada peringkat
- General SurgeryDokumen18 halamanGeneral SurgeryYogesh KharcheBelum ada peringkat
- Surgical Management of ObesityDokumen13 halamanSurgical Management of Obesityمحمد حميدانBelum ada peringkat
- Use of Blood Products in The Critically Ill - UpToDateDokumen13 halamanUse of Blood Products in The Critically Ill - UpToDateOscar F RojasBelum ada peringkat
- (HLMN 5-19) Evaluation of The Adult With Abdominal Pain - UpToDateDokumen21 halaman(HLMN 5-19) Evaluation of The Adult With Abdominal Pain - UpToDateandylumanBelum ada peringkat
- Proton Pump Inhibitors - The Beginning of The End or The End of The Beginning PDFDokumen8 halamanProton Pump Inhibitors - The Beginning of The End or The End of The Beginning PDFbravohr98Belum ada peringkat
- Day Care SurgeryDokumen5 halamanDay Care SurgeryazharmoBelum ada peringkat
- CME Trunk, Abdomen, and Pressure Sore ReconstructionDokumen15 halamanCME Trunk, Abdomen, and Pressure Sore ReconstructionVeronica TomaselloBelum ada peringkat
- Pre Op 2010Dokumen37 halamanPre Op 2010Tawona DhlakamaBelum ada peringkat
- Phyllodes Tumors of The Breast UpToDateDokumen22 halamanPhyllodes Tumors of The Breast UpToDateSean SialanaBelum ada peringkat
- 3.preoperative Patient Assessment and ManagementDokumen76 halaman3.preoperative Patient Assessment and Managementoliyad alemayehuBelum ada peringkat
- UCL Aneasthesia Year 4 Workbookv15Dokumen83 halamanUCL Aneasthesia Year 4 Workbookv15Jay KayBelum ada peringkat
- Overview of Complications Occurring in The Post-Anesthesia Care UnitDokumen14 halamanOverview of Complications Occurring in The Post-Anesthesia Care UnitShahabuddin ShaikhBelum ada peringkat
- Preanesthesia Evaluation For Noncardiac Surgery - UpToDate PDFDokumen86 halamanPreanesthesia Evaluation For Noncardiac Surgery - UpToDate PDFCharlie Bellow100% (1)
- Overview of Management of Mechanical Small Bowel Obstruction in Adults - UpToDateDokumen19 halamanOverview of Management of Mechanical Small Bowel Obstruction in Adults - UpToDateDesak PramestiBelum ada peringkat
- Pharmacotherapy During Pregnancy, Childbirth and Lactation: Principles To ConsiderDokumen7 halamanPharmacotherapy During Pregnancy, Childbirth and Lactation: Principles To Consideryuliana nurcahyatiBelum ada peringkat
- American College of Surgeons and Surgical Infection Society - Surgical Site Infection Guidelines, 2016 Update (SSI)Dokumen16 halamanAmerican College of Surgeons and Surgical Infection Society - Surgical Site Infection Guidelines, 2016 Update (SSI)Anonymous LnWIBo1GBelum ada peringkat
- Definition, Classification, Etiology, and Pathophysiology of Shock in Adults - UpToDateDokumen16 halamanDefinition, Classification, Etiology, and Pathophysiology of Shock in Adults - UpToDatevara prasadBelum ada peringkat
- Diagnosis and Acute Management of Suspected Nephrolithiasis in Adults - UpToDateDokumen44 halamanDiagnosis and Acute Management of Suspected Nephrolithiasis in Adults - UpToDateManu Luciano100% (1)
- Shock On TraumaDokumen36 halamanShock On TraumaMeviraf BennyBelum ada peringkat
- Laparoscopic Gastrointestinal SurgeryDokumen22 halamanLaparoscopic Gastrointestinal SurgeryRoxana BoloagaBelum ada peringkat
- Postoperative Peritoneal Adhesions in Adults and Their Prevention - UpToDateDokumen17 halamanPostoperative Peritoneal Adhesions in Adults and Their Prevention - UpToDateDesak PramestiBelum ada peringkat
- Acid Related DisordersDokumen18 halamanAcid Related DisordersMinto SanjoyoBelum ada peringkat
- Elsevier - Anaesthesiology Clinics - Vol.26, Issues 1 - Obstetric Anesthesia (2008) PDFDokumen230 halamanElsevier - Anaesthesiology Clinics - Vol.26, Issues 1 - Obstetric Anesthesia (2008) PDFMila KarmilaBelum ada peringkat
- Airway Management Inside and Outside Operating Rooms 2018 British Journal ofDokumen3 halamanAirway Management Inside and Outside Operating Rooms 2018 British Journal ofSeveNBelum ada peringkat
- Factors Affectin Block HeightDokumen37 halamanFactors Affectin Block HeightshikhaBelum ada peringkat
- Practice Guidelines For Juniors 01 June 2016Dokumen3 halamanPractice Guidelines For Juniors 01 June 2016ElaineBelum ada peringkat
- Manejo de Las Crisis en Anestesia - Gaba 2 Ed PDFDokumen424 halamanManejo de Las Crisis en Anestesia - Gaba 2 Ed PDFdianisssuxBelum ada peringkat
- Abdominal Wall IncisionDokumen42 halamanAbdominal Wall IncisionURo KkuBelum ada peringkat
- Trauma and Acute Care SurgeryDokumen24 halamanTrauma and Acute Care SurgeryPar Do100% (1)
- Murmur EvaluationDokumen4 halamanMurmur EvaluationManjunath GeminiBelum ada peringkat
- Perioperative Laboratorytesting - The ClinicsDokumen6 halamanPerioperative Laboratorytesting - The Clinicsapi-265532519Belum ada peringkat
- Use of Vasopressors and Inotropes - UpToDateDokumen18 halamanUse of Vasopressors and Inotropes - UpToDateAlbertoMarteBelum ada peringkat
- Principles of Bariatric and Metabolic SurgeryDokumen51 halamanPrinciples of Bariatric and Metabolic SurgeryDr Shahzad Alam ShahBelum ada peringkat
- Max Surgical Blood Order PDFDokumen6 halamanMax Surgical Blood Order PDFatina putriBelum ada peringkat
- Sedation and Analgesia in The Intubated Patient (Adult Critical Care)Dokumen12 halamanSedation and Analgesia in The Intubated Patient (Adult Critical Care)Beatriz Maria Espinosa HernandezBelum ada peringkat
- Treatment of Severe Hypovolemia or Hypovolemic Shock in Adults - UpToDateDokumen16 halamanTreatment of Severe Hypovolemia or Hypovolemic Shock in Adults - UpToDateparou haBelum ada peringkat
- Topical Hemostatic Agents in Surgery PDFDokumen10 halamanTopical Hemostatic Agents in Surgery PDFFernanda SouzaBelum ada peringkat
- ERAS For Colorectal SurgeryDokumen53 halamanERAS For Colorectal SurgeryJorge De VeraBelum ada peringkat
- ERAS Guidelines PDFDokumen8 halamanERAS Guidelines PDFWadezigBelum ada peringkat
- Levine 1990Dokumen6 halamanLevine 1990María Fernanda RíosBelum ada peringkat
- Dab Bous Eh 2011Dokumen3 halamanDab Bous Eh 2011María Fernanda RíosBelum ada peringkat
- Arrhythmogenic Right Ventricular Cardiomyopathy in Young Versus Adult Patients: Similarities and DifferencesDokumen10 halamanArrhythmogenic Right Ventricular Cardiomyopathy in Young Versus Adult Patients: Similarities and DifferencesMaría Fernanda RíosBelum ada peringkat
- Phlebitis and ThrombophlebitisDokumen27 halamanPhlebitis and ThrombophlebitisMaría Fernanda RíosBelum ada peringkat
- Phlebitis and ThrombophlebitisDokumen27 halamanPhlebitis and ThrombophlebitisMaría Fernanda Ríos100% (1)
- Kdigo 2021 BP GLDokumen92 halamanKdigo 2021 BP GLAndres Bermudez100% (1)
- 2009 - ACE Inhibition As A Cornerstone of Hypertension TreatmentDokumen111 halaman2009 - ACE Inhibition As A Cornerstone of Hypertension TreatmentHovhannes SahakyanBelum ada peringkat
- MRCP Part 1-Pharm GuestionsDokumen42 halamanMRCP Part 1-Pharm GuestionswyenyBelum ada peringkat
- The Renin Angiotensin Aldosterone System (RAAS)Dokumen22 halamanThe Renin Angiotensin Aldosterone System (RAAS)Chandra pranataBelum ada peringkat
- Renovascular HypertensionDokumen20 halamanRenovascular Hypertensionalul847474Belum ada peringkat
- Polypharmacy: in Older Adults at HomeDokumen12 halamanPolypharmacy: in Older Adults at HomenellyBelum ada peringkat
- NCLEX Medications For Nurses 1 PDFDokumen118 halamanNCLEX Medications For Nurses 1 PDF281175100% (4)
- Guidelines Made Simple 2017 HBPDokumen29 halamanGuidelines Made Simple 2017 HBPPianBelum ada peringkat
- Cytokine Storm in COVID-19Dokumen11 halamanCytokine Storm in COVID-19Feli FelBelum ada peringkat
- Preferred Beta-Blockers For The Treatment of Heart FailureDokumen7 halamanPreferred Beta-Blockers For The Treatment of Heart FailureAshutosh SinghBelum ada peringkat
- Review PharmacologyDokumen137 halamanReview PharmacologyGeronimo GonzalezBelum ada peringkat
- Drugs For Hypertension MIMSDokumen13 halamanDrugs For Hypertension MIMSriczen mae vilaBelum ada peringkat
- Chapter27-Assessment and Management of Patients With HypertensionDokumen31 halamanChapter27-Assessment and Management of Patients With HypertensionAhmed 123Belum ada peringkat
- NPTE CArdio NotesDokumen27 halamanNPTE CArdio NotesAubrey Vale SagunBelum ada peringkat
- Standards of Medical Care in Diabetes - 2022: 10. Cardiovascular Disease and Risk ManagementDokumen31 halamanStandards of Medical Care in Diabetes - 2022: 10. Cardiovascular Disease and Risk ManagementAdina SimionBelum ada peringkat
- Etiology and Diagnosis of Prerenal Disease and Acute Tubular Necrosis in Acute Kidney Injury in Adults - UpToDateDokumen22 halamanEtiology and Diagnosis of Prerenal Disease and Acute Tubular Necrosis in Acute Kidney Injury in Adults - UpToDatecuentaparatrabajosdelau10Belum ada peringkat
- Heart FailureDokumen10 halamanHeart FailureYudha GanesaBelum ada peringkat
- Obat UperioDokumen5 halamanObat UperioAnonymous Aa6VAStBelum ada peringkat
- Benazepril Synthesis - by DR ANTHONY CRASTODokumen46 halamanBenazepril Synthesis - by DR ANTHONY CRASTOAnthony Melvin Crasto Ph.DBelum ada peringkat
- Youngia JaponicaDokumen6 halamanYoungia JaponicarafrejuBelum ada peringkat
- ACLS Drugs (2010)Dokumen16 halamanACLS Drugs (2010)RN333100% (2)
- Cardiovascular and Metabolic Syndrome MOCK Test: Pharmacy PREPDokumen26 halamanCardiovascular and Metabolic Syndrome MOCK Test: Pharmacy PREPNOORBelum ada peringkat
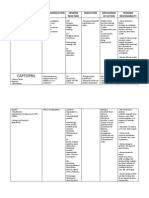
- Amlodipine Captopril MetronidazoleDokumen5 halamanAmlodipine Captopril Metronidazolekhrysty1506Belum ada peringkat
- Fast Five Quiz: Dangerous Drug CombinationsDokumen3 halamanFast Five Quiz: Dangerous Drug CombinationsHany ManikBelum ada peringkat
- Heart Failure: More... 58Dokumen4 halamanHeart Failure: More... 58pmBelum ada peringkat
- Pharmacological and Pharmaceutical Profile of Valsartan: A ReviewDokumen8 halamanPharmacological and Pharmaceutical Profile of Valsartan: A ReviewChikaFauzi100% (1)
- MEFTAL P Suspension PIDokumen10 halamanMEFTAL P Suspension PIpiyush patelBelum ada peringkat
- Medlifeline Drug of Choice 1st EditionDokumen39 halamanMedlifeline Drug of Choice 1st EditionAswin Krishna83% (6)
- PHARMACY MCQ Quiz 1Dokumen18 halamanPHARMACY MCQ Quiz 1Noah MrjBelum ada peringkat
- Ketorolac (Systemic) - Drug Information - UpToDateDokumen42 halamanKetorolac (Systemic) - Drug Information - UpToDateJosué Pablo Chicaiza AbadBelum ada peringkat