Anda mungkin juga menyukai
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (587)
- CHAPTER 27 - Heart Failure With A Preserved Ejection FractionDokumen15 halamanCHAPTER 27 - Heart Failure With A Preserved Ejection FractionReda SoBelum ada peringkat
- CHAPTER 61: Diabetes and The Cardiovascular System: Ma. Arnee V. Anico-Tondo, M.D., FPCP (CGH)Dokumen1 halamanCHAPTER 61: Diabetes and The Cardiovascular System: Ma. Arnee V. Anico-Tondo, M.D., FPCP (CGH)Reda SoBelum ada peringkat
- Chinese General Hospital and Medical Center Department of Medical Education and Research Research Ethics Review Board (Rerb)Dokumen11 halamanChinese General Hospital and Medical Center Department of Medical Education and Research Research Ethics Review Board (Rerb)Reda SoBelum ada peringkat
- CHAPTER 55 - Percutaneous Coronary InterventionDokumen1 halamanCHAPTER 55 - Percutaneous Coronary InterventionReda SoBelum ada peringkat
- Trials SummaryDokumen12 halamanTrials SummaryReda SoBelum ada peringkat
- Mitral Valve Disease QuizDokumen5 halamanMitral Valve Disease QuizReda SoBelum ada peringkat
- Braunwald Chapter KeypointersDokumen6 halamanBraunwald Chapter KeypointersReda SoBelum ada peringkat
- Chapter 32 - Genetic Cardiac ArrythmiasDokumen7 halamanChapter 32 - Genetic Cardiac ArrythmiasReda SoBelum ada peringkat
- CH 50 - Approach To Patient With Chest PainDokumen1 halamanCH 50 - Approach To Patient With Chest PainReda SoBelum ada peringkat
- Answer Key-Mitral ValveDokumen6 halamanAnswer Key-Mitral ValveReda SoBelum ada peringkat
- Ward Reflection PaperDokumen1 halamanWard Reflection PaperReda SoBelum ada peringkat
- Rapid Response and Cardiac Arrest TeamsDokumen11 halamanRapid Response and Cardiac Arrest TeamsReda SoBelum ada peringkat
- Name: - Year LevelDokumen6 halamanName: - Year LevelReda SoBelum ada peringkat
- Private Ward Admission Census 1Dokumen6 halamanPrivate Ward Admission Census 1Reda SoBelum ada peringkat
- Risk Factors in Developing Diabetic Foot Ulcers Among Patients in DM Foot Clinic at East Avenue Medical Center From January 2013 To January 2015Dokumen7 halamanRisk Factors in Developing Diabetic Foot Ulcers Among Patients in DM Foot Clinic at East Avenue Medical Center From January 2013 To January 2015Reda SoBelum ada peringkat
- Tilt Table Testing: Name Age/Sex APDokumen1 halamanTilt Table Testing: Name Age/Sex APReda SoBelum ada peringkat
- Vascular Conference: JUNE 2018 - MARCH 2019Dokumen2 halamanVascular Conference: JUNE 2018 - MARCH 2019Reda SoBelum ada peringkat
- Evidence-Based Approach to Heart Failure History and Physical ExamDokumen5 halamanEvidence-Based Approach to Heart Failure History and Physical ExamReda SoBelum ada peringkat
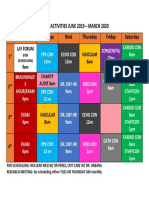
- Daily Activities 2019Dokumen1 halamanDaily Activities 2019Reda SoBelum ada peringkat
- Heart Institute Team Building April 2019Dokumen1 halamanHeart Institute Team Building April 2019Reda SoBelum ada peringkat
- Aortic ExamDokumen3 halamanAortic ExamReda SoBelum ada peringkat
- Coronary Blood Flow & Myocardial Ischemia Cardiology Fellows Exam July 23, 2018Dokumen3 halamanCoronary Blood Flow & Myocardial Ischemia Cardiology Fellows Exam July 23, 2018Reda SoBelum ada peringkat
- Coronary Blood Flow & Myocardial Ischemia Cardiology Fellows Exam July 23, 2018Dokumen3 halamanCoronary Blood Flow & Myocardial Ischemia Cardiology Fellows Exam July 23, 2018Reda SoBelum ada peringkat
- 2011 PadDokumen19 halaman2011 PadReda SoBelum ada peringkat
- Tilt Table Testing: Name Age/Sex APDokumen1 halamanTilt Table Testing: Name Age/Sex APReda SoBelum ada peringkat
- Cardiology census and patient detailsDokumen9 halamanCardiology census and patient detailsReda SoBelum ada peringkat
- Marijuana LegalizationDokumen5 halamanMarijuana LegalizationMatt ImpellusoBelum ada peringkat
- Case Protocol 3Dokumen2 halamanCase Protocol 3Reda SoBelum ada peringkat
- Case Protocol 3Dokumen5 halamanCase Protocol 3Reda SoBelum ada peringkat
- Computed Tomography Findings for 8 Cardiovascular PatientsDokumen1 halamanComputed Tomography Findings for 8 Cardiovascular PatientsReda SoBelum ada peringkat
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (399)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (73)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2219)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (265)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (119)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- Module 3 Cherry 110309Dokumen17 halamanModule 3 Cherry 110309Krislyn Dulay LagartoBelum ada peringkat
- Engaged Listening Worksheet 3 - 24Dokumen3 halamanEngaged Listening Worksheet 3 - 24John BennettBelum ada peringkat
- B767 WikipediaDokumen18 halamanB767 WikipediaxXxJaspiexXx100% (1)
- Das Aufkommen Eines Neuen Pseudoephedrinprodukts Zur Bekämpfung Des MethamphetaminmissbrauchsDokumen17 halamanDas Aufkommen Eines Neuen Pseudoephedrinprodukts Zur Bekämpfung Des Methamphetaminmissbrauchszossel ringoBelum ada peringkat
- AdmitCard 1688037Dokumen1 halamanAdmitCard 1688037P.Supreeth ReddyBelum ada peringkat
- Natural Science subject curriculumDokumen15 halamanNatural Science subject curriculum4porte3Belum ada peringkat
- Portland Cement: Material Safety Data Sheet (MSDS)Dokumen6 halamanPortland Cement: Material Safety Data Sheet (MSDS)eslam sokaBelum ada peringkat
- Susan Oyama The Ontogeny of Information Developmental Systems and Evolution Science and Cultural Theory 2000Dokumen297 halamanSusan Oyama The Ontogeny of Information Developmental Systems and Evolution Science and Cultural Theory 2000Marelin Hernández SaBelum ada peringkat
- Zeal Study 10th English Synonym Unit 1 - 7Dokumen24 halamanZeal Study 10th English Synonym Unit 1 - 7viaanenterprises2008Belum ada peringkat
- RITL 2007 (Full Text)Dokumen366 halamanRITL 2007 (Full Text)Institutul de Istorie și Teorie LiterarăBelum ada peringkat
- Mechanics of Solids Unit - I: Chadalawada Ramanamma Engineering CollegeDokumen1 halamanMechanics of Solids Unit - I: Chadalawada Ramanamma Engineering CollegeMITTA NARESH BABUBelum ada peringkat
- Uk GeographyDokumen9 halamanUk GeographyStainbok MihaiBelum ada peringkat
- I CEV20052 Structureofthe Food Service IndustryDokumen98 halamanI CEV20052 Structureofthe Food Service IndustryJowee TigasBelum ada peringkat
- Class 7 Summer Vacation PDFDokumen4 halamanClass 7 Summer Vacation PDFPrince RajBelum ada peringkat
- Introduction To Opengl/Glsl and WebglDokumen46 halamanIntroduction To Opengl/Glsl and Webglanon_828313787Belum ada peringkat
- Sikkim Public Works Liability of Government and Contractor Act 1983Dokumen11 halamanSikkim Public Works Liability of Government and Contractor Act 1983Latest Laws TeamBelum ada peringkat
- INDIA'S DEFENCE FORCESDokumen3 halamanINDIA'S DEFENCE FORCESJanardhan ChakliBelum ada peringkat
- January 2008 Ecobon Newsletter Hilton Head Island Audubon SocietyDokumen6 halamanJanuary 2008 Ecobon Newsletter Hilton Head Island Audubon SocietyHilton Head Island Audubon SocietyBelum ada peringkat
- Presentation 1Dokumen13 halamanPresentation 1lordonezBelum ada peringkat
- JSP - How To Edit Table of Data Displayed Using JSP When Clicked On Edit ButtonDokumen8 halamanJSP - How To Edit Table of Data Displayed Using JSP When Clicked On Edit Buttonrithuik1598Belum ada peringkat
- Homologation Form Number 5714 Group 1Dokumen28 halamanHomologation Form Number 5714 Group 1ImadBelum ada peringkat
- Arraignment PleaDokumen4 halamanArraignment PleaJoh SuhBelum ada peringkat
- The Ramayana and The Sacred Palm Trees of Sumeria, Mesopotamia, Assyria and PhoeniciaDokumen7 halamanThe Ramayana and The Sacred Palm Trees of Sumeria, Mesopotamia, Assyria and PhoeniciaNeeta RainaBelum ada peringkat
- Fitting A Logistic Curve To DataDokumen12 halamanFitting A Logistic Curve To DataXiaoyan ZouBelum ada peringkat
- Condicional Perfecto Continuo interrogativo guíaDokumen2 halamanCondicional Perfecto Continuo interrogativo guíaMaxi RamirezBelum ada peringkat
- How Should Management Be Structured British English StudentDokumen7 halamanHow Should Management Be Structured British English Studentr i s uBelum ada peringkat
- How To Write A Cover Letter For A Training ProgramDokumen4 halamanHow To Write A Cover Letter For A Training Programgyv0vipinem3100% (2)
- The Avengers (2012 Film)Dokumen4 halamanThe Avengers (2012 Film)Matthew SusetioBelum ada peringkat
- The Principle of Subsidiarity and Catholic Ecclesiology - ImplicatDokumen218 halamanThe Principle of Subsidiarity and Catholic Ecclesiology - ImplicatJonathanKiehlBelum ada peringkat
- EDUC 5240 - Creating Positive Classroom EnvironmentsDokumen5 halamanEDUC 5240 - Creating Positive Classroom EnvironmentsMay Phyo ThuBelum ada peringkat