Anda mungkin juga menyukai
- Emergency Ortho BCS 2017Dokumen80 halamanEmergency Ortho BCS 2017Priza RazunipBelum ada peringkat
- 9 Orthopaedic EmergenciesDokumen68 halaman9 Orthopaedic EmergenciesAndrew WdsmithBelum ada peringkat
- Femoral Shaft FracturesDokumen40 halamanFemoral Shaft FracturesOlasinde AnthonyBelum ada peringkat
- Damage ControlDokumen26 halamanDamage ControlSuad StambulieBelum ada peringkat
- Kevin Coates MD Femur and Tibia FracturesDokumen90 halamanKevin Coates MD Femur and Tibia FracturesIkhsan HidayatBelum ada peringkat
- Orthopaedic Emergencies AndreDokumen49 halamanOrthopaedic Emergencies AndreLusi MunawarohBelum ada peringkat
- G03 Evaluation and Treatment of Vascular Injury JTG Rev 2-3-10Dokumen37 halamanG03 Evaluation and Treatment of Vascular Injury JTG Rev 2-3-10kosmynin86Belum ada peringkat
- RTC Brachial Artery Injury and Upper Ext FasciotomyDokumen47 halamanRTC Brachial Artery Injury and Upper Ext FasciotomyAndini RezkiBelum ada peringkat
- Neck Trauma DR Hauwa Shitu 1Dokumen40 halamanNeck Trauma DR Hauwa Shitu 1Hauwa shitu.B100% (1)
- Fracture Dan Penanganan EmergencyDokumen52 halamanFracture Dan Penanganan Emergencyshindie lethulurBelum ada peringkat
- Initial Management in Musculoskeletal Trauma: Yoyos D. IsmiartoDokumen40 halamanInitial Management in Musculoskeletal Trauma: Yoyos D. IsmiartozaroziBelum ada peringkat
- Potentially Life-Threatening Extremity InjuriesDokumen41 halamanPotentially Life-Threatening Extremity Injuriesyuliaoksiyulanda ingeniopadangBelum ada peringkat
- Upper C Spine FractureDokumen54 halamanUpper C Spine FracturekiranbcBelum ada peringkat
- Fractures of The Lower LimbDokumen50 halamanFractures of The Lower LimbVishwajit Hegde100% (1)
- Handout Lat Elbow Pain PDFDokumen47 halamanHandout Lat Elbow Pain PDFgemichan26Belum ada peringkat
- Osteonecrosis of The Femoral Head: Kriangk BenjawongsathianDokumen65 halamanOsteonecrosis of The Femoral Head: Kriangk Benjawongsathianryc0% (1)
- 1 Materi Kuliah Spine, Dr. AzharuddinDokumen59 halaman1 Materi Kuliah Spine, Dr. AzharuddinfazliahBelum ada peringkat
- Trauma Spinal Wates Dr. WRDokumen68 halamanTrauma Spinal Wates Dr. WRLanlan LesmanaBelum ada peringkat
- Traumatic Proximal Femur Fractures: Molly E. Collins, Harvard Medical School Gillian Lieberman, MDDokumen31 halamanTraumatic Proximal Femur Fractures: Molly E. Collins, Harvard Medical School Gillian Lieberman, MDB-win IrawanBelum ada peringkat
- Fractures HFHDokumen74 halamanFractures HFHEmmanuel Papa AcquahBelum ada peringkat
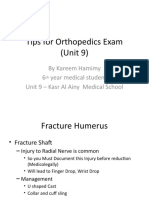
- Tips For Orthopedics ExamDokumen41 halamanTips For Orthopedics ExamKareem Waleed Ibrahim HamimyBelum ada peringkat
- Vascular EmergenciesDokumen81 halamanVascular EmergenciesJujhar BoparaiBelum ada peringkat
- Vascular InjuryDokumen26 halamanVascular InjuryEka NataBelum ada peringkat
- Cervical Spine FracturesDokumen58 halamanCervical Spine Fracturesamarsidin1Belum ada peringkat
- S6 Upper Cervical Spine TraumaDokumen82 halamanS6 Upper Cervical Spine TraumaDwi WicaksonoBelum ada peringkat
- Lower Limb Fracture..MeDokumen142 halamanLower Limb Fracture..MeWorku KifleBelum ada peringkat
- Wrist Pain: Pramono Ari Wibowo, MDDokumen46 halamanWrist Pain: Pramono Ari Wibowo, MDIwan Wonodihardjo100% (1)
- A Case Presentation On PolytraumaDokumen27 halamanA Case Presentation On PolytraumaFERDINAND ATSERBelum ada peringkat
- Fraktur PelvisDokumen39 halamanFraktur PelvisDzikrullah Akbar II100% (1)
- Fractures of Shoulder and Elbow EditedDokumen25 halamanFractures of Shoulder and Elbow EditedSurgicalgownBelum ada peringkat
- Avascular NecrosisDokumen51 halamanAvascular NecrosisBHARATH MOHANBelum ada peringkat
- Elbow Injuries: DR R B Kalia, Additional Professor Department of OrthopaedicsDokumen57 halamanElbow Injuries: DR R B Kalia, Additional Professor Department of OrthopaedicsHajar AlSaediBelum ada peringkat
- Femur Shaft FractureDokumen33 halamanFemur Shaft FractureAkash KoulBelum ada peringkat
- Lower Limb FracturesDokumen124 halamanLower Limb Fracturesmau tau100% (1)
- Hip FracturesDokumen74 halamanHip FracturesMina SamirBelum ada peringkat
- Intro To Orthopedic Emergencies - RCSI Orthopaedic Emergencies - MK1Dokumen65 halamanIntro To Orthopedic Emergencies - RCSI Orthopaedic Emergencies - MK1kylieverBelum ada peringkat
- Dislocations (PDFDrive)Dokumen111 halamanDislocations (PDFDrive)hemasary15Belum ada peringkat
- Compartment 20syndrome 20 - 20diagnostic 20difficulties 20and 20future 20developments 20 - 20flims 20lecture 20march2008 PDFDokumen44 halamanCompartment 20syndrome 20 - 20diagnostic 20difficulties 20and 20future 20developments 20 - 20flims 20lecture 20march2008 PDFHafiidz Fatich RosihanBelum ada peringkat
- Initial Trauma MusculoskeletalDokumen53 halamanInitial Trauma MusculoskeletalAnonymous wyBvCzkEBelum ada peringkat
- Trauma Musculoskeletal - Spine FKK UMJ1Dokumen92 halamanTrauma Musculoskeletal - Spine FKK UMJ1Hendra Hash AwoBelum ada peringkat
- Pathologicalfractures 170201065538Dokumen54 halamanPathologicalfractures 170201065538manan shroffBelum ada peringkat
- Extremity Trauma Board Review 2018Dokumen80 halamanExtremity Trauma Board Review 2018rigo montejoBelum ada peringkat
- אוסטיאומיאליטיס ושברים פתוחיםDokumen68 halamanאוסטיאומיאליטיס ושברים פתוחיםHussein SamhatBelum ada peringkat
- Pengayaan Koass Ortho - Update 5 VersionDokumen122 halamanPengayaan Koass Ortho - Update 5 Versionanon_967171484Belum ada peringkat
- Supracondylarfracture PDFDokumen40 halamanSupracondylarfracture PDFSurya AbigamikaBelum ada peringkat
- 220pm - Acute Aortic SyndromesDokumen17 halaman220pm - Acute Aortic SyndromesHARBENBelum ada peringkat
- Emergency in Musculoskeletal Trauma and Spinal Injuries - Dr. Asrafi Rizki Gatam SpOTDokumen42 halamanEmergency in Musculoskeletal Trauma and Spinal Injuries - Dr. Asrafi Rizki Gatam SpOTefancoolhand09Belum ada peringkat
- Fracture Tibia & Fibula-1Dokumen111 halamanFracture Tibia & Fibula-1Usaid SulaimanBelum ada peringkat
- Management of Fracture Acetabulum in Geriatric Age Group Saturday 12 15Dokumen44 halamanManagement of Fracture Acetabulum in Geriatric Age Group Saturday 12 15tarikeopsBelum ada peringkat
- Neck of Femur FractureDokumen36 halamanNeck of Femur FractureAbdulMushib100% (1)
- AAAJakarta2017 (DR - Hanafiah Haruna Rashid)Dokumen97 halamanAAAJakarta2017 (DR - Hanafiah Haruna Rashid)Intan Eklesiana NapitupuluBelum ada peringkat
- Immobilization and Transport On Patient FractureDokumen58 halamanImmobilization and Transport On Patient FractureDinaBelum ada peringkat
- Cervical Spine InjuriesDokumen50 halamanCervical Spine InjuriesgamalramadiBelum ada peringkat
- Scfe PDFDokumen39 halamanScfe PDFMuhammad Tabish SaleemBelum ada peringkat
- Fractures and DislocationsDokumen41 halamanFractures and DislocationsRic Raphael PiodenaBelum ada peringkat
- Polytrauma, ABC of Trauma & Its ManagementDokumen33 halamanPolytrauma, ABC of Trauma & Its ManagementMongolian MutuBelum ada peringkat
- Sports Medicine (Elbow and Spinal Injuries) InjuriesDokumen73 halamanSports Medicine (Elbow and Spinal Injuries) InjuriesnhfbyqvgwhBelum ada peringkat
- Departement of Orthopaedic and TraumatologyDokumen89 halamanDepartement of Orthopaedic and TraumatologyMukhizalBelum ada peringkat
- Pelvic TraumaDokumen20 halamanPelvic Traumachehak.kumar2000Belum ada peringkat
- Hotel and Room Facilities (Part3g1)Dokumen14 halamanHotel and Room Facilities (Part3g1)Mary Joy CelamorBelum ada peringkat
- Characterization of Glaucoma Medication Adherence in Kaiser Permanente Southern CaliforniaDokumen5 halamanCharacterization of Glaucoma Medication Adherence in Kaiser Permanente Southern CaliforniaAu ZouBelum ada peringkat
- Ve 101 - MSDSDokumen13 halamanVe 101 - MSDSEngineering MP CikupaBelum ada peringkat
- Kertas Trial English Perlis K1 Set B 2021Dokumen13 halamanKertas Trial English Perlis K1 Set B 2021darwish erfanBelum ada peringkat
- (PDF) Transformational Leadership, Self Efficacy, Group Cohesiveness, Commitment, and PerformanceDokumen11 halaman(PDF) Transformational Leadership, Self Efficacy, Group Cohesiveness, Commitment, and Performancesyarif suksesBelum ada peringkat
- Suggestive Questions of Isc 2023 BiologyDokumen12 halamanSuggestive Questions of Isc 2023 Biologyjahnvipatel2004Belum ada peringkat
- Garden Trust Launches A CompetitionDokumen3 halamanGarden Trust Launches A CompetitionCami GrossiBelum ada peringkat
- Weekly Report 13 - 19 2017Dokumen11 halamanWeekly Report 13 - 19 2017Sitha MahendrataBelum ada peringkat
- Jurnal AsiDokumen6 halamanJurnal AsiAmeliarBelum ada peringkat
- Tissue Salts CombinationsDokumen12 halamanTissue Salts Combinationsherbacija9213100% (2)
- Hemorrhagic StrokeDokumen2 halamanHemorrhagic StrokeMuhammad Anwar AnsoriBelum ada peringkat
- 2 - GFSI Overview One Pager 1Dokumen2 halaman2 - GFSI Overview One Pager 1Diego GordoBelum ada peringkat
- The Role of Physiotherapy in The Prevention and Treatment of OsteoporosisDokumen16 halamanThe Role of Physiotherapy in The Prevention and Treatment of OsteoporosisDiego Cruces OrdoñezBelum ada peringkat
- Kooner - Google SearchDokumen2 halamanKooner - Google Searchmiir ikbalBelum ada peringkat
- Timbul Sakulasi Atau DivertikelDokumen2 halamanTimbul Sakulasi Atau DivertikelRendi PotlotBelum ada peringkat
- TRAINING WORKSHOP FOR TRADITIONAL HERBAL MEDICAL PRACTIONERS Ode OmuDokumen2 halamanTRAINING WORKSHOP FOR TRADITIONAL HERBAL MEDICAL PRACTIONERS Ode OmuOlatunji Adebisi TundeBelum ada peringkat
- Lemon and Baking Soda Miraculous CombinationDokumen14 halamanLemon and Baking Soda Miraculous CombinationMoses Apeabu100% (4)
- BS 5000-17Dokumen8 halamanBS 5000-17stuart3962Belum ada peringkat
- HSE Manager & Supervisor CV - Niranjan 30-04-2021Dokumen4 halamanHSE Manager & Supervisor CV - Niranjan 30-04-2021NiraBelum ada peringkat
- Stepping Inside The Mind: Da Vinci and The World of The Human BrainDokumen5 halamanStepping Inside The Mind: Da Vinci and The World of The Human BrainbarakuparaBelum ada peringkat
- Cognitive-Behavioral Therapy: Instructor's ManualDokumen68 halamanCognitive-Behavioral Therapy: Instructor's ManualzingpalmsBelum ada peringkat
- Directorate of Medical Education and Research, Haryana: Telephone:0172-2584533/2584633, SCO No.-7 Sector-16, PanchkulaDokumen1 halamanDirectorate of Medical Education and Research, Haryana: Telephone:0172-2584533/2584633, SCO No.-7 Sector-16, PanchkulaQwertyBelum ada peringkat
- Pepper PDFDokumen52 halamanPepper PDFMarie GregorioBelum ada peringkat
- Manual de Usuario Panasonic Toughbook CF-31 (44 Páginas)Dokumen3 halamanManual de Usuario Panasonic Toughbook CF-31 (44 Páginas)Angel VelascoBelum ada peringkat
- Subdermal HematomaDokumen2 halamanSubdermal HematomaDristi KhanalBelum ada peringkat
- The Health Care Delivery System in The PhilippinesDokumen15 halamanThe Health Care Delivery System in The PhilippinesXandra Basnillo100% (2)
- Therapeutic Aquatic Exercise in The Treatment of Low Back Pain - A Systematic ReviewDokumen12 halamanTherapeutic Aquatic Exercise in The Treatment of Low Back Pain - A Systematic ReviewGleiiseTalitaBelum ada peringkat
- The Statistical Abstract of The United States 2009Dokumen996 halamanThe Statistical Abstract of The United States 2009Aaron MonkBelum ada peringkat
- 1st Decision - G.R. No. 217872Dokumen11 halaman1st Decision - G.R. No. 217872MerBelum ada peringkat
- Unit 14. Nursing DocumentationDokumen6 halamanUnit 14. Nursing Documentationputridelia yalanavilaBelum ada peringkat