Anda mungkin juga menyukai
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- Complementary Therapies in Medicine: Fulvio Dal Farra, Roberta Giulia Risio, Luca Vismara, Andrea BergnaDokumen13 halamanComplementary Therapies in Medicine: Fulvio Dal Farra, Roberta Giulia Risio, Luca Vismara, Andrea BergnaOliver JimenezBelum ada peringkat
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (399)
- Sicilienne For Cello PianoDokumen2 halamanSicilienne For Cello PianoProfa Luciana GuimarãesBelum ada peringkat
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Complementary Therapies in MedicineDokumen7 halamanComplementary Therapies in MedicineProfa Luciana GuimarãesBelum ada peringkat
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (894)
- Barcelona Scoliosis Physical Therapy School - BSPTDokumen1 halamanBarcelona Scoliosis Physical Therapy School - BSPTProfa Luciana GuimarãesBelum ada peringkat
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Effects of Cervical High Velocity Low AmDokumen9 halamanEffects of Cervical High Velocity Low AmProfa Luciana GuimarãesBelum ada peringkat
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- Neurophysiological Effects of Spinal Manipulation: Joel G. Pickar, DC, PHDDokumen15 halamanNeurophysiological Effects of Spinal Manipulation: Joel G. Pickar, DC, PHDAnonymous ZmRV6WqBelum ada peringkat
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- Changes in Pain Sensitivity Following SPDokumen16 halamanChanges in Pain Sensitivity Following SPProfa Luciana GuimarãesBelum ada peringkat
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Sicilienne: PianoDokumen1 halamanSicilienne: PianoProfa Luciana GuimarãesBelum ada peringkat
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (587)
- Manipulative Therapy For Lower ExtremityDokumen40 halamanManipulative Therapy For Lower ExtremityProfa Luciana GuimarãesBelum ada peringkat
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (265)
- HeimDokumen99 halamanHeimProfa Luciana GuimarãesBelum ada peringkat
- Paulino 2018 Prevalencia de Sinais e Sintomas deDokumen14 halamanPaulino 2018 Prevalencia de Sinais e Sintomas deProfa Luciana GuimarãesBelum ada peringkat
- Infertility and Manual Therapy TreatmentDokumen14 halamanInfertility and Manual Therapy TreatmentririnBelum ada peringkat
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- Liberati2009 PDFDokumen34 halamanLiberati2009 PDFMiranti Dea DoraBelum ada peringkat
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (73)
- Article About Joint CrackingDokumen5 halamanArticle About Joint CrackingJeffsynthBelum ada peringkat
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- 3 - Cosmin 2010Dokumen8 halaman3 - Cosmin 2010Profa Luciana GuimarãesBelum ada peringkat
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Terwee2007 PDFDokumen9 halamanTerwee2007 PDFazeemBelum ada peringkat
- Guidelines For The Process of Cross-Cultural AdaptationDokumen6 halamanGuidelines For The Process of Cross-Cultural Adaptationas2696891Belum ada peringkat
- Guidelines For The Process of Cross-Cultural AdaptationDokumen6 halamanGuidelines For The Process of Cross-Cultural Adaptationas2696891Belum ada peringkat
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- 5 - Protocol of The COSMIN Study 2006Dokumen7 halaman5 - Protocol of The COSMIN Study 2006Profa Luciana GuimarãesBelum ada peringkat
- Scholtes2011 PDFDokumen5 halamanScholtes2011 PDFThayla Amorim SantinoBelum ada peringkat
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- Plicae - Where Do They Come From and When Are They RelevantDokumen22 halamanPlicae - Where Do They Come From and When Are They RelevantProfa Luciana GuimarãesBelum ada peringkat
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2219)
- Osteopathic Manipulative Treatment in Pediatric, 2016Dokumen5 halamanOsteopathic Manipulative Treatment in Pediatric, 2016Profa Luciana GuimarãesBelum ada peringkat
- Panchmatia Et Al 2015 - Lido PDFDokumen8 halamanPanchmatia Et Al 2015 - Lido PDFProfa Luciana GuimarãesBelum ada peringkat
- 2008, Effectiveness of Osteopathy in The Cranial Field and Myofascial ReleaseDokumen12 halaman2008, Effectiveness of Osteopathy in The Cranial Field and Myofascial ReleaseProfa Luciana GuimarãesBelum ada peringkat
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- Panchmatia Et Al 2015 - Lido PDFDokumen8 halamanPanchmatia Et Al 2015 - Lido PDFProfa Luciana GuimarãesBelum ada peringkat
- 2013, Effectiveness of Dry NeedlingDokumen15 halaman2013, Effectiveness of Dry NeedlingProfa Luciana GuimarãesBelum ada peringkat
- 2012 Perez Sneed Eland Evidence-Based Osteopathic Manipulative Treatment For Coomon ConditionsDokumen5 halaman2012 Perez Sneed Eland Evidence-Based Osteopathic Manipulative Treatment For Coomon ConditionsProfa Luciana GuimarãesBelum ada peringkat
- Adolescent Scoliosis Classification and PDFDokumen12 halamanAdolescent Scoliosis Classification and PDFProfa Luciana GuimarãesBelum ada peringkat
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (119)
- 2006 Bevilaqua Grossi Et Al Anamnestic Index Severity and Signs and SymptomsDokumen9 halaman2006 Bevilaqua Grossi Et Al Anamnestic Index Severity and Signs and SymptomsProfa Luciana GuimarãesBelum ada peringkat
- Jamilex Polonia PLC ProjectDokumen8 halamanJamilex Polonia PLC Projectapi-491267452Belum ada peringkat
- How Can You Cultivate A Creative Self? The Five-Part Prescription From THE CREATIVITY CUREDokumen33 halamanHow Can You Cultivate A Creative Self? The Five-Part Prescription From THE CREATIVITY CURESimon and Schuster75% (8)
- Cognitive Development in Infancy Refers To The Development in The Way A Baby ThinkDokumen16 halamanCognitive Development in Infancy Refers To The Development in The Way A Baby ThinkKirsten Anne BarbaBelum ada peringkat
- Unit 9b Listening p143 Audio ScriptDokumen1 halamanUnit 9b Listening p143 Audio ScriptふんBelum ada peringkat
- Gestural TheoryDokumen9 halamanGestural TheoryCaroline BilousBelum ada peringkat
- Scared YouthDokumen2 halamanScared Youthnarcis2009Belum ada peringkat
- Cyprus International UniversityDokumen8 halamanCyprus International UniversitykhaleelthalegendBelum ada peringkat
- Observing with the Senses for Magical SkillDokumen1 halamanObserving with the Senses for Magical SkillIon VladBelum ada peringkat
- Holistic Nursing Care ModelDokumen14 halamanHolistic Nursing Care ModelmujionoBelum ada peringkat
- A 5Dokumen6 halamanA 5Winnie AriolaBelum ada peringkat
- PYC1501 Basic Psychology Cognition - ThinkingDokumen4 halamanPYC1501 Basic Psychology Cognition - Thinkingektha_nankoomar91100% (3)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- Applications of Psychological Test in Education and CounsellingDokumen22 halamanApplications of Psychological Test in Education and CounsellingShweta Poonam100% (1)
- Response of The Brain To EnrichmentDokumen66 halamanResponse of The Brain To EnrichmentCandi Kamira BalladaresBelum ada peringkat
- A Review of Intrinsic and Extrinsic Motivations of ESL LearnersDokumen9 halamanA Review of Intrinsic and Extrinsic Motivations of ESL LearnersCynthia MéndezBelum ada peringkat
- Psychiatric Emergencies (Part I) : Psychiatric Disorders Causing Organic SymptomsDokumen22 halamanPsychiatric Emergencies (Part I) : Psychiatric Disorders Causing Organic Symptomsgoldenday_hdpBelum ada peringkat
- Dahraan Mental Hospital Marka Mental Health CareDokumen8 halamanDahraan Mental Hospital Marka Mental Health CareJossephBelum ada peringkat
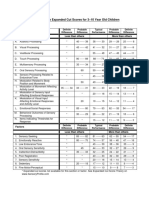
- Sensory Profile Expanded Cut Scores For 3-10 Year Old ChildrenDokumen1 halamanSensory Profile Expanded Cut Scores For 3-10 Year Old ChildrenAyra MagpiliBelum ada peringkat
- Leadership Assessment From MindtoolsDokumen3 halamanLeadership Assessment From MindtoolsigoeneezmBelum ada peringkat
- How Your Brain WorksDokumen7 halamanHow Your Brain WorksMRITZBelum ada peringkat
- Cataract NCPDokumen1 halamanCataract NCPMhegz Halcon75% (8)
- Theory of Personality Chapter-1Dokumen13 halamanTheory of Personality Chapter-1chat gaza0% (1)
- Clinical Psychologist Challenges After UniversityDokumen21 halamanClinical Psychologist Challenges After UniversityAya Nabil El ByalyBelum ada peringkat
- FBM PDFDokumen1 halamanFBM PDFJeremiahgibsonBelum ada peringkat
- IB Psychology EE ExemplarDokumen28 halamanIB Psychology EE Exemplaryorma uamBelum ada peringkat
- Backpropagation explainedDokumen14 halamanBackpropagation explainedRamyasree BadeBelum ada peringkat
- Educator Guide: Challenger DeepDokumen3 halamanEducator Guide: Challenger DeepEpicReads100% (2)
- Hiperakusis 2015Dokumen20 halamanHiperakusis 2015Abdur ShamilBelum ada peringkat
- Questionnaire For Thesis Boarding and Non-BoardingDokumen3 halamanQuestionnaire For Thesis Boarding and Non-BoardingNeguill AmoncioBelum ada peringkat
- Language and The Human BrainDokumen2 halamanLanguage and The Human BrainDharshan GunaBelum ada peringkat
- The Age of Magical Overthinking: Notes on Modern IrrationalityDari EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityPenilaian: 4 dari 5 bintang4/5 (13)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsDari EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsBelum ada peringkat
- Why We Die: The New Science of Aging and the Quest for ImmortalityDari EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityPenilaian: 3.5 dari 5 bintang3.5/5 (2)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsDari EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsPenilaian: 3.5 dari 5 bintang3.5/5 (3)