Anda mungkin juga menyukai
- 14 Local Anesthesia 2006 BDokumen18 halaman14 Local Anesthesia 2006 BMansoor AhmadBelum ada peringkat
- Basics of Local Anesthesia AdministrationDokumen18 halamanBasics of Local Anesthesia Administrationrutikanaga williamBelum ada peringkat
- LOCAL ANESTHETICS MECHANISMDokumen30 halamanLOCAL ANESTHETICS MECHANISMCorry QyBelum ada peringkat
- Local Anesthetic AgentsDokumen42 halamanLocal Anesthetic AgentsyohannesBelum ada peringkat
- #Local Anesthetic DrugsDokumen26 halaman#Local Anesthetic DrugsTripti Padalia100% (1)
- Local AnestheticsDokumen93 halamanLocal Anestheticsgeetika100% (1)
- Drugs For Anesthesia, Muscle RelaxationDokumen265 halamanDrugs For Anesthesia, Muscle RelaxationTamara Heradwita GSBelum ada peringkat
- LA Pharma and ArmamentariumDokumen59 halamanLA Pharma and ArmamentariumPakistan Dental SocietyBelum ada peringkat
- Local AnestheticsDokumen44 halamanLocal Anestheticsblack pink in ur area 21Belum ada peringkat
- Local AnesthesiaDokumen9 halamanLocal AnesthesiaSherry RamirezBelum ada peringkat
- Local AnaestheticsDokumen27 halamanLocal AnaestheticsRawand Ra'ed D.AlshawabkehBelum ada peringkat
- Wa0020.Dokumen32 halamanWa0020.Safura IjazBelum ada peringkat
- Anestesi LokalDokumen62 halamanAnestesi LokalNiaBelum ada peringkat
- L.A in Dentistry 1Dokumen13 halamanL.A in Dentistry 1CHUKWUDI HENRYBelum ada peringkat
- Local Anesthetics 2019-2020 2nd YrDokumen54 halamanLocal Anesthetics 2019-2020 2nd YrJolaine ValloBelum ada peringkat
- Anesthetic SubstancesDokumen12 halamanAnesthetic SubstancesNewPhoneWhoDisBelum ada peringkat
- 2 Pharmacology of LA 2 1Dokumen50 halaman2 Pharmacology of LA 2 1محمد ربيعيBelum ada peringkat
- Local Analgesia in AnimalsDokumen88 halamanLocal Analgesia in AnimalsBibek SutradharBelum ada peringkat
- Local Anesthesia ToxicityDokumen5 halamanLocal Anesthesia ToxicityvelangniBelum ada peringkat
- Unit 1 (B) - DibucaineDokumen4 halamanUnit 1 (B) - DibucaineDr_GSBelum ada peringkat
- Local Anaesthesia: Department of Anaesthesia University of Cape TownDokumen0 halamanLocal Anaesthesia: Department of Anaesthesia University of Cape TownjuniorebindaBelum ada peringkat
- Pre Anesthetics Local AnestheticsDokumen45 halamanPre Anesthetics Local AnestheticsDR AbidBelum ada peringkat
- L.A 2015Dokumen32 halamanL.A 2015Eisha BatoolBelum ada peringkat
- Pharmacology of Local AnestheticsDokumen25 halamanPharmacology of Local AnestheticsMonica RaafatBelum ada peringkat
- Local AnaestheticsDokumen19 halamanLocal AnaestheticsMohamed Abdullahi OsmanBelum ada peringkat
- Educational Material RA Handbook FinalDokumen58 halamanEducational Material RA Handbook Finalอี๊ด โสภิต Pizzy100% (5)
- Locac AnaestheticsDokumen31 halamanLocac AnaestheticsfadhiliBelum ada peringkat
- Review Article: New Formulations of Local Anaesthetics-Part IDokumen12 halamanReview Article: New Formulations of Local Anaesthetics-Part IJavier Farias VeraBelum ada peringkat
- Arp2012 546409Dokumen11 halamanArp2012 546409Agustina ZairidaBelum ada peringkat
- Local Anesthesia Review: Mechanisms, Uses, and SafetyDokumen12 halamanLocal Anesthesia Review: Mechanisms, Uses, and SafetyG.S. Imanto UchihaBelum ada peringkat
- PRINCIPLES OF SURGICAL ANESTHESIADokumen46 halamanPRINCIPLES OF SURGICAL ANESTHESIASisay FentaBelum ada peringkat
- Local AnaestheticsDokumen31 halamanLocal AnaestheticsNodi NodiBelum ada peringkat
- Local Anaesthesia Techniques and Complications in DentistryDokumen149 halamanLocal Anaesthesia Techniques and Complications in DentistryARNOLD OBIBelum ada peringkat
- 12.1.4 - Local Anesthetics (2009 - Feb2013)Dokumen42 halaman12.1.4 - Local Anesthetics (2009 - Feb2013)Gabrielle NnomoBelum ada peringkat
- Pediatric Dental Procedures, Anesthesia & Drug DosageDokumen75 halamanPediatric Dental Procedures, Anesthesia & Drug DosageElamaaraeen MadhvanBelum ada peringkat
- LECTURADokumen13 halamanLECTURAKaren VillegasBelum ada peringkat
- Local Anesthetics: Richard D. Minshall, PHD Tobias Piegeler, MDDokumen40 halamanLocal Anesthetics: Richard D. Minshall, PHD Tobias Piegeler, MDJohnBedaLatawanMalecdanBelum ada peringkat
- Chapt 3Dokumen5 halamanChapt 3arifjo7999Belum ada peringkat
- Local Anaesthetics: For BdsDokumen47 halamanLocal Anaesthetics: For BdsDr.U.P.Rathnakar.MD.DIH.PGDHMBelum ada peringkat
- Local Anaesthetics Sum SheetDokumen2 halamanLocal Anaesthetics Sum Sheetnzq7m6ph4dBelum ada peringkat
- Local Anesthesia Exam TipsDokumen9 halamanLocal Anesthesia Exam TipsshadapaaakBelum ada peringkat
- Veterinary Anesthesia (Autosaved)Dokumen57 halamanVeterinary Anesthesia (Autosaved)Zeinab Ali Shokor100% (2)
- 6 Regional AnaesthesiaDokumen12 halaman6 Regional AnaesthesiasaniaaBelum ada peringkat
- PCOL211 Introduction To PharmacologyDokumen6 halamanPCOL211 Introduction To PharmacologyLady RabadonBelum ada peringkat
- Pha051 Las#10 RationaleDokumen39 halamanPha051 Las#10 RationaleMonique EamiguelBelum ada peringkat
- Local Anesthetics SabinDokumen69 halamanLocal Anesthetics Sabinsabin7000Belum ada peringkat
- Local Dan PNB in EDDokumen26 halamanLocal Dan PNB in EDabdulkadirmunsyBelum ada peringkat
- Local Anesthesia in Pediatric DentistryDokumen70 halamanLocal Anesthesia in Pediatric DentistryNicky Romeo100% (1)
- LocalanestheticsDokumen51 halamanLocalanestheticskingkb4uBelum ada peringkat
- Pharmacology of Local Anesthetics IDokumen93 halamanPharmacology of Local Anesthetics IAlshaimaa AhmedBelum ada peringkat
- LOCAL ANAESTHETICS - Presentation RecordedDokumen22 halamanLOCAL ANAESTHETICS - Presentation RecordedTatenda SibandaBelum ada peringkat
- Local Anesthetic Drugs: DR - Safa Bakr Karim M.B.Ch.B.,H.D.A.,F.I.B.M.S. (Anesth.)Dokumen45 halamanLocal Anesthetic Drugs: DR - Safa Bakr Karim M.B.Ch.B.,H.D.A.,F.I.B.M.S. (Anesth.)venus jalalBelum ada peringkat
- Chapt 3Dokumen5 halamanChapt 3Javier Farias VeraBelum ada peringkat
- Local Anesthetic AgentsDokumen32 halamanLocal Anesthetic AgentsAbby BorabienBelum ada peringkat
- Pharmacology Intravenous Anesthetic Agents DissociativesDokumen13 halamanPharmacology Intravenous Anesthetic Agents DissociativesInnocent MwilaBelum ada peringkat
- Local Anaesthetics ExplainedDokumen24 halamanLocal Anaesthetics ExplainedMalueth AnguiBelum ada peringkat
- Local anesthesia in large animalsDokumen53 halamanLocal anesthesia in large animalsNot SayingBelum ada peringkat
- Local Anesthetic Pharmacology LecDokumen16 halamanLocal Anesthetic Pharmacology LecFazira EkmaBelum ada peringkat
- High-Resolution Electrophoresis and Immunofixation: Techniques and InterpretationDari EverandHigh-Resolution Electrophoresis and Immunofixation: Techniques and InterpretationPenilaian: 5 dari 5 bintang5/5 (1)
- ProductsDokumen3 halamanProductsMirza HassanBelum ada peringkat
- New Microsoft Word DocumentDokumen9 halamanNew Microsoft Word DocumentMirza HassanBelum ada peringkat
- Qaid e Taqdeer by Ayesha LiaqatDokumen201 halamanQaid e Taqdeer by Ayesha LiaqatMirza HassanBelum ada peringkat
- Vaccination Schedule of Farm AnimalsDokumen2 halamanVaccination Schedule of Farm AnimalsMirza HassanBelum ada peringkat
- New Microsoft Word DocumentDokumen9 halamanNew Microsoft Word DocumentMirza HassanBelum ada peringkat
- New Microsoft Word DocumentDokumen9 halamanNew Microsoft Word DocumentMirza HassanBelum ada peringkat
- Pharma Product List with Generic and Brand NamesDokumen12 halamanPharma Product List with Generic and Brand NamesMirza HassanBelum ada peringkat
- ProductsDokumen3 halamanProductsMirza HassanBelum ada peringkat
- Observations On Cattle Dairy Breeds in Pakistan Need To Curb Unseen Economic Losses Through Control of Mastitis and Endemic DiseasesDokumen18 halamanObservations On Cattle Dairy Breeds in Pakistan Need To Curb Unseen Economic Losses Through Control of Mastitis and Endemic DiseasesMirza HassanBelum ada peringkat
- Data Analysis of Multiple VariablesDokumen10 halamanData Analysis of Multiple VariablesMirza HassanBelum ada peringkat
- Ego and SuperegoDokumen14 halamanEgo and SuperegoMirza HassanBelum ada peringkat
- 4 Applied AnthropologyDokumen20 halaman4 Applied AnthropologyMirza HassanBelum ada peringkat
- Brain LaraDokumen6 halamanBrain LaraMirza HassanBelum ada peringkat
- Product Purchase ReportDokumen3 halamanProduct Purchase ReportMirza HassanBelum ada peringkat
- Central Processing Unit.: 1. CPU Stands ForDokumen1 halamanCentral Processing Unit.: 1. CPU Stands ForMirza HassanBelum ada peringkat
- Anti-Convulsants or Anti-Epileptic Drugs: Seizure DisordersDokumen38 halamanAnti-Convulsants or Anti-Epileptic Drugs: Seizure DisordersMirza HassanBelum ada peringkat
- IVM (In Vitro Maturation) WWWWWWWWWDokumen17 halamanIVM (In Vitro Maturation) WWWWWWWWWMirza HassanBelum ada peringkat
- Pharmacology of Anti-Inflammatory Drugs: Corticosteroids and NSAIDsDokumen3 halamanPharmacology of Anti-Inflammatory Drugs: Corticosteroids and NSAIDsMirza HassanBelum ada peringkat
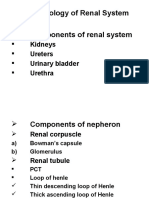
- Pharmacology of Renal System Components of Renal System: Kidneys Ureters Urinary Bladder UrethraDokumen30 halamanPharmacology of Renal System Components of Renal System: Kidneys Ureters Urinary Bladder UrethraMirza HassanBelum ada peringkat
- Anthelmintic SDokumen33 halamanAnthelmintic SMirza HassanBelum ada peringkat
- Auricular AbscessDokumen20 halamanAuricular AbscessMirza HassanBelum ada peringkat
- Pricing Information of Vet Products..HarisDokumen17 halamanPricing Information of Vet Products..HarisMirza Hassan75% (4)
- SDokumen2 halamanSMirza HassanBelum ada peringkat
- Anasthetic SDokumen26 halamanAnasthetic SMirza HassanBelum ada peringkat
- Analgesics NewDokumen21 halamanAnalgesics NewMirza HassanBelum ada peringkat
- IVM (In Vitro Maturation) WWWWWWWWWDokumen17 halamanIVM (In Vitro Maturation) WWWWWWWWWMirza HassanBelum ada peringkat
- RadiologyDokumen19 halamanRadiologyMirza HassanBelum ada peringkat
- Cell Cycle and MitosisDokumen21 halamanCell Cycle and MitosisMirza HassanBelum ada peringkat
- Pricing Information of Vet Products..HarisDokumen17 halamanPricing Information of Vet Products..HarisMirza Hassan75% (4)
- Ob2rle Sas 20Dokumen10 halamanOb2rle Sas 20Aira Mae R. AndradaBelum ada peringkat
- All Topics - 2008-2011 - ADokumen37 halamanAll Topics - 2008-2011 - ADebangshu KumarBelum ada peringkat
- Use of Local Anesthesia For Pediatric DentalDokumen6 halamanUse of Local Anesthesia For Pediatric DentalمعتزباللهBelum ada peringkat
- Journal AnesthesiaDokumen9 halamanJournal AnesthesiaoliviafabitaBelum ada peringkat
- Local Anaesthesia in EndodonticsDokumen76 halamanLocal Anaesthesia in Endodonticssaurav kumar duttaBelum ada peringkat
- Caudal anesthesia guideDokumen27 halamanCaudal anesthesia guidepradeep daniel100% (1)
- Obat-Obat AnestesiDokumen68 halamanObat-Obat AnestesiNia HndynBelum ada peringkat
- Basic Suturing TechniqueDokumen41 halamanBasic Suturing TechniqueAisyah01 Kayla100% (1)
- DrugsDokumen81 halamanDrugsrevathidadam55555100% (1)
- Malamed S HandBook of Local Anasthesia 6ed PDFDokumen428 halamanMalamed S HandBook of Local Anasthesia 6ed PDFCleverys Qisthi Phienna94% (16)
- Ropivacaine HCL (Naropine)Dokumen23 halamanRopivacaine HCL (Naropine)Dea NandaBelum ada peringkat
- Surgical SkillsDokumen47 halamanSurgical SkillsSamah SuhailBelum ada peringkat
- 2006, Vol.19, Issues 2, Ocular Anesthesia PDFDokumen156 halaman2006, Vol.19, Issues 2, Ocular Anesthesia PDFalvyandaniBelum ada peringkat
- Abdominal Pain Causes and Exam FindingsDokumen171 halamanAbdominal Pain Causes and Exam FindingsNaveen ChandanBelum ada peringkat
- Medschool AnestheticsDokumen4 halamanMedschool AnestheticsJustin HulinBelum ada peringkat
- Santi-Total Thesis Title - Upto June 2016Dokumen33 halamanSanti-Total Thesis Title - Upto June 2016Tulip JBelum ada peringkat
- Anaesthesia in Endodontics: Eirini Fragouli, Georgios Dechouniotis, Maria GeorgopoulouDokumen14 halamanAnaesthesia in Endodontics: Eirini Fragouli, Georgios Dechouniotis, Maria GeorgopoulouShriya ShahuBelum ada peringkat
- 2019 Paulo Steagall Et All - Lidocaina IntraperitonealDokumen5 halaman2019 Paulo Steagall Et All - Lidocaina IntraperitonealHarrisonBelum ada peringkat
- 2018 PG Dissertation TopicsDokumen118 halaman2018 PG Dissertation Topicsparas yadavBelum ada peringkat
- Local and General AnestheticsDokumen9 halamanLocal and General AnestheticsRon Olegario100% (1)
- Thesis Topics in AnaesthesiaDokumen1 halamanThesis Topics in AnaesthesiaShlok Tandon100% (1)
- Incision and Drainage of Scrotal AbscessDokumen31 halamanIncision and Drainage of Scrotal AbscessRm LavariasBelum ada peringkat
- Analgesia and Anesthesia in Labor and DeliveryDokumen52 halamanAnalgesia and Anesthesia in Labor and DeliveryAnggri Septyan100% (1)
- To Evaluate The Efficacy of Ultrasonography Guided Pectoral Nerve Block For Postoperative Analgesia in Breast SurgeriesDokumen4 halamanTo Evaluate The Efficacy of Ultrasonography Guided Pectoral Nerve Block For Postoperative Analgesia in Breast SurgeriesInternational Journal of Innovative Science and Research TechnologyBelum ada peringkat
- AnaestheticsDokumen33 halamanAnaestheticsAsif Ali LashariBelum ada peringkat
- Additive To Additive To Hyperbaric Bupivacaine in Spinal AnesthesiaDokumen6 halamanAdditive To Additive To Hyperbaric Bupivacaine in Spinal AnesthesiazzzzBelum ada peringkat
- Rle NotesDokumen7 halamanRle NotesLorens Troy SoltisBelum ada peringkat
- LESSON PLAN - AnagicisDokumen22 halamanLESSON PLAN - AnagicisrenuBelum ada peringkat
- Method of Vital Extirpation PDFDokumen23 halamanMethod of Vital Extirpation PDFShany SchwarzwaldBelum ada peringkat
- Introduction to Local AnestheticsDokumen24 halamanIntroduction to Local AnestheticsBismah SaeedBelum ada peringkat