Anda mungkin juga menyukai
- NutritionDokumen51 halamanNutritionEd CBelum ada peringkat
- AsthmaDokumen4 halamanAsthmaEd CBelum ada peringkat
- The Complete Guide To Functional Training (PDFDrive)Dokumen552 halamanThe Complete Guide To Functional Training (PDFDrive)carlosBelum ada peringkat
- Senior Boot CampDokumen35 halamanSenior Boot CampEd C100% (1)
- Strength SmallDokumen1 halamanStrength SmallEd CBelum ada peringkat
- Iec 383Dokumen1 halamanIec 383rohitjhangraindiaBelum ada peringkat
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5782)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (587)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (72)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (119)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- Dental Chair Positions GuideDokumen35 halamanDental Chair Positions GuideFaye Nervanna Alecha Alferez100% (1)
- Strength Size or Power PDFDokumen5 halamanStrength Size or Power PDFSphinx Strong100% (2)
- 0610 s07 QP 2Dokumen24 halaman0610 s07 QP 2Hubbak Khan100% (3)
- Animal Physiology, Fourth EditionDokumen2 halamanAnimal Physiology, Fourth EditionCamila GuzmanBelum ada peringkat
- Aging of PlantDokumen30 halamanAging of PlantMujahid HussainBelum ada peringkat
- Periodization in Football Training and the 6 Week ModelDokumen22 halamanPeriodization in Football Training and the 6 Week ModelDadan GunawanBelum ada peringkat
- Institute of Pharmacy S.Y. 2022 - 2023 1st Year I 2st Semester I Midterms Prof. Joshua Kenneth NGDokumen72 halamanInstitute of Pharmacy S.Y. 2022 - 2023 1st Year I 2st Semester I Midterms Prof. Joshua Kenneth NGJaden GonzagaBelum ada peringkat
- Psych 101 NotesDokumen19 halamanPsych 101 NotesAlison BlackBelum ada peringkat
- Lesson 5 - Disaster ManagementDokumen40 halamanLesson 5 - Disaster ManagementHampson MalekanoBelum ada peringkat
- RED CELL MORPHOLOGY Tabulation SummaryDokumen6 halamanRED CELL MORPHOLOGY Tabulation SummaryStephen YorBelum ada peringkat
- 2015-2016 SQ2 (Chemistry of Lipids and Biological Menbranes)Dokumen11 halaman2015-2016 SQ2 (Chemistry of Lipids and Biological Menbranes)Jerrica Charlene GalopeBelum ada peringkat
- Annotated Bibliography 1Dokumen8 halamanAnnotated Bibliography 1api-432883682Belum ada peringkat
- NEWS2 Chart 3 - NEWS Observation Chart - 0 PDFDokumen1 halamanNEWS2 Chart 3 - NEWS Observation Chart - 0 PDFcicaklomenBelum ada peringkat
- Presentation Metabolic SyndromeDokumen56 halamanPresentation Metabolic SyndromeAbdulhakeem Tleimat100% (1)
- B1 UNIT 4 Test 2Dokumen3 halamanB1 UNIT 4 Test 2Ваня ЯровойBelum ada peringkat
- The Lysosome As A Cellular Centre For Signalling, MetabolismDokumen10 halamanThe Lysosome As A Cellular Centre For Signalling, MetabolismHaru SahaBelum ada peringkat
- Healthy Living Event Proposal 2013 Group 3Dokumen7 halamanHealthy Living Event Proposal 2013 Group 3api-235001675Belum ada peringkat
- Tumours of The Central Nervous System: FM Brett MD., FrcpathDokumen57 halamanTumours of The Central Nervous System: FM Brett MD., FrcpathDrGasnasBelum ada peringkat
- 2016 Specimen Paper 4 Mark SchemeDokumen8 halaman2016 Specimen Paper 4 Mark SchemeAaa IiiBelum ada peringkat
- Characteristics of Keratinocytes in Facial Solar Lentigo With Flattened Rete Ridges - Comparison With MelasmaDokumen6 halamanCharacteristics of Keratinocytes in Facial Solar Lentigo With Flattened Rete Ridges - Comparison With MelasmaOzheanAMBelum ada peringkat
- Water Birth PPDokumen5 halamanWater Birth PPAzi SamiBelum ada peringkat
- Review of Laboratory and Diagnostic TestsDokumen41 halamanReview of Laboratory and Diagnostic TestsPutri Anggraini Rusanti100% (1)
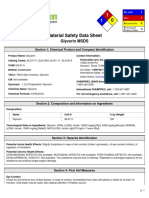
- Msds Glycerine Oil PDFDokumen6 halamanMsds Glycerine Oil PDFknabpshoBelum ada peringkat
- Lecture 4-Cell PolarityDokumen52 halamanLecture 4-Cell PolarityFarrelita Nayla GhaniBelum ada peringkat
- Neurologic Manifestations of Major Electrolyte AbnormalitiesDokumen9 halamanNeurologic Manifestations of Major Electrolyte AbnormalitiesMartha OktaviaBelum ada peringkat
- Terminology LabDokumen26 halamanTerminology LabياسرBelum ada peringkat
- Neuroanatomy Topic OutlineDokumen2 halamanNeuroanatomy Topic OutlineEdmar SumagaysayBelum ada peringkat
- Lecture Chapter 1 PDFDokumen30 halamanLecture Chapter 1 PDFmresearchBelum ada peringkat
- Medicowesome Glasgow Coma Scale Mnemonic 2Dokumen1 halamanMedicowesome Glasgow Coma Scale Mnemonic 2KC Dela RosaBelum ada peringkat
- Exam-4 Ecpe 1 2014 TeDokumen22 halamanExam-4 Ecpe 1 2014 TePoc100% (2)