Anda mungkin juga menyukai
- La Formula de La Felicidad - Alvaro AsensioDokumen76 halamanLa Formula de La Felicidad - Alvaro AsensioPercy Vasquez100% (1)
- Cuadro ComparativoDokumen8 halamanCuadro ComparativoJose Antonio Manuel Bello100% (2)
- Hipertension ArterialDokumen28 halamanHipertension ArterialAngie Carolina Pino MarquinaBelum ada peringkat
- Cardiopatia Isquemica e IamDokumen68 halamanCardiopatia Isquemica e IamMOMOSSBelum ada peringkat
- Trastornos Del Metabolismo Acido BaseDokumen41 halamanTrastornos Del Metabolismo Acido Baseluisa suarezBelum ada peringkat
- Pruebas Mecanicas AlimentosDokumen32 halamanPruebas Mecanicas AlimentosArturo Velasco50% (4)
- Sindrome MielodisplasicoDokumen43 halamanSindrome MielodisplasicoAdolfo Jesus Labarca CoronelBelum ada peringkat
- Cardiopatia IsquemicaDokumen19 halamanCardiopatia IsquemicaYudith Lisbeth Evaristo YrigoinBelum ada peringkat
- Evaluación Del Paciente en ComaDokumen46 halamanEvaluación Del Paciente en ComaGabriela Génesis Peca Ibarra100% (1)
- Evaluación Del Paciente en Coma y Con AlteraciónDokumen47 halamanEvaluación Del Paciente en Coma y Con Alteraciónsilvana guidiciBelum ada peringkat
- Evaluacion Financiera de ProyectosDokumen55 halamanEvaluacion Financiera de ProyectosAngie Rodríguez100% (2)
- Síndrome Antifosfolípidos en El EmbarazoDokumen8 halamanSíndrome Antifosfolípidos en El EmbarazoMagaly PuertoBelum ada peringkat
- Hta ExposicionDokumen77 halamanHta ExposicionEvelyn Dayana100% (1)
- Resumen. Hiper e Hipoparatiroidismo PDFDokumen15 halamanResumen. Hiper e Hipoparatiroidismo PDFGarcía PérezBelum ada peringkat
- Hallazgos Normales y Patológicos Del Recien NacidoDokumen42 halamanHallazgos Normales y Patológicos Del Recien NacidoElvis Valdez MecaBelum ada peringkat
- Semiología Resumen Síndromes ValvularesDokumen1 halamanSemiología Resumen Síndromes ValvularesCristhián Ignacio Jerez FernándezBelum ada peringkat
- 2016 SincopeDokumen8 halaman2016 SincopeSebastian Adolfo Palma MoragaBelum ada peringkat
- Hipertensión Arterial SistémicaDokumen34 halamanHipertensión Arterial Sistémicafrancisco88rg100% (1)
- POLIMIOSITISDokumen22 halamanPOLIMIOSITISGiovanna Marroquin0% (1)
- Fisiologia EndocrinaDokumen39 halamanFisiologia EndocrinaTomas Garciaguirre100% (1)
- Neumopatías Intersticiales DifusasDokumen33 halamanNeumopatías Intersticiales DifusasCarlos M Garcia LaraBelum ada peringkat
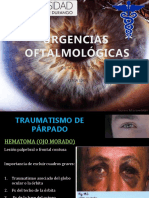
- Urgencias OftalmicasDokumen54 halamanUrgencias OftalmicasMaria Fernanda RG100% (1)
- Grupo#5 - Síndrome Coronario AgudoDokumen53 halamanGrupo#5 - Síndrome Coronario AgudoNicole AlvarezBelum ada peringkat
- Gastritis y UlcerasDokumen19 halamanGastritis y UlcerasNelly Fátima Bravo Huamán100% (1)
- 2.sind NefroticoDokumen22 halaman2.sind NefroticoDavid ArbildoBelum ada peringkat
- SX CushingDokumen8 halamanSX CushingBrandom Bautista RamirezBelum ada peringkat
- Diabetes y Embarazo.Dokumen31 halamanDiabetes y Embarazo.19candy19Belum ada peringkat
- Guia Clinica Diabetes Mellitus Tipo 2 2009 ChileDokumen73 halamanGuia Clinica Diabetes Mellitus Tipo 2 2009 ChileViejo MolinaBelum ada peringkat
- PalpitacionesDokumen33 halamanPalpitacionesapi-3697245100% (1)
- Casos Clínicos de Cardiovascular de Pequeños AnimalesDokumen4 halamanCasos Clínicos de Cardiovascular de Pequeños Animalesbromor1113Belum ada peringkat
- Urgencias en Oftalmologia IpsDokumen54 halamanUrgencias en Oftalmologia IpsjhzapataBelum ada peringkat
- Hiperparatiroidismo Primario y SecundarioDokumen4 halamanHiperparatiroidismo Primario y Secundariomegaslug1691Belum ada peringkat
- Examen Practico HistologiaDokumen22 halamanExamen Practico HistologiaJoseph Rosado MorenoBelum ada peringkat
- Mais - MSPDokumen12 halamanMais - MSPMaría Salazar EspinozaBelum ada peringkat
- 1 Oficio Solicitud de PlazaDokumen1 halaman1 Oficio Solicitud de Plazathaly narvaezBelum ada peringkat
- Histologia de Las Glandulas SalivalesDokumen9 halamanHistologia de Las Glandulas SalivalesEdmar Angel Aguilar LeyvaBelum ada peringkat
- Normas de Atención Integral A La Niñez 2011 PDFDokumen126 halamanNormas de Atención Integral A La Niñez 2011 PDFAlberto Romero CedeñoBelum ada peringkat
- Sindrome Coronario Agudo 2023-IDokumen45 halamanSindrome Coronario Agudo 2023-Ijuan diego huaman ramirezBelum ada peringkat
- Guia de Diabetes MellitusDokumen82 halamanGuia de Diabetes Mellituscarlos rBelum ada peringkat
- Sindrome de CushingDokumen193 halamanSindrome de CushingAngel MCBelum ada peringkat
- Tratamiento HiponatremiaDokumen26 halamanTratamiento HiponatremiaJota Mario Martínez CardenasBelum ada peringkat
- Trastornos de PotasioDokumen23 halamanTrastornos de PotasioAndres F BarriosBelum ada peringkat
- PALPITACIONESDokumen3 halamanPALPITACIONESliliana navarroBelum ada peringkat
- Intoxicación Por CocaínaDokumen32 halamanIntoxicación Por CocaínaIunius InventusBelum ada peringkat
- Exposicion Derrame Pleural, Absceso Pulmonar, EmpiemaDokumen37 halamanExposicion Derrame Pleural, Absceso Pulmonar, EmpiemaValeria CastroBelum ada peringkat
- AnemiaDokumen27 halamanAnemiaCassiel LopezBelum ada peringkat
- CEFALEA UrgenciasDokumen25 halamanCEFALEA UrgenciasNeurologia FedllerasBelum ada peringkat
- Enfermedades Autoinmunes Del Sistema CardiovascularDokumen33 halamanEnfermedades Autoinmunes Del Sistema CardiovascularAlba Yaneth GutierrezBelum ada peringkat
- Clase 7 CefaleaDokumen18 halamanClase 7 Cefaleaanon-766286Belum ada peringkat
- Asma BronquialDokumen14 halamanAsma BronquialIriana Nathaly Joya García100% (1)
- Retinopatia HipertensivaDokumen11 halamanRetinopatia HipertensivaZoila Castro Uriol100% (1)
- Gases Arteriales y Equilibrio HidroelectrolíticoDokumen61 halamanGases Arteriales y Equilibrio HidroelectrolíticoAngelica FuentesBelum ada peringkat
- HIPERTENSION ARTERIAL InternadoDokumen6 halamanHIPERTENSION ARTERIAL Internadoceciliaaandrea1Belum ada peringkat
- Antihipertensivos 2018Dokumen76 halamanAntihipertensivos 2018Martica RamosBelum ada peringkat
- Hipertension ArterialDokumen29 halamanHipertension Arterialedwin andres restrepo garciaBelum ada peringkat
- Fisiopatologia HTADokumen61 halamanFisiopatologia HTAMiriam Atoche EstelaBelum ada peringkat
- Hipertension Arterial TEMA 1Dokumen63 halamanHipertension Arterial TEMA 1gerson1contreras-167% (3)
- Seminario 1 - Urgencias y Emergencias HipertensivasDokumen14 halamanSeminario 1 - Urgencias y Emergencias HipertensivasJean Pierre del Aguila MattaBelum ada peringkat
- Hipertension Arterial SistemicaDokumen27 halamanHipertension Arterial SistemicaEzgar VillanuevaBelum ada peringkat
- Hta 2022Dokumen25 halamanHta 2022Cristopher SosaBelum ada peringkat
- Hipertension Arterial Ronald Celi Celi Nov 2020Dokumen83 halamanHipertension Arterial Ronald Celi Celi Nov 2020antony orozcoBelum ada peringkat
- 1º ROTAFOLIO HipertencionDokumen41 halaman1º ROTAFOLIO Hipertencionpaola sofia cordova huamaniBelum ada peringkat
- Algoritmo HipertensionDokumen1 halamanAlgoritmo HipertensionAnthony silupu espinozaBelum ada peringkat
- Patologia de Las Glandulas Anexas Al Tubo DigestivoDokumen35 halamanPatologia de Las Glandulas Anexas Al Tubo DigestivoAdolfo Jesus Labarca CoronelBelum ada peringkat
- Bases ConissDokumen8 halamanBases ConissAdolfo Jesus Labarca CoronelBelum ada peringkat
- Discrasias SanguíneasDokumen49 halamanDiscrasias SanguíneasanayancylcBelum ada peringkat
- MovimaDokumen10 halamanMovimaNicol ApBelum ada peringkat
- Tecnicas de Radiofarmacia.2º Idmn PDFDokumen32 halamanTecnicas de Radiofarmacia.2º Idmn PDFmariaBelum ada peringkat
- Artropodos 2018Dokumen224 halamanArtropodos 2018Jorge Janampa Campos100% (3)
- 3.4 Medidas de Tendencia CentralDokumen13 halaman3.4 Medidas de Tendencia CentralCarlos SolanoBelum ada peringkat
- Ejercicios CohesiónDokumen6 halamanEjercicios CohesiónMarta Gallego medinaBelum ada peringkat
- Protección AuditivaDokumen2 halamanProtección AuditivasabyBelum ada peringkat
- Protocolo de Acceso 10Dokumen6 halamanProtocolo de Acceso 10Jose DiazBelum ada peringkat
- Preguntas Selectividad Bloque MetabolismoDokumen16 halamanPreguntas Selectividad Bloque MetabolismoLucía FO100% (1)
- Equilibrio IonicoDokumen23 halamanEquilibrio IonicoFroilan CanquiBelum ada peringkat
- INVENTARIO DEL LABORATORIO DE LA INSTITUCION SAN FRANCISCO DEL RAYO (Nuevo)Dokumen2 halamanINVENTARIO DEL LABORATORIO DE LA INSTITUCION SAN FRANCISCO DEL RAYO (Nuevo)Jose Eduardo Salazar SandovalBelum ada peringkat
- Anemias Parte 1Dokumen5 halamanAnemias Parte 1Alex HidalgoBelum ada peringkat
- Huella de Carbono YoneiderDokumen25 halamanHuella de Carbono YoneiderYONEIDER JOSE MENDOZA GAMEZ (:-)Belum ada peringkat
- La Importancia de Ser Como NiñosDokumen9 halamanLa Importancia de Ser Como NiñosMilagros Rodriguez FerminBelum ada peringkat
- Todo Tipo de OracionesDokumen2 halamanTodo Tipo de OracionesPaco Ramos derquiBelum ada peringkat
- Catalogo Reles de Monitoreo y ControlDokumen16 halamanCatalogo Reles de Monitoreo y ControlFernando MontejanoBelum ada peringkat
- Ochitekita Naga Ryuuou To Horobiyuku Majo No Kuni-Volumen IIIDokumen283 halamanOchitekita Naga Ryuuou To Horobiyuku Majo No Kuni-Volumen IIIPablo Andree Bautista lajoBelum ada peringkat
- Cuadro Sinóptico ConductismoDokumen1 halamanCuadro Sinóptico ConductismoAngelica FuentesBelum ada peringkat
- Tesina Jorge Baños PDFDokumen264 halamanTesina Jorge Baños PDFpaulkohanBelum ada peringkat
- Tarea Línea Del Tiempo 10 Melvia MorenoDokumen3 halamanTarea Línea Del Tiempo 10 Melvia MorenoMelvia MorenoBelum ada peringkat
- Trabajo de Cimentaciones Ultimo-Hamilton Abal GarciaDokumen34 halamanTrabajo de Cimentaciones Ultimo-Hamilton Abal GarciaYesy GonzalesBelum ada peringkat
- Escuelas Arriba 5to Año Básico 2021Dokumen3 halamanEscuelas Arriba 5to Año Básico 2021María Eugenia Lara PonceBelum ada peringkat
- Caso 1Dokumen7 halamanCaso 1Juan PradoBelum ada peringkat
- 1.5 - PPA Primera Etapa Ecosistema MarinoDokumen7 halaman1.5 - PPA Primera Etapa Ecosistema Marinojavier alexisBelum ada peringkat
- PROYECTO VIDA SALUDABLE BUENA ALIMENTACION Williams LDokumen32 halamanPROYECTO VIDA SALUDABLE BUENA ALIMENTACION Williams LRonald SolisBelum ada peringkat
- Cartilla - Programacion de Maquinas CNCDokumen31 halamanCartilla - Programacion de Maquinas CNCNicolas CuellarBelum ada peringkat
- Econsejo 4 Los ColoidesDokumen21 halamanEconsejo 4 Los ColoidesAsun ArribaBelum ada peringkat