Anda mungkin juga menyukai
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (399)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Physical Examination AbdomenDokumen249 halamanPhysical Examination AbdomenDrbee10100% (1)
- Physioex Lab Report: Pre-Lab Quiz ResultsDokumen4 halamanPhysioex Lab Report: Pre-Lab Quiz ResultsNovanza RayhanBelum ada peringkat
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (73)
- Acute Kidney Injury W/ Hyperkalemia NCPDokumen5 halamanAcute Kidney Injury W/ Hyperkalemia NCPMyrvic Ortiz La OrdenBelum ada peringkat
- Eric Berg CVDokumen6 halamanEric Berg CVHaralambicBelum ada peringkat
- DRUG STUDY PsycheDokumen1 halamanDRUG STUDY Psychejulesubayubay5428100% (1)
- Prostho MCQ Www-Matterhere-Com NRRDokumen10 halamanProstho MCQ Www-Matterhere-Com NRRYoung FlameBelum ada peringkat
- An Advanced Laboratory Manual of Organic ChemistryDokumen103 halamanAn Advanced Laboratory Manual of Organic Chemistryalkem7100% (1)
- Part1 WHOStandardAccupuncturePointLocationsDokumen39 halamanPart1 WHOStandardAccupuncturePointLocationsJiman Ryu100% (1)
- Pre-Test Maternal and Child Health NursingDokumen18 halamanPre-Test Maternal and Child Health NursingDefensor Pison GringgoBelum ada peringkat
- Bansenshukai 000Dokumen0 halamanBansenshukai 000graalstBelum ada peringkat
- Review of Literature on Rabies Prevention and ControlDokumen24 halamanReview of Literature on Rabies Prevention and ControlBeah Claudette AbundoBelum ada peringkat
- Cataract BookDokumen261 halamanCataract Bookstarsk777Belum ada peringkat
- Donguibogam: Principles and Practice of Eastern MedicineDokumen15 halamanDonguibogam: Principles and Practice of Eastern Medicine小次郎 佐々木Belum ada peringkat
- Ectwo Biology and The: Future of MediclneDokumen4 halamanEctwo Biology and The: Future of Mediclne小次郎 佐々木Belum ada peringkat
- Some Field Methods in Medical Ethnobiology: University of GeorgiaDokumen34 halamanSome Field Methods in Medical Ethnobiology: University of Georgia小次郎 佐々木Belum ada peringkat
- Raveling Oward THE Nknown: L C S N YDokumen14 halamanRaveling Oward THE Nknown: L C S N Y小次郎 佐々木Belum ada peringkat
- c2Dokumen18 halamanc2小次郎 佐々木Belum ada peringkat
- Wu 2014Dokumen10 halamanWu 2014小次郎 佐々木Belum ada peringkat
- The Science of Mesotherapy: Chemical Anarchy: Hot TopicsDokumen4 halamanThe Science of Mesotherapy: Chemical Anarchy: Hot Topics小次郎 佐々木Belum ada peringkat
- Pankaj Article BonesettingDokumen6 halamanPankaj Article Bonesetting小次郎 佐々木Belum ada peringkat
- Utovsk 2015Dokumen38 halamanUtovsk 2015小次郎 佐々木Belum ada peringkat
- Chinaperspectives 5621Dokumen9 halamanChinaperspectives 5621小次郎 佐々木Belum ada peringkat
- The Science of Mesotherapy: Chemical Anarchy: Hot TopicsDokumen4 halamanThe Science of Mesotherapy: Chemical Anarchy: Hot Topics小次郎 佐々木Belum ada peringkat
- Barrett 2003Dokumen21 halamanBarrett 2003小次郎 佐々木Belum ada peringkat
- Strategic Resource Use For Learning: A Self-Administered Intervention That Guides Self-Reflection On Effective Resource Use Enhances Academic PerformanceDokumen12 halamanStrategic Resource Use For Learning: A Self-Administered Intervention That Guides Self-Reflection On Effective Resource Use Enhances Academic Performance小次郎 佐々木Belum ada peringkat
- Guidelines Clinical Research On AcupunctureDokumen66 halamanGuidelines Clinical Research On AcupuncturebcalichiamaBelum ada peringkat
- Zhang 2012Dokumen7 halamanZhang 2012小次郎 佐々木Belum ada peringkat
- 1 s2.0 S2005290110600015 MainDokumen9 halaman1 s2.0 S2005290110600015 Main小次郎 佐々木Belum ada peringkat
- Zeng 2017Dokumen20 halamanZeng 2017小次郎 佐々木Belum ada peringkat
- 23 1 PDFDokumen5 halaman23 1 PDF小次郎 佐々木100% (1)
- Peripheral Mechanisms of Burn Injury Associated PainDokumen10 halamanPeripheral Mechanisms of Burn Injury Associated Pain小次郎 佐々木Belum ada peringkat
- Medicinal Plants For The Treatment of Nervios Anxiety and Depression in Mexican Traditional Medicine - 2014 - Revista Brasileira de Farmacognosia PDFDokumen18 halamanMedicinal Plants For The Treatment of Nervios Anxiety and Depression in Mexican Traditional Medicine - 2014 - Revista Brasileira de Farmacognosia PDFGabriela OliveiraBelum ada peringkat
- Claudia Focks - Icons TerminologyDokumen2 halamanClaudia Focks - Icons Terminology小次郎 佐々木Belum ada peringkat
- Improved Germination American Ginseng Seeds PDFDokumen5 halamanImproved Germination American Ginseng Seeds PDF小次郎 佐々木Belum ada peringkat
- Flower 2016Dokumen7 halamanFlower 2016小次郎 佐々木Belum ada peringkat
- Zeng 2017Dokumen20 halamanZeng 2017小次郎 佐々木Belum ada peringkat
- Patogenesis MelasmaDokumen7 halamanPatogenesis MelasmaYessicaBelum ada peringkat
- Culltivation of American Ginseng PDFDokumen18 halamanCulltivation of American Ginseng PDF小次郎 佐々木Belum ada peringkat
- US Elsevier Health Bookshop - Mosby, Saunders, Netter & MoreDokumen4 halamanUS Elsevier Health Bookshop - Mosby, Saunders, Netter & MoreWilmer Zambrano GuerreroBelum ada peringkat
- Expression of MDM2 and p16 in AngiomyolipomaDokumen7 halamanExpression of MDM2 and p16 in AngiomyolipomaTiago TavaresBelum ada peringkat
- Daftar PustakaDokumen2 halamanDaftar PustakaNurfauziyahBelum ada peringkat
- Buletin Farmasi 1/2014Dokumen14 halamanBuletin Farmasi 1/2014afiq83100% (1)
- Conscious Sedation PaediatricsDokumen44 halamanConscious Sedation PaediatricsReeta TaxakBelum ada peringkat
- Chest XrayDokumen6 halamanChest XrayAjit KumarBelum ada peringkat
- Bladder Cancer Types, Symptoms, Tests & TreatmentDokumen1 halamanBladder Cancer Types, Symptoms, Tests & TreatmentCarmina AguilarBelum ada peringkat
- Effects of Malnutrition Among ChildrenDokumen3 halamanEffects of Malnutrition Among ChildrenDesiree Aranggo MangueraBelum ada peringkat
- The Partograph: Dr. Rimonta F Gunanegara, SpogDokumen30 halamanThe Partograph: Dr. Rimonta F Gunanegara, SpogHans Natanael PosoBelum ada peringkat
- Hypertension in PregnancyDokumen18 halamanHypertension in Pregnancyshubham kumarBelum ada peringkat
- Ligibel JA Et Al. 2022 Exercise, Diet and Weight Management During Cancer Treatment - ASCO GuidelineDokumen20 halamanLigibel JA Et Al. 2022 Exercise, Diet and Weight Management During Cancer Treatment - ASCO GuidelineJasmyn KimBelum ada peringkat
- Abnormal PuerperiumDokumen65 halamanAbnormal PuerperiumNigus AfessaBelum ada peringkat
- IV Drug ReactionsDokumen19 halamanIV Drug Reactionsphp_czarina04421Belum ada peringkat
- Definition of NephrolithiasisDokumen30 halamanDefinition of Nephrolithiasiszz_13Belum ada peringkat
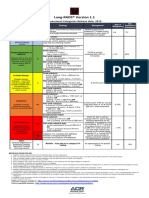
- Lung RADS® Version 1.1: Assessment Categories Release Date: 2019Dokumen1 halamanLung RADS® Version 1.1: Assessment Categories Release Date: 2019S Francisco MotBelum ada peringkat
- TimeWise Miracle Set 3D Fact Sheet MYSG ENGDokumen2 halamanTimeWise Miracle Set 3D Fact Sheet MYSG ENGKilinSilinBelum ada peringkat
- Bull InfertilDokumen29 halamanBull InfertilYonaaasBelum ada peringkat
- Uncorrected Author ProofDokumen15 halamanUncorrected Author ProofindahBelum ada peringkat
- Windkessel EffectDokumen11 halamanWindkessel EffectAkhmad HidayatBelum ada peringkat
- UAS Genap Semester II Kebidanan STIKES HafshawatyDokumen3 halamanUAS Genap Semester II Kebidanan STIKES HafshawatyHanna HannaBelum ada peringkat
- Lesson 3 ReviewDokumen4 halamanLesson 3 ReviewHo Yong WaiBelum ada peringkat