Anda mungkin juga menyukai
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5795)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (74)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (400)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- Usg PidDokumen13 halamanUsg PidHisbulloh syarifBelum ada peringkat
- Bones Flash CardDokumen22 halamanBones Flash CardMiki AberaBelum ada peringkat
- Dr. Sourav Chakraborty (Kolkata, Durgapur)Dokumen5 halamanDr. Sourav Chakraborty (Kolkata, Durgapur)thadanikrishBelum ada peringkat
- Dental ImplantDokumen37 halamanDental ImplantrejipgBelum ada peringkat
- Quiz 3 MATERNAL BSN2 SFDokumen2 halamanQuiz 3 MATERNAL BSN2 SFElaiza Anne SanchezBelum ada peringkat
- Undetectable Hair Transplants by Dr. Ch. Krishna PriyaDokumen155 halamanUndetectable Hair Transplants by Dr. Ch. Krishna PriyaKrishna RayaluBelum ada peringkat
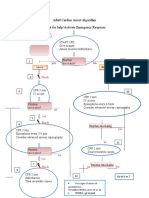
- Adult Cardiac Arrest Algorithm Shout For Help/activate Emergency ResponseDokumen1 halamanAdult Cardiac Arrest Algorithm Shout For Help/activate Emergency ResponseICU RSBMBelum ada peringkat
- Gingival Tissue ManagementDokumen144 halamanGingival Tissue ManagementMakkapati AmaniBelum ada peringkat
- EVALUATION Book Intern Medical-2023 Report 2Dokumen1 halamanEVALUATION Book Intern Medical-2023 Report 2Ahsif IsmailBelum ada peringkat
- Urine EliminationDokumen33 halamanUrine EliminationInnocent MuhumuzaBelum ada peringkat
- Menstrual - Disorders 2Dokumen24 halamanMenstrual - Disorders 2Abdibaset Mohamed AdenBelum ada peringkat
- AppendectomyDokumen51 halamanAppendectomymoqtadirBelum ada peringkat
- Paranasal Sinuses by DR SharakyDokumen21 halamanParanasal Sinuses by DR SharakyMobile AsdBelum ada peringkat
- Ob Clinical Worksheet - IntrapartumDokumen8 halamanOb Clinical Worksheet - Intrapartumcandice lavigneBelum ada peringkat
- Delorenzi 2017Dokumen3 halamanDelorenzi 2017Marilia RezendeBelum ada peringkat
- Periocular Hyaluronic Acid Fillers: Applications, Implications, ComplicationsDokumen6 halamanPeriocular Hyaluronic Acid Fillers: Applications, Implications, ComplicationsLuis Fernando WeffortBelum ada peringkat
- CPG - Management of Breast Cancer (2nd Edition)Dokumen100 halamanCPG - Management of Breast Cancer (2nd Edition)umiraihana1Belum ada peringkat
- Shock 2022 SeminarDokumen17 halamanShock 2022 Seminarrosie100% (2)
- Guide To Dental Treatment BandsDokumen2 halamanGuide To Dental Treatment BandsVikram Kapur100% (1)
- EG-580UT Operation ManualDokumen112 halamanEG-580UT Operation Manualkeng suttisangchanBelum ada peringkat
- Evidence Review 7Dokumen573 halamanEvidence Review 7Gracia Putra SecundaBelum ada peringkat
- CPT Coding Examples For Common Spine Procedures: CervicalDokumen5 halamanCPT Coding Examples For Common Spine Procedures: CervicalKrishna KumarBelum ada peringkat
- 3 High Risk PregnancyDokumen103 halaman3 High Risk PregnancyKaguraBelum ada peringkat
- 7.consent For Dental Implant SurgeryDokumen3 halaman7.consent For Dental Implant SurgeryPaul MathaiBelum ada peringkat
- Pancreatic Solid LeasionsDokumen24 halamanPancreatic Solid LeasionsEliza CrăciunBelum ada peringkat
- Special Leave Benefits For Women PDFDokumen2 halamanSpecial Leave Benefits For Women PDFJoan CarigaBelum ada peringkat
- Duodenal Injuries: E. Degiannis and K. BoffardDokumen7 halamanDuodenal Injuries: E. Degiannis and K. BoffardriftaBelum ada peringkat
- Dr. Yudha Mathan Sakti, Sp. OT (K) Limb Saving-Rahadyan Magetsari (2016)Dokumen56 halamanDr. Yudha Mathan Sakti, Sp. OT (K) Limb Saving-Rahadyan Magetsari (2016)dewiswahyuBelum ada peringkat
- Aortic Valve StenosisDokumen4 halamanAortic Valve StenosisYrag NoznipBelum ada peringkat
- Periodontology 2000 - 2023 - Liñares - Critical Review On Bone Grafting During Immediate Implant PlacementDokumen18 halamanPeriodontology 2000 - 2023 - Liñares - Critical Review On Bone Grafting During Immediate Implant Placementahmadalturaiki1Belum ada peringkat