Anda mungkin juga menyukai
- Kardiologi: Muhammad Arief Munandhar, MDDokumen9 halamanKardiologi: Muhammad Arief Munandhar, MDArief MunandharBelum ada peringkat
- Cover Pleuritis TBDokumen1 halamanCover Pleuritis TBArief MunandharBelum ada peringkat
- Kardiologi: Muhammad Arief Munandhar, MDDokumen9 halamanKardiologi: Muhammad Arief Munandhar, MDArief MunandharBelum ada peringkat
- 2017Dokumen5 halaman2017Arief MunandharBelum ada peringkat
- Hubungan Antara Abdominal Perfusion Pressure: (App) Dengan Outcome Post OperasiDokumen17 halamanHubungan Antara Abdominal Perfusion Pressure: (App) Dengan Outcome Post OperasidrelvBelum ada peringkat
- Nutrisi Pra Konsepsi PDFDokumen44 halamanNutrisi Pra Konsepsi PDFArief MunandharBelum ada peringkat
- PPHDokumen7 halamanPPHArief MunandharBelum ada peringkat
- Standard Case Report Checklist and Template For AuthorsDokumen5 halamanStandard Case Report Checklist and Template For AuthorsArief MunandharBelum ada peringkat
- VOLUME RESUSCITATION IN SHOCK STATE PPDS I Prof HanafiDokumen78 halamanVOLUME RESUSCITATION IN SHOCK STATE PPDS I Prof HanafiArief MunandharBelum ada peringkat
- Chronic Otitis Media: Chunfu Dai M.D & Ph. D Otolaryngology Department Eye Ear Nose and Throat Hospital Fudan UniversityDokumen25 halamanChronic Otitis Media: Chunfu Dai M.D & Ph. D Otolaryngology Department Eye Ear Nose and Throat Hospital Fudan UniversityChristman SihiteBelum ada peringkat
- 02 02 Original PyonephrosisDokumen4 halaman02 02 Original PyonephrosisArief MunandharBelum ada peringkat
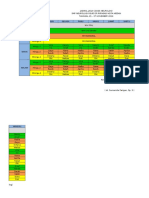
- Jadwal Jaga 21 - 27 NovemberDokumen2 halamanJadwal Jaga 21 - 27 NovemberArief MunandharBelum ada peringkat
- Pionefroze EnglDokumen10 halamanPionefroze EnglArief MunandharBelum ada peringkat
- Intracranial Dural Arteriovenous Fistulae: by Timothy R. Miller, and Dheeraj GandhiDokumen5 halamanIntracranial Dural Arteriovenous Fistulae: by Timothy R. Miller, and Dheeraj GandhiArief MunandharBelum ada peringkat
- Bakul SepsisDokumen42 halamanBakul SepsisRegina HershaaBelum ada peringkat
- Journal Hirchprung's DiseaseDokumen14 halamanJournal Hirchprung's DiseaseArief MunandharBelum ada peringkat
- Typhoid Fever & Pneumonia CaseDokumen4 halamanTyphoid Fever & Pneumonia CaseArief MunandharBelum ada peringkat
- Dermatophyte TestDokumen2 halamanDermatophyte TestArief MunandharBelum ada peringkat
- Anzcor Basic Life Support FlowchartDokumen1 halamanAnzcor Basic Life Support FlowchartGeethanjali SadasivamBelum ada peringkat
- AboutHydrocephalus-A Book For Families Dec08Dokumen40 halamanAboutHydrocephalus-A Book For Families Dec08rudy.langeBelum ada peringkat
- Study Guide Respiratory Semester VI 16 Pebruari 2015Dokumen50 halamanStudy Guide Respiratory Semester VI 16 Pebruari 2015Adi ParamarthaBelum ada peringkat
- Tinea PedisDokumen16 halamanTinea PedisArief MunandharBelum ada peringkat
- Bipolar disorder management in adults, children and adolescentsDokumen9 halamanBipolar disorder management in adults, children and adolescentsSepti Norfa RindaBelum ada peringkat
- Etiologi Efusi PericardDokumen1 halamanEtiologi Efusi PericardArief MunandharBelum ada peringkat
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (399)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (73)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (120)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- Pediatric Surgery HandbookDokumen75 halamanPediatric Surgery HandbookAlex Vătau100% (2)
- Multiple Sclerosis (MS)Dokumen15 halamanMultiple Sclerosis (MS)Arianna Jasmine MabungaBelum ada peringkat
- Common Congenital Git Malformations FinDokumen60 halamanCommon Congenital Git Malformations FinRuth DanielBelum ada peringkat
- Hirschsprungs DiseaseDokumen39 halamanHirschsprungs DiseaseYolanda Octaviana TariganBelum ada peringkat
- ILA - Hirschsprungs DiseaseDokumen48 halamanILA - Hirschsprungs DiseaseSoleh Ramly100% (1)
- AbdomenDokumen23 halamanAbdomenjnyamusiBelum ada peringkat
- Pediatric GI RadiologyDokumen6 halamanPediatric GI Radiologysarguss14Belum ada peringkat
- Paediatric Q & ADokumen47 halamanPaediatric Q & AHafizuddin RazidBelum ada peringkat
- Coloi Eeml Disease: Original ArticlesDokumen67 halamanColoi Eeml Disease: Original ArticlesLuisAngelPonceTorresBelum ada peringkat
- Hisprung DiseaseDokumen12 halamanHisprung DiseaseEky Madyaning NastitiBelum ada peringkat
- 19-Pediatric SurgeryDokumen39 halaman19-Pediatric Surgerycallisto3487Belum ada peringkat
- Hirschsprung 'S Disease: Incidence and Classi FicationDokumen6 halamanHirschsprung 'S Disease: Incidence and Classi FicationGhina Mauizha WulandariBelum ada peringkat
- 2015 PM Lecture 4 Barium EnemaDokumen62 halaman2015 PM Lecture 4 Barium EnemaObrian ReidBelum ada peringkat
- MT 1Dokumen57 halamanMT 1Bibek goitBelum ada peringkat
- Pediatric Nursing 1: Points 100 Questions 100 Time Limit 90 MinutesDokumen54 halamanPediatric Nursing 1: Points 100 Questions 100 Time Limit 90 MinutesSean Lloyd RigonBelum ada peringkat
- Hirschsprung's Disease and The Allied Disorders PDFDokumen278 halamanHirschsprung's Disease and The Allied Disorders PDFriri siahaanBelum ada peringkat
- Handbook of PEDIATRIC SURGERY PDFDokumen43 halamanHandbook of PEDIATRIC SURGERY PDFPETERBelum ada peringkat
- Chirurgie Pediatrica Engleza 125 Teste 2019 08.02.2019Dokumen25 halamanChirurgie Pediatrica Engleza 125 Teste 2019 08.02.2019gm hashBelum ada peringkat
- Constipation in ChildrenDokumen9 halamanConstipation in Childrenozoemena29Belum ada peringkat
- Askep HisprungDokumen25 halamanAskep HisprungRika AmaliyaBelum ada peringkat
- Hirschsprung DiseaseDokumen96 halamanHirschsprung DiseaseHariette Delmo de Leon100% (1)
- Chapter 28 Child With A Gastrointestinal ConditionDokumen85 halamanChapter 28 Child With A Gastrointestinal Conditionsey_scottBelum ada peringkat
- Pediatric Imaging Cases: Mysteries Solved with RadiologyDokumen82 halamanPediatric Imaging Cases: Mysteries Solved with Radiologyabakferro0% (1)
- Pedia 102 MIDTERM EXAMSDokumen15 halamanPedia 102 MIDTERM EXAMSquidditch07Belum ada peringkat
- Hirchsprung's DiseaseDokumen11 halamanHirchsprung's DiseaseMariah Alexis EncinaBelum ada peringkat
- CholostomyDokumen10 halamanCholostomySinta AnggrainiBelum ada peringkat
- Chapter 23 - The Child With Gastrointestinal Dysfunction Flashcards - QuizletDokumen30 halamanChapter 23 - The Child With Gastrointestinal Dysfunction Flashcards - QuizletJannah Mae PoligratesBelum ada peringkat
- Hirschprung Associated EnterocolitisDokumen9 halamanHirschprung Associated Enterocolitiskeyla_shineeeBelum ada peringkat
- Constipation: Practice GapsDokumen16 halamanConstipation: Practice GapsMafer LealBelum ada peringkat
- Friedmacher2013Classification and Diagnostic Criteria of Hirschprung DiseaseDokumen18 halamanFriedmacher2013Classification and Diagnostic Criteria of Hirschprung DiseaseMelchizedek M. SantanderBelum ada peringkat