Anda mungkin juga menyukai
- Survival and Austere MedicineDokumen614 halamanSurvival and Austere Medicinewilderd20100% (9)
- Diagnostic Laparoscopy in Penetrating Abdominal TraumaDokumen4 halamanDiagnostic Laparoscopy in Penetrating Abdominal TraumaNicolás Joel Peñalosa CupajitaBelum ada peringkat
- Antimicrobial ChemotherapyDokumen12 halamanAntimicrobial ChemotherapyArvi MandaweBelum ada peringkat
- Botany ProDokumen44 halamanBotany ProJishnu ABelum ada peringkat
- Antimicrobial AgentDokumen30 halamanAntimicrobial AgentShardendu MishraBelum ada peringkat
- Prompt Inoculation System-D-3251-3000 PDFDokumen40 halamanPrompt Inoculation System-D-3251-3000 PDFbogdan.tomosBelum ada peringkat
- Clsi 2012Dokumen50 halamanClsi 2012niluh suwasanti100% (1)
- Apendik KoesnadiDokumen4 halamanApendik KoesnadiUbay'z DillahBelum ada peringkat
- Jurnal FixDokumen2 halamanJurnal Fixuflah_Belum ada peringkat
- Research Paper Effectiveness of Conservative Management of Uncomplicated Acute Appendicitis: A Single Hospital Based Prospective StudyDokumen8 halamanResearch Paper Effectiveness of Conservative Management of Uncomplicated Acute Appendicitis: A Single Hospital Based Prospective StudyAnsoriBelum ada peringkat
- Critical Appraisal KADokumen36 halamanCritical Appraisal KAKentVilandkaBelum ada peringkat
- Journal of Pediatric Surgery: Steven L. Lee, Lara Spence, Kyle Mock, James X. Wu, Huan Yan, Daniel A. DeugarteDokumen6 halamanJournal of Pediatric Surgery: Steven L. Lee, Lara Spence, Kyle Mock, James X. Wu, Huan Yan, Daniel A. DeugarteMelian AnitaBelum ada peringkat
- Journal Reading AppendicitisDokumen24 halamanJournal Reading AppendicitisMira PrawiraBelum ada peringkat
- FitulotomyDokumen5 halamanFitulotomyDenis StoicaBelum ada peringkat
- Perianal AbsesDokumen4 halamanPerianal AbsesRizki SatriaBelum ada peringkat
- Early Uncomplicated AppendicitDokumen8 halamanEarly Uncomplicated Appendicitaxl___Belum ada peringkat
- Vrijland Et Al-2002-British Journal of SurgeryDokumen5 halamanVrijland Et Al-2002-British Journal of SurgeryTivHa Cii Mpuzz MandjaBelum ada peringkat
- Corto y Largo PlazoDokumen6 halamanCorto y Largo PlazoElard Paredes MacedoBelum ada peringkat
- Study of Conservative Treatment in Uncomplicated Acute AppendicitisDokumen9 halamanStudy of Conservative Treatment in Uncomplicated Acute Appendicitisaryo aryoBelum ada peringkat
- Journal Medicine: The New EnglandDokumen7 halamanJournal Medicine: The New England'Muhamad Rofiq Anwar'Belum ada peringkat
- The Clinical Outcomes and Predictive Factors For.24Dokumen5 halamanThe Clinical Outcomes and Predictive Factors For.24KeziaBelum ada peringkat
- Management of Acute Upper Gastrointestinal Bleeding: Urgent Versus Early EndosDokumen5 halamanManagement of Acute Upper Gastrointestinal Bleeding: Urgent Versus Early EndosCarolina Ormaza GiraldoBelum ada peringkat
- Management of Acute Upper Gastrointestinal Bleeding: Urgent Versus Early EndosDokumen5 halamanManagement of Acute Upper Gastrointestinal Bleeding: Urgent Versus Early EndossamuelBelum ada peringkat
- Original Research PaperDokumen2 halamanOriginal Research Paperيحيى الجبليBelum ada peringkat
- Nah Incarcerated HerniaDokumen4 halamanNah Incarcerated Herniafelix_the_meowBelum ada peringkat
- A Prospective Study On Appendicular MassDokumen4 halamanA Prospective Study On Appendicular MassA BBelum ada peringkat
- The Besmart (Best Supportive Management For Adults Referred With Tonsillopharyngitis) Multicentre Observational StudyDokumen6 halamanThe Besmart (Best Supportive Management For Adults Referred With Tonsillopharyngitis) Multicentre Observational StudyArizkamhBelum ada peringkat
- Journal Homepage: - : IntroductionDokumen10 halamanJournal Homepage: - : IntroductionIJAR JOURNALBelum ada peringkat
- Ultrasonographic Usg Evaluation of Acute AppendiciDokumen8 halamanUltrasonographic Usg Evaluation of Acute AppendiciKurnia HandayaniBelum ada peringkat
- Liver A BSC DrainDokumen8 halamanLiver A BSC DrainAngelica AmesquitaBelum ada peringkat
- Chung PrognosisDokumen6 halamanChung PrognosisMarlyn SuciningtiasBelum ada peringkat
- Lintula Score & AppendicitisDokumen7 halamanLintula Score & AppendicitisAulia Eka Purwani0% (1)
- Ventosa Na Dor LombarDokumen7 halamanVentosa Na Dor Lombarmauricio da silva barbosaBelum ada peringkat
- f194 DikonversiDokumen5 halamanf194 DikonversiFarizka Dwinda HBelum ada peringkat
- Appropriate Antibiotics For Peritonsillar Abscess - A 9 Month CohortDokumen5 halamanAppropriate Antibiotics For Peritonsillar Abscess - A 9 Month CohortSiti Annisa NurfathiaBelum ada peringkat
- Critical Appraisal KADokumen35 halamanCritical Appraisal KAKentVilandkaBelum ada peringkat
- The Effect of Early Canalith Repositioning On Benign Paroxysmal Positional Vertigo On RecurrenceDokumen5 halamanThe Effect of Early Canalith Repositioning On Benign Paroxysmal Positional Vertigo On RecurrencezanafiraBelum ada peringkat
- Isj-5899 oDokumen5 halamanIsj-5899 oAbhiram MundleBelum ada peringkat
- Outcome and Clinical Characteristics in Pleural Empyema: A Retrospective StudyDokumen7 halamanOutcome and Clinical Characteristics in Pleural Empyema: A Retrospective StudylestarisurabayaBelum ada peringkat
- A Non-Operative Treatment of Perforated Peptic Ulcer: A Prospective Study With 50 CasesDokumen4 halamanA Non-Operative Treatment of Perforated Peptic Ulcer: A Prospective Study With 50 CasesSake Cinema21Belum ada peringkat
- Song 2018Dokumen7 halamanSong 2018Jonathan RyanBelum ada peringkat
- Methisoprinol y VPHDokumen4 halamanMethisoprinol y VPHAndres Gonzalez Cruz100% (1)
- Timing of Endoscopy For Acute Upper Gastrointestinal Bleeding: A Territory-Wide Cohort StudyDokumen7 halamanTiming of Endoscopy For Acute Upper Gastrointestinal Bleeding: A Territory-Wide Cohort StudyFaisal BaigBelum ada peringkat
- Togasj 6 25Dokumen6 halamanTogasj 6 25Prabowo SuryaningtyasBelum ada peringkat
- Research: Pain Over Speed Bumps in Diagnosis of Acute Appendicitis: Diagnostic Accuracy StudyDokumen7 halamanResearch: Pain Over Speed Bumps in Diagnosis of Acute Appendicitis: Diagnostic Accuracy StudydimasBelum ada peringkat
- Traning Schedule 2018Dokumen5 halamanTraning Schedule 2018alvaedison00Belum ada peringkat
- Low-Dose Abdominal CT For Evaluating Suspected Appendicitis: Original ArticleDokumen10 halamanLow-Dose Abdominal CT For Evaluating Suspected Appendicitis: Original ArticlePra YudhaBelum ada peringkat
- Journal AppraisalDokumen37 halamanJournal AppraisalLeahBelum ada peringkat
- Prospective Randomized Evaluation of Prophylactic Antibiotic Usage in Patients Undergoing Tension Free Inguinal HernioplastyDokumen6 halamanProspective Randomized Evaluation of Prophylactic Antibiotic Usage in Patients Undergoing Tension Free Inguinal HernioplastyYai El BaRcaBelum ada peringkat
- SRP2021 8848162Dokumen6 halamanSRP2021 8848162Maria AkulinaBelum ada peringkat
- Thumb Spica Cast For The Management of de Quervain, S TenosynovitisDokumen4 halamanThumb Spica Cast For The Management of de Quervain, S TenosynovitisJeanie WangsaBelum ada peringkat
- Early Use of TIPS in Cirrhosis and Variceal BleedingDokumen10 halamanEarly Use of TIPS in Cirrhosis and Variceal Bleedingray liBelum ada peringkat
- Clinical Correlation of Acute Appendicitis With Histopathological Diagnosis: A Prospective StudyDokumen5 halamanClinical Correlation of Acute Appendicitis With Histopathological Diagnosis: A Prospective StudyHarun NasutionBelum ada peringkat
- Journal Homepage: - : Manuscript HistoryDokumen8 halamanJournal Homepage: - : Manuscript HistoryIJAR JOURNALBelum ada peringkat
- Surgery & Surgical Procedures: International Journal ofDokumen3 halamanSurgery & Surgical Procedures: International Journal ofRinaldy T SetiawanBelum ada peringkat
- JournalDokumen37 halamanJournalLeahBelum ada peringkat
- A Study Into The Efficacy of OsteopathicDokumen11 halamanA Study Into The Efficacy of Osteopathicसंदीप गुप्ताBelum ada peringkat
- Adult Intussusception: A Retrospective ReviewDokumen5 halamanAdult Intussusception: A Retrospective ReviewkameliasitorusBelum ada peringkat
- @medicinejournal European Journal of Pediatric Surgery January 2020Dokumen126 halaman@medicinejournal European Journal of Pediatric Surgery January 2020Ricardo Uzcategui ArreguiBelum ada peringkat
- 1 s2.0 S0965229915000552 MainDokumen8 halaman1 s2.0 S0965229915000552 MainUtami DewiBelum ada peringkat
- IMU Learning Outcome: Psychomotor SkillsDokumen11 halamanIMU Learning Outcome: Psychomotor SkillsRameshBelum ada peringkat
- Chan 1997Dokumen5 halamanChan 1997Sree BanBelum ada peringkat
- Article ApendicitisDokumen7 halamanArticle ApendicitisXerexBelum ada peringkat
- El Beheiry2019Dokumen4 halamanEl Beheiry2019achmadaBelum ada peringkat
- Complementary and Alternative Medical Lab Testing Part 5: GastrointestinalDari EverandComplementary and Alternative Medical Lab Testing Part 5: GastrointestinalBelum ada peringkat
- Atlas of Early Neoplasias of the Gastrointestinal Tract: Endoscopic Diagnosis and Therapeutic DecisionsDari EverandAtlas of Early Neoplasias of the Gastrointestinal Tract: Endoscopic Diagnosis and Therapeutic DecisionsFrieder BerrBelum ada peringkat
- Renal Replacement Therapy in Acute Kidney Injury: Review: Blood Research & Transfusion JournalDokumen4 halamanRenal Replacement Therapy in Acute Kidney Injury: Review: Blood Research & Transfusion JournalNova SuryatiBelum ada peringkat
- Aortic Stenosis: Yerizal Karani MD Cardiology Division Faculty of Medicine Andalas UniversityDokumen29 halamanAortic Stenosis: Yerizal Karani MD Cardiology Division Faculty of Medicine Andalas UniversityNova SuryatiBelum ada peringkat
- Bacterial Aspect of The Cardiac DiseaseDokumen9 halamanBacterial Aspect of The Cardiac DiseaseNova SuryatiBelum ada peringkat
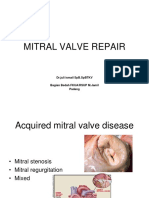
- Mitral Valve Repair: DR - Juli Ismail SPB - SPBTKV Bagian Bedah Fkua/Rsup M.Jamil PadangDokumen22 halamanMitral Valve Repair: DR - Juli Ismail SPB - SPBTKV Bagian Bedah Fkua/Rsup M.Jamil PadangNova SuryatiBelum ada peringkat
- Ijcri 1056610201566 AbdelreheemDokumen6 halamanIjcri 1056610201566 AbdelreheemNova SuryatiBelum ada peringkat
- Idiopathic Normal Pressure Hydrocephalus: A Review For General PractitionersDokumen6 halamanIdiopathic Normal Pressure Hydrocephalus: A Review For General PractitionersNova SuryatiBelum ada peringkat
- Miringitis BulosaDokumen1 halamanMiringitis BulosaNova SuryatiBelum ada peringkat
- TutorialDokumen13 halamanTutorialNova SuryatiBelum ada peringkat
- "Labor and Delivery": Joserizal Serudji Bag/SMF OBGIN FK Unand/RS. M.Djamil PadangDokumen34 halaman"Labor and Delivery": Joserizal Serudji Bag/SMF OBGIN FK Unand/RS. M.Djamil PadangNova SuryatiBelum ada peringkat
- Jurnal VariselaDokumen7 halamanJurnal VariselaNova SuryatiBelum ada peringkat
- Infeksi Jamur OportunistikDokumen27 halamanInfeksi Jamur OportunistikNova SuryatiBelum ada peringkat
- Jurnal Varisela ZosterDokumen19 halamanJurnal Varisela ZosterNova SuryatiBelum ada peringkat
- Bartholinitis: DiagnosisDokumen11 halamanBartholinitis: DiagnosisNova SuryatiBelum ada peringkat
- Fungsi Mata Dan KulitDokumen4 halamanFungsi Mata Dan KulitNova SuryatiBelum ada peringkat
- Gangguan NutrisiDokumen8 halamanGangguan NutrisiNova SuryatiBelum ada peringkat
- Pleno MG 5Dokumen13 halamanPleno MG 5Nova SuryatiBelum ada peringkat
- DGFGHDokumen4 halamanDGFGHKaur AnjandeepBelum ada peringkat
- Effect of Single-Dose Antibiotic Prophylaxis Versus Conventional Antibiotic Therapy in Surgery A Randomized Controlled Trial in A Public Teaching HospitalDokumen5 halamanEffect of Single-Dose Antibiotic Prophylaxis Versus Conventional Antibiotic Therapy in Surgery A Randomized Controlled Trial in A Public Teaching HospitalكنBelum ada peringkat
- 21 CFR 558.15 "Studies": A Brief History: Jeffrey M. Gilbert, PH.DDokumen24 halaman21 CFR 558.15 "Studies": A Brief History: Jeffrey M. Gilbert, PH.Drosebelle1906Belum ada peringkat
- ) The Right Answer: Instructions:-Q.1 A. Multiple Choice Questions - 10 X 1 10Dokumen2 halaman) The Right Answer: Instructions:-Q.1 A. Multiple Choice Questions - 10 X 1 10swapnil goyalBelum ada peringkat
- Spain, Towards A Pig Factory Farm Nation?Dokumen6 halamanSpain, Towards A Pig Factory Farm Nation?Food and Water WatchBelum ada peringkat
- 2006 4266b1!01!03 Ketek Briefing DocumentDokumen186 halaman2006 4266b1!01!03 Ketek Briefing Documentbmartindoyle6396Belum ada peringkat
- Evaluation of Bacterial Agents Isolated From Aspirate Cultures of Covid 19 General Intensivecare Patients Compared To Pre Pandemic ConditionsDokumen8 halamanEvaluation of Bacterial Agents Isolated From Aspirate Cultures of Covid 19 General Intensivecare Patients Compared To Pre Pandemic ConditionsRicardo ZúñigaBelum ada peringkat
- Thyfoid FeverDokumen31 halamanThyfoid FeverTommy Prasetyo AliBelum ada peringkat
- 2016 Cap by PsmidDokumen26 halaman2016 Cap by PsmidBaeyonce MDBelum ada peringkat
- Present Advancement in The Diagnosis and Treatment of Typhoid FeverDokumen7 halamanPresent Advancement in The Diagnosis and Treatment of Typhoid Feverelsa_imamBelum ada peringkat
- TROLOLOLOLOLOLOLOLOLOLOLOLOLOLOLOLDokumen171 halamanTROLOLOLOLOLOLOLOLOLOLOLOLOLOLOLOLpritpal40Belum ada peringkat
- Updated IDSA - ATS Guidelines On Management of Adults With HAP and VAPDokumen11 halamanUpdated IDSA - ATS Guidelines On Management of Adults With HAP and VAPr dwiandiniBelum ada peringkat
- Kebijakan Ab, Formularium IkaDokumen26 halamanKebijakan Ab, Formularium IkaValentina PangayomanBelum ada peringkat
- Aus Pi TargocidDokumen5 halamanAus Pi TargocidAsto Ata InteristiBelum ada peringkat
- Isolation and Antibacterial Activity of Terpenoid From: Available Online atDokumen4 halamanIsolation and Antibacterial Activity of Terpenoid From: Available Online atDeni PratamaBelum ada peringkat
- Pharmacology - Antibiotics - Cell Wall & Membrane Inhibit...Dokumen2 halamanPharmacology - Antibiotics - Cell Wall & Membrane Inhibit...Saurabh Singh RajputBelum ada peringkat
- Biology of Nutrition in Growing AnimalsDokumen599 halamanBiology of Nutrition in Growing AnimalsSam Rafael Bravo GutierrezBelum ada peringkat
- MCQsDokumen12 halamanMCQs54momoBelum ada peringkat
- Inhibitory Activity of Aloe Vera Gel On Some Clinically Isolated Cariogenic and Periodontopathic BacteriaDokumen7 halamanInhibitory Activity of Aloe Vera Gel On Some Clinically Isolated Cariogenic and Periodontopathic BacteriaMarstaRavitriBelum ada peringkat
- Microbiology Lecture - 04 AntibioticsDokumen72 halamanMicrobiology Lecture - 04 AntibioticsChris Queiklin100% (1)
- AntibioticsDokumen7 halamanAntibioticsRahmania Eka SagitaBelum ada peringkat
- Pleurotus FloridaDokumen5 halamanPleurotus FloridaDewiScintaBelum ada peringkat
- Antibiotic Resistance in Diabetic Foot Soft Tissue Infections: A Series From GreeceDokumen5 halamanAntibiotic Resistance in Diabetic Foot Soft Tissue Infections: A Series From GreeceBelinda AngelBelum ada peringkat