Anda mungkin juga menyukai
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (894)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (587)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (119)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2219)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (73)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- MEASLES PresentationDokumen29 halamanMEASLES PresentationMobin Ur Rehman Khan100% (3)
- Introduction and Neoplasia - PathologyDokumen20 halamanIntroduction and Neoplasia - PathologyjmosserBelum ada peringkat
- Osce SuturingDokumen3 halamanOsce Suturingdaniel ragonjanBelum ada peringkat
- Perineal Length Norms in Gravid Women in The First Stage of LabourDokumen4 halamanPerineal Length Norms in Gravid Women in The First Stage of LabourFadil Hidayat100% (1)
- Perineal Outcome After Restrictive Use of Episiotomy in Primi-GravidasDokumen5 halamanPerineal Outcome After Restrictive Use of Episiotomy in Primi-GravidasFadil HidayatBelum ada peringkat
- Liver Disease in Pregnancy: DR Amita Suneja Professor, OB & GYN Ucms & GTBHDokumen22 halamanLiver Disease in Pregnancy: DR Amita Suneja Professor, OB & GYN Ucms & GTBHFadil HidayatBelum ada peringkat
- Jama Septic ShockDokumen2 halamanJama Septic ShockFadil HidayatBelum ada peringkat
- Anthropological and Biological Perspectives of LaborDokumen1 halamanAnthropological and Biological Perspectives of LaborFadil HidayatBelum ada peringkat
- Anatomi Abdomen FinalDokumen55 halamanAnatomi Abdomen FinalFadil HidayatBelum ada peringkat
- Liverdiseaseinpregnancy 2Dokumen40 halamanLiverdiseaseinpregnancy 2Fadil HidayatBelum ada peringkat
- TB PelvisDokumen3 halamanTB PelvisFadil HidayatBelum ada peringkat
- Anatomi Abdomen FinalDokumen55 halamanAnatomi Abdomen FinalFadil HidayatBelum ada peringkat
- JR 2 FadilDokumen14 halamanJR 2 FadilFadil HidayatBelum ada peringkat
- HLHsDokumen3 halamanHLHsFadil HidayatBelum ada peringkat
- Committee Opinion No 620 Salpingectomy For.53Dokumen3 halamanCommittee Opinion No 620 Salpingectomy For.53Muhammad RamadhanBelum ada peringkat
- Cardio To C OgraphyDokumen11 halamanCardio To C OgraphyFadil HidayatBelum ada peringkat
- Spermatogenesis ExplainedDokumen10 halamanSpermatogenesis ExplainedFadil HidayatBelum ada peringkat
- Immune Response ExplainedDokumen34 halamanImmune Response ExplainedAtanas NaydenovBelum ada peringkat
- Pacifc MMI Application Form PDFDokumen6 halamanPacifc MMI Application Form PDFKaitaMahnBelum ada peringkat
- ICOPHAI Abstract Book 2017Dokumen131 halamanICOPHAI Abstract Book 2017Omar TalhaBelum ada peringkat
- 08 - Chapter 4 PDFDokumen197 halaman08 - Chapter 4 PDFkeshav shishyaBelum ada peringkat
- Actinomycosis, Tuberculosis, Leprosy, Syphilis, NomaDokumen37 halamanActinomycosis, Tuberculosis, Leprosy, Syphilis, NomaAroosha MasoodBelum ada peringkat
- Nursing Care for High-Risk Pregnancies Due to Pre-Existing ConditionsDokumen31 halamanNursing Care for High-Risk Pregnancies Due to Pre-Existing Conditionsallanrnmanaloto100% (2)
- Soal Bhs Inggris 1 PerbaikanDokumen7 halamanSoal Bhs Inggris 1 PerbaikanNurul LailiBelum ada peringkat
- Causes RothmanDokumen6 halamanCauses RothmanSamuel Andrés AriasBelum ada peringkat
- Aseptic TechniqueDokumen34 halamanAseptic TechniqueJessa Adenig100% (1)
- Population Knowledge, Attitude, and Practice Regarding Helicobacter Pylori Transmission and OutcomesDokumen6 halamanPopulation Knowledge, Attitude, and Practice Regarding Helicobacter Pylori Transmission and OutcomesBernardo CBBelum ada peringkat
- Takushige Retreat J LSTRDokumen5 halamanTakushige Retreat J LSTRPascalis Adhi KurniawanBelum ada peringkat
- 35 Sources Showing The COVID19 - Corona Virus Is Over Hyped, and Likely Fraud. - RevealingFraud - Com (By Jason Hommel)Dokumen64 halaman35 Sources Showing The COVID19 - Corona Virus Is Over Hyped, and Likely Fraud. - RevealingFraud - Com (By Jason Hommel)DMDOBelum ada peringkat
- Referat PsoriasisDokumen10 halamanReferat PsoriasisAyu AriestaBelum ada peringkat
- Antibacterilal Therapy of MastitisDokumen8 halamanAntibacterilal Therapy of MastitisSunilBelum ada peringkat
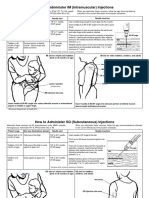
- Im SQ Admin PDFDokumen2 halamanIm SQ Admin PDFAlvin JjBelum ada peringkat
- Adult HIV Notes On GuidelinesDokumen423 halamanAdult HIV Notes On GuidelinesJokerBelum ada peringkat
- Department of Genetics: Covid-19 RT PCRDokumen1 halamanDepartment of Genetics: Covid-19 RT PCRSahil AnsariBelum ada peringkat
- Amoxicillin Tri Hydrate Table FormatDokumen2 halamanAmoxicillin Tri Hydrate Table FormatNico DonatoBelum ada peringkat
- Neonatal Sepsis Case 2Dokumen81 halamanNeonatal Sepsis Case 2Joanne Bernadette Aguilar100% (1)
- E. faecalis Endodontic ChallengeDokumen5 halamanE. faecalis Endodontic ChallengeMonica RoopChanderBelum ada peringkat
- Crp-DikonversiDokumen13 halamanCrp-DikonversiKurnia FitriasariBelum ada peringkat
- Introduction To NeuroimagingDokumen11 halamanIntroduction To NeuroimagingJojo LastBelum ada peringkat
- ToxoplasmosisDokumen7 halamanToxoplasmosisEgha Ratu EdoBelum ada peringkat
- Review: Macrophage Activation Syndrome in Adults: Recent Advances in Pathophysiology, Diagnosis and TreatmentDokumen13 halamanReview: Macrophage Activation Syndrome in Adults: Recent Advances in Pathophysiology, Diagnosis and TreatmentSilvia Leticia BrunoBelum ada peringkat
- Sars-Cov-2 (Covid 19) Detection (Qualitative) by Real Time RT PCRDokumen3 halamanSars-Cov-2 (Covid 19) Detection (Qualitative) by Real Time RT PCRVedant KarnatakBelum ada peringkat
- Ap Biology CH 19 Reading GuideDokumen4 halamanAp Biology CH 19 Reading Guideapi-293174360Belum ada peringkat