Anda mungkin juga menyukai
- FR dISLOKASI BAHUDokumen39 halamanFR dISLOKASI BAHUnurul azizaBelum ada peringkat
- Joint DislocationsDokumen64 halamanJoint DislocationsSabrina Indri WardaniBelum ada peringkat
- 15 - Common Shoulder DisordersDokumen70 halaman15 - Common Shoulder DisordersSyafaringga Dian oscarBelum ada peringkat
- Fractures and Dislocations of The Upper LimbDokumen57 halamanFractures and Dislocations of The Upper Limbمعتز فرعون100% (2)
- Shoulder PainDokumen6 halamanShoulder Painjrice003Belum ada peringkat
- Fracture Pelvis, Hip DislocationsDokumen34 halamanFracture Pelvis, Hip DislocationsMisoBelum ada peringkat
- 12 - Fractures & Dislocations of The Upper Limb-1Dokumen84 halaman12 - Fractures & Dislocations of The Upper Limb-1Ain Ul NoorBelum ada peringkat
- Lecture 7 Upper Limb FracturesDokumen43 halamanLecture 7 Upper Limb Fracturesmukhtar abddiBelum ada peringkat
- Evaluation and Treatment of Common Musculoskeletal Disorder of The ShoulderDokumen42 halamanEvaluation and Treatment of Common Musculoskeletal Disorder of The ShoulderhdthhhhBelum ada peringkat
- Shoulder Dislocation: Orthopedics Department DR Kilian K.KDokumen32 halamanShoulder Dislocation: Orthopedics Department DR Kilian K.KInnocentBelum ada peringkat
- 8.8.2017 - Fracture of FemurDokumen57 halaman8.8.2017 - Fracture of FemurUlfa Sari Al-BahmiBelum ada peringkat
- Fractures of Spine and Pelvis2007Dokumen70 halamanFractures of Spine and Pelvis2007api-19916399Belum ada peringkat
- PBL 1 - Rotator CuffDokumen11 halamanPBL 1 - Rotator CuffEmmanuel Saka100% (1)
- 14-Clinical Notes of ULDokumen54 halaman14-Clinical Notes of ULAmimul EhsanBelum ada peringkat
- Shoulder and HumerusDokumen75 halamanShoulder and HumerusIka HarikartiBelum ada peringkat
- Affections of The KneeDokumen92 halamanAffections of The KneeJudy Ann Bahom SantiagoBelum ada peringkat
- Shoulder Trauma Fractures and Dislocations-Orthoinfo - AaosDokumen6 halamanShoulder Trauma Fractures and Dislocations-Orthoinfo - Aaosapi-228773845Belum ada peringkat
- Dislokasi Panggul & BahuDokumen42 halamanDislokasi Panggul & BahuAnton TrihartantoBelum ada peringkat
- Shoulder Dislocation: DR Saseendar SDokumen55 halamanShoulder Dislocation: DR Saseendar SPankaj VatsaBelum ada peringkat
- Treatment of Femur FracturesDokumen55 halamanTreatment of Femur FracturesMabvuto BandaBelum ada peringkat
- S.S. Medical College Rewa & Associated G.M.H & SGM Hospital, Rewa (M.P.)Dokumen47 halamanS.S. Medical College Rewa & Associated G.M.H & SGM Hospital, Rewa (M.P.)Chrysi TsiouriBelum ada peringkat
- Trauma Medulla SpinalisDokumen79 halamanTrauma Medulla SpinalisiqiqiqiqiqBelum ada peringkat
- Thoracolumbarfractures 150817055817 Lva1 App6891Dokumen75 halamanThoracolumbarfractures 150817055817 Lva1 App6891Pap PipBelum ada peringkat
- Dislocations: Diagnosis, Management, and Complications: Marvin H. Meyers, M.D.Dokumen12 halamanDislocations: Diagnosis, Management, and Complications: Marvin H. Meyers, M.D.Unoscientris StupaBelum ada peringkat
- Shoulder Joint AssessmentDokumen92 halamanShoulder Joint Assessmentsonali tushamerBelum ada peringkat
- BTCLS Trauma SpineDokumen25 halamanBTCLS Trauma SpinePuji NurjanahBelum ada peringkat
- Shoulder DislocationDokumen27 halamanShoulder DislocationReza SyahrialBelum ada peringkat
- Shoulder - LectureDokumen82 halamanShoulder - LectureElizabethBelum ada peringkat
- AnatomyDokumen22 halamanAnatomygggghcBelum ada peringkat
- Supracondylar Fracture HumerusDokumen14 halamanSupracondylar Fracture HumerusFardan AnsarBelum ada peringkat
- Fractures and Dislocations of The Upper Limb IIDokumen90 halamanFractures and Dislocations of The Upper Limb IIatikah_jamilBelum ada peringkat
- 6a. Anatomi Dan Biomekanik Trauma Tulang BelakangDokumen53 halaman6a. Anatomi Dan Biomekanik Trauma Tulang BelakangnurwajdainiBelum ada peringkat
- William C. Cottrell, MD AbstractDokumen4 halamanWilliam C. Cottrell, MD AbstractmalaBelum ada peringkat
- Initial ManagementDokumen2 halamanInitial ManagementVictor ChanBelum ada peringkat
- Femur Leg FracturesDokumen78 halamanFemur Leg FracturesAnonymous hTivgzixVNBelum ada peringkat
- The First Affiliated Hospital of Zhengzhou UniversityDokumen42 halamanThe First Affiliated Hospital of Zhengzhou Universityapi-19916399Belum ada peringkat
- Ortho Review 1Dokumen67 halamanOrtho Review 1mark tBelum ada peringkat
- Department of Orthopaedics & Traumatology, Osmania General Hospital, HydDokumen54 halamanDepartment of Orthopaedics & Traumatology, Osmania General Hospital, HydKolipaka VenkataswamyBelum ada peringkat
- The Shoulder: M.K. SastryDokumen37 halamanThe Shoulder: M.K. SastryGugus EkaBelum ada peringkat
- Surgical Treatment of Neglected Malunion of Shaft Femur: Case ReportDokumen13 halamanSurgical Treatment of Neglected Malunion of Shaft Femur: Case ReportNando OktariBelum ada peringkat
- Facultad de Medicina Humana Y Ciencias de La Salud Escuela Profesional de Tecnologia MédicaDokumen10 halamanFacultad de Medicina Humana Y Ciencias de La Salud Escuela Profesional de Tecnologia MédicaTati LobonBelum ada peringkat
- TrunkDokumen86 halamanTrunkdr_asalehBelum ada peringkat
- Upper Extremity FracturesDokumen80 halamanUpper Extremity FracturesSidan EmozieBelum ada peringkat
- Kamars RadiologyDokumen135 halamanKamars RadiologyNayantara Nair100% (1)
- Musculoskeletal Disorders of Elbow, Wrist and HandsDokumen59 halamanMusculoskeletal Disorders of Elbow, Wrist and Handssaroj yadavBelum ada peringkat
- Femoral Nerve: Riddhi Shroff Shruti Shah SybpthDokumen25 halamanFemoral Nerve: Riddhi Shroff Shruti Shah SybpthNithin NairBelum ada peringkat
- Clinical Anatomy of Upper Limb Joints and MusclesDokumen92 halamanClinical Anatomy of Upper Limb Joints and Musclesgechanatomy100% (1)
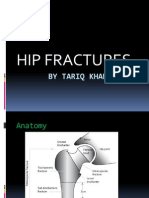
- Hip Fractures: by Tariq KhanDokumen42 halamanHip Fractures: by Tariq KhanKamran Khan KhalilBelum ada peringkat
- Fraktur Humerus EnglishDokumen12 halamanFraktur Humerus EnglishAzizah Mutiara RosdianiBelum ada peringkat
- Spinal Cord InjuryDokumen9 halamanSpinal Cord Injuryta CBelum ada peringkat
- Blue Writing Is What I Added To These Notes: RadiographyDokumen46 halamanBlue Writing Is What I Added To These Notes: Radiographybjpalmer100% (2)
- Orthopedics Notes for Medical StudentsDari EverandOrthopedics Notes for Medical StudentsPenilaian: 4.5 dari 5 bintang4.5/5 (3)
- Materi Kuliah FK ULM 2022 - Lower Extremity I - Hip & KneeDokumen61 halamanMateri Kuliah FK ULM 2022 - Lower Extremity I - Hip & Kneezaki ridhoniBelum ada peringkat
- Upper Extremity FracturesDokumen50 halamanUpper Extremity FracturesClexBelum ada peringkat
- ShoulderDokumen64 halamanShoulderrojansoltanianBelum ada peringkat
- Spinal Cord Injury AlexiDokumen41 halamanSpinal Cord Injury AlexiRoberto AlexiBelum ada peringkat
- Elbow WristDokumen59 halamanElbow Wristdr_asalehBelum ada peringkat
- Elbow Dislocation: DR Ajith John KDokumen53 halamanElbow Dislocation: DR Ajith John KPankaj VatsaBelum ada peringkat
- Bone TumorsDokumen62 halamanBone TumorsEvan Permana PutraBelum ada peringkat
- Ocular TraumaDokumen109 halamanOcular TraumaEvan Permana PutraBelum ada peringkat
- Oxygen DeliveryDokumen10 halamanOxygen DeliveryEvan Permana PutraBelum ada peringkat
- Ocular TraumaDokumen109 halamanOcular TraumaEvan Permana PutraBelum ada peringkat
- SssDokumen5 halamanSssEvan Permana PutraBelum ada peringkat
- Retinal Detachment PDFDokumen8 halamanRetinal Detachment PDFEvan Permana PutraBelum ada peringkat
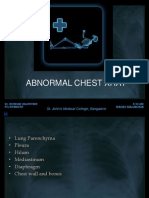
- Abnormal Chest X RayDokumen127 halamanAbnormal Chest X RayEvan Permana PutraBelum ada peringkat
- Assessment of Vestibular SystemDokumen31 halamanAssessment of Vestibular SystemEvan Permana Putra100% (1)
- Kalender Siklus Dokter MudaDokumen1 halamanKalender Siklus Dokter MudaEvan Permana PutraBelum ada peringkat
- Exercise MethodDokumen13 halamanExercise MethodEvan Permana PutraBelum ada peringkat
- Marker KankerDokumen1 halamanMarker KankerEvan Permana PutraBelum ada peringkat
- RenalstonesDokumen13 halamanRenalstonesEvan Permana PutraBelum ada peringkat
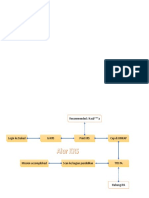
- Alur KRSDokumen2 halamanAlur KRSEvan PermanaBelum ada peringkat
- Natural History and Spectrum of DiseaseDokumen34 halamanNatural History and Spectrum of DiseaseEvan Permana Putra100% (1)
- Ophthalmology AlgorithmsDokumen5 halamanOphthalmology AlgorithmsEvan Permana PutraBelum ada peringkat
- Estimating RiskDokumen47 halamanEstimating RiskEvan Permana PutraBelum ada peringkat
- ATP III Guideline KolesterolDokumen6 halamanATP III Guideline KolesterolRakasiwi GalihBelum ada peringkat
- Models of Health Behavior: DR Yusuf Abdu MisauDokumen80 halamanModels of Health Behavior: DR Yusuf Abdu MisauEvan Permana PutraBelum ada peringkat
- Treating Sepsis - The Latest EvidenceDokumen1 halamanTreating Sepsis - The Latest EvidenceEvan Permana PutraBelum ada peringkat
- Guideline ADA 2010 in Hyperglicemia CrisisDokumen9 halamanGuideline ADA 2010 in Hyperglicemia CrisisAissyiyah Nur An NisaBelum ada peringkat
- Genogram SymbolsDokumen7 halamanGenogram SymbolsBenor AmRi MustaqimBelum ada peringkat
- Diagnosis and Management of Red EyeDokumen8 halamanDiagnosis and Management of Red EyeNelly AstikaBelum ada peringkat
- Sepsis Dan Syok SepsisDokumen13 halamanSepsis Dan Syok SepsisEvan Permana PutraBelum ada peringkat
- Swollen Red Eyelid PDFDokumen10 halamanSwollen Red Eyelid PDFEvan Permana PutraBelum ada peringkat
- DepresiDokumen6 halamanDepresiEvan Permana PutraBelum ada peringkat
- Investigation of Outbreak 2Dokumen54 halamanInvestigation of Outbreak 2Evan Permana PutraBelum ada peringkat
- Simbol GenogramDokumen1 halamanSimbol GenogramEvan Permana Putra100% (4)
- EpistaxisDokumen7 halamanEpistaxisapi-3728652100% (4)
- Epidemic CurveDokumen24 halamanEpidemic CurveEvan Permana Putra50% (2)
- Epidemic CurveDokumen24 halamanEpidemic CurveEvan Permana Putra100% (1)
- Grade 3 Cot Filipino Pandiwa q4Dokumen9 halamanGrade 3 Cot Filipino Pandiwa q4Maricar FaralaBelum ada peringkat
- NCP Impaired Skin IntegrityDokumen2 halamanNCP Impaired Skin IntegrityLiza Marie Cayetano Adarne93% (14)
- Ebook Emergency Radiology The Requisites PDF Full Chapter PDFDokumen67 halamanEbook Emergency Radiology The Requisites PDF Full Chapter PDFrobert.prinz849100% (22)
- Sodium Azide SopDokumen13 halamanSodium Azide SopIndu BarwalBelum ada peringkat
- Evaluating Long Bone Fractures in Children A BiomechanicalDokumen20 halamanEvaluating Long Bone Fractures in Children A BiomechanicalIlma Kurnia SariBelum ada peringkat
- How To Write A Story Final PDFDokumen3 halamanHow To Write A Story Final PDFBárbara SymmesBelum ada peringkat
- Nuero - Brain HerniationDokumen87 halamanNuero - Brain Herniationapi-19916399Belum ada peringkat
- NASS GuidebookDokumen30 halamanNASS Guidebooksheel1Belum ada peringkat
- Materi Dr. Tjhin Sun Fu SP.B M.BiomedDokumen41 halamanMateri Dr. Tjhin Sun Fu SP.B M.BiomedSteven HerbertBelum ada peringkat
- Cervical Radiculopathy Part 1 - Clinical Presentation - Rayner & Smale PDFDokumen9 halamanCervical Radiculopathy Part 1 - Clinical Presentation - Rayner & Smale PDFItai IzhakBelum ada peringkat
- Letter of ApologyDokumen2 halamanLetter of ApologyLaura DorobanțuBelum ada peringkat
- Lower Limb: Muscle Charts: Cheat Sheet (Latin Terminology)Dokumen9 halamanLower Limb: Muscle Charts: Cheat Sheet (Latin Terminology)ali reza khatibiBelum ada peringkat
- RESEARCH THESIS (IZAZ Khan)Dokumen51 halamanRESEARCH THESIS (IZAZ Khan)Izaz KhanBelum ada peringkat
- Manual Muscle TestingDokumen29 halamanManual Muscle TestingImran Ghafoor67% (6)
- The Rover - Part 5 Melchester Rovers 2016/17 SeasonDokumen24 halamanThe Rover - Part 5 Melchester Rovers 2016/17 SeasonCyril "Storky" KnightBelum ada peringkat
- Presenter - Dr. Hershdeep SinghDokumen107 halamanPresenter - Dr. Hershdeep Singhdr. harneet100% (1)
- Alcohol Related Harm in India A Fact SheetDokumen6 halamanAlcohol Related Harm in India A Fact SheetSubrat NandaBelum ada peringkat
- Kundalini Yogafor The Liver, Colon and StomachDokumen4 halamanKundalini Yogafor The Liver, Colon and StomachSandra Costa Bras100% (1)
- Marlin 60 Owners ManualDokumen16 halamanMarlin 60 Owners ManualLeonard Nelson Soliz Vega100% (1)
- Chest X-Ray (CXR) Interpretation 2Dokumen30 halamanChest X-Ray (CXR) Interpretation 2NaveedBelum ada peringkat
- DOH Approved Herbal MedicineDokumen4 halamanDOH Approved Herbal MedicineFea Marielle Macapayad100% (1)
- Guidelines For Preventing Workplace Violence For Healthcare and Social Service WorkersDokumen60 halamanGuidelines For Preventing Workplace Violence For Healthcare and Social Service WorkersSafety and Health magazineBelum ada peringkat
- NCLEX PN Practice Exam Set I-VDokumen56 halamanNCLEX PN Practice Exam Set I-Vaajo136Belum ada peringkat
- Lecture 9 Obstetrical OperationsDokumen47 halamanLecture 9 Obstetrical OperationsgnpobsBelum ada peringkat
- Maxillofacial RadiologyDokumen59 halamanMaxillofacial RadiologyArya KepakisanBelum ada peringkat
- Effect of Knee Position On Hip and Knee Torques.1Dokumen5 halamanEffect of Knee Position On Hip and Knee Torques.1Caerulea Accipiter StriatusBelum ada peringkat
- 2007 Honda Civic Hatchback Owners Manual (Australian, Type R)Dokumen509 halaman2007 Honda Civic Hatchback Owners Manual (Australian, Type R)pblazevski_1100% (3)
- ACAS II Bulletin 12 - Focus On Pilot TrainingDokumen4 halamanACAS II Bulletin 12 - Focus On Pilot TrainingguineasorinBelum ada peringkat
- Nice Sugar StudyDokumen12 halamanNice Sugar StudydociturriagaBelum ada peringkat
- Tehnik Balut MembalutDokumen24 halamanTehnik Balut MembalutmelisandrianaBelum ada peringkat