Anda mungkin juga menyukai
- Notification Central Bank of India Faculty PostsDokumen9 halamanNotification Central Bank of India Faculty PostsRohitRajakBelum ada peringkat
- Official Notification For Union Bank of India RecruitmentDokumen22 halamanOfficial Notification For Union Bank of India RecruitmentKabya SrivastavaBelum ada peringkat
- Instructions APDCL Asst Junior Manager PostsDokumen2 halamanInstructions APDCL Asst Junior Manager PostsRohitRajakBelum ada peringkat
- Notification NPCC Site Engineer PostsDokumen5 halamanNotification NPCC Site Engineer PostsRohitRajakBelum ada peringkat
- Notification HPSCB JR Clerk PostsDokumen7 halamanNotification HPSCB JR Clerk PostsRohitRajakBelum ada peringkat
- Notification CICR YP I PostsDokumen1 halamanNotification CICR YP I PostsRohitRajakBelum ada peringkat
- Recruitment Civil Electrcial Fire EngineersDokumen12 halamanRecruitment Civil Electrcial Fire EngineersPraneeta KatdareBelum ada peringkat
- Notification NRCSS RA PostsDokumen4 halamanNotification NRCSS RA PostsRohitRajakBelum ada peringkat
- Notification Central Bank of India Faculty PostsDokumen9 halamanNotification Central Bank of India Faculty PostsRohitRajakBelum ada peringkat
- Notification PNB Part Time Medical Consultant PostsDokumen2 halamanNotification PNB Part Time Medical Consultant PostsRohitRajakBelum ada peringkat
- Notification IIT Delhi Project Asst Jr. Proj Attendent PostsDokumen1 halamanNotification IIT Delhi Project Asst Jr. Proj Attendent PostsRohitRajakBelum ada peringkat
- Notification IIT Bhubaneswar JRF PostsDokumen1 halamanNotification IIT Bhubaneswar JRF PostsRohitRajakBelum ada peringkat
- Notification NCERT Computer Asst PostsDokumen1 halamanNotification NCERT Computer Asst PostsRohitRajakBelum ada peringkat
- Notification AIC of India Administrative Officer PostsDokumen19 halamanNotification AIC of India Administrative Officer PostsRohitRajakBelum ada peringkat
- Notification SCTIMST Medico Social Worker PostsDokumen1 halamanNotification SCTIMST Medico Social Worker PostsRohitRajakBelum ada peringkat
- Notification DRDO LASTEC JRF PostsDokumen3 halamanNotification DRDO LASTEC JRF PostsRohitRajakBelum ada peringkat
- Notification PNB Part Time Medical Consultant PostsDokumen2 halamanNotification PNB Part Time Medical Consultant PostsRohitRajakBelum ada peringkat
- Notification Lok Nayak Hospital SR Resident PostsDokumen3 halamanNotification Lok Nayak Hospital SR Resident PostsRohitRajakBelum ada peringkat
- Notification West Central Railway Sports Person PostsDokumen9 halamanNotification West Central Railway Sports Person PostsRohitRajakBelum ada peringkat
- Nainitaal Bank RecruitentDokumen10 halamanNainitaal Bank RecruitentkabyaBelum ada peringkat
- Notification SCTIMST Apprentice PostsDokumen1 halamanNotification SCTIMST Apprentice PostsRohitRajakBelum ada peringkat
- Notification Judicial Department WB Non Official Marriage Officer PostsDokumen3 halamanNotification Judicial Department WB Non Official Marriage Officer PostsRohitRajakBelum ada peringkat
- Notification IIT Bhubaneswar Project Assistant PostsDokumen1 halamanNotification IIT Bhubaneswar Project Assistant PostsRohitRajakBelum ada peringkat
- Notification DRDO LASTEC JRF PostsDokumen3 halamanNotification DRDO LASTEC JRF PostsRohitRajakBelum ada peringkat
- Notification ONGC Director Finance PostsDokumen5 halamanNotification ONGC Director Finance PostsRohitRajakBelum ada peringkat
- Notification PNRD Assam Accredited Eng Computer Asst Other PostsDokumen2 halamanNotification PNRD Assam Accredited Eng Computer Asst Other PostsRohitRajakBelum ada peringkat
- Notification JIPMER Statistician PostsDokumen2 halamanNotification JIPMER Statistician PostsRohitRajakBelum ada peringkat
- Notification CIPET JRF PostsDokumen1 halamanNotification CIPET JRF PostsRohitRajakBelum ada peringkat
- Notification Oriental Insurance Company LTD Administrative Officer PostsDokumen28 halamanNotification Oriental Insurance Company LTD Administrative Officer PostsRohitRajakBelum ada peringkat
- Notification Kerala University Senior Research Fellow PostsDokumen1 halamanNotification Kerala University Senior Research Fellow PostsRohitRajakBelum ada peringkat
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (399)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (73)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (120)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- Gender and Human SexualityDokumen1 halamanGender and Human SexualitygosmileyBelum ada peringkat
- Topic: The Global Interstate System Exercise 2: The Most Talked About IssuesDokumen2 halamanTopic: The Global Interstate System Exercise 2: The Most Talked About IssuesDanica Jane RamosBelum ada peringkat
- Exercise 3 Predator Prey EcologyDokumen2 halamanExercise 3 Predator Prey EcologyRenielle RebadomiaBelum ada peringkat
- A Guide To The Linguistic and Stylistic Analysis of A Passage From ChaucerDokumen3 halamanA Guide To The Linguistic and Stylistic Analysis of A Passage From ChaucerNasrullah AliBelum ada peringkat
- Analisis Beban Kerja Mental Mahasiswa Saat PerkuliDokumen8 halamanAnalisis Beban Kerja Mental Mahasiswa Saat PerkuliAdiyatma Ghazian PratamaBelum ada peringkat
- Overweight Students of GANHS SHS On The Efficacy of The Ketogenic Diet"Dokumen2 halamanOverweight Students of GANHS SHS On The Efficacy of The Ketogenic Diet"Red Meigen ImportanteBelum ada peringkat
- DyslexiaDokumen10 halamanDyslexiaapi-710612589Belum ada peringkat
- International Journal of Organizational InnovationFinal Issue Vol 6 Num 3 January 2014Dokumen225 halamanInternational Journal of Organizational InnovationFinal Issue Vol 6 Num 3 January 2014Vinit DawaneBelum ada peringkat
- Harrah's Case QuestionsDokumen8 halamanHarrah's Case QuestionsAhad Tanveer100% (2)
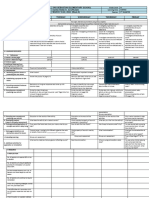
- Science 4 Q3 W8 DLLDokumen3 halamanScience 4 Q3 W8 DLLDiana Rose AcupeadoBelum ada peringkat
- Grade 7 Exam 9 PDFDokumen16 halamanGrade 7 Exam 9 PDFShane Rajapaksha100% (2)
- QSEV Introduction Final RAHDokumen29 halamanQSEV Introduction Final RAHPrapti SuraniBelum ada peringkat
- MCT 3423Dokumen6 halamanMCT 3423abdio89Belum ada peringkat
- Manifesta Journal 7Dokumen65 halamanManifesta Journal 7David Ayala AlfonsoBelum ada peringkat
- Stroke MistakesDokumen10 halamanStroke Mistakeschitra selviBelum ada peringkat
- Soalan Interview EnglishDokumen7 halamanSoalan Interview EnglishzanwahidBelum ada peringkat
- Checkpoint Past Paper 2 2015 PDFDokumen10 halamanCheckpoint Past Paper 2 2015 PDFShafia N0% (2)
- Caritas in Veritate: A Reflection PaperDokumen2 halamanCaritas in Veritate: A Reflection PaperMarbert PinqueBelum ada peringkat
- ARRANGED HEALTH - PEACE.VALUES Catch Up FridaysDokumen44 halamanARRANGED HEALTH - PEACE.VALUES Catch Up FridaysVegilla Sinlao Ann Jeeh100% (1)
- 3 New Literacies, 21st Century SkillsDokumen66 halaman3 New Literacies, 21st Century Skillsirene apiladaBelum ada peringkat
- Johns Hopkins University PHD DissertationDokumen5 halamanJohns Hopkins University PHD DissertationWriteMyCustomPaperUK100% (1)
- Pre-Con-Form - Mirasol A. RosalesDokumen2 halamanPre-Con-Form - Mirasol A. RosalesMirasol RosalesBelum ada peringkat
- Bee PPT Sem 2Dokumen14 halamanBee PPT Sem 2Divya ZopeBelum ada peringkat
- Language AttitudesDokumen18 halamanLanguage AttitudesScholar WinterflameBelum ada peringkat
- The Morning Calm Korea Weekly - June 24, 2005Dokumen26 halamanThe Morning Calm Korea Weekly - June 24, 2005Morning Calm Weekly NewspaperBelum ada peringkat
- Thinking From A To ZDokumen165 halamanThinking From A To ZadrianaBelum ada peringkat
- Cedric VillaniDokumen18 halamanCedric VillaniJe Suis TuBelum ada peringkat
- Research PaperDokumen40 halamanResearch PaperBENEDICT FRANZ ALMERIABelum ada peringkat
- IacmDokumen3 halamanIacmmanendra_shuklaBelum ada peringkat
- Broadcasting WorkshopDokumen9 halamanBroadcasting WorkshopRyan De la TorreBelum ada peringkat