Anda mungkin juga menyukai
- Nomination Form CHED IQuAME AssessorDokumen4 halamanNomination Form CHED IQuAME Assessorramilsanchez@yahoo.comBelum ada peringkat
- Position Applied For:: Employment Data FormDokumen4 halamanPosition Applied For:: Employment Data FormNilesh BendaleBelum ada peringkat
- Application FormDokumen5 halamanApplication FormboyleBelum ada peringkat
- Mdt-Job Application FormDokumen8 halamanMdt-Job Application Formpuspa paramithaBelum ada peringkat
- Matura, Marry Joy A.: Cell Phone #: - Email AddressDokumen1 halamanMatura, Marry Joy A.: Cell Phone #: - Email AddressJude Thaddeus EstoquiaBelum ada peringkat
- Application SampleDokumen1 halamanApplication SamplenageenBelum ada peringkat
- Buitems Incubation FormDokumen3 halamanBuitems Incubation FormSheryar ShakirBelum ada peringkat
- Policy Employee Grievance and Complaint Procedure FormDokumen1 halamanPolicy Employee Grievance and Complaint Procedure FormLagare EndBelum ada peringkat
- Eteeap Application FormDokumen6 halamanEteeap Application FormsumaychengBelum ada peringkat
- Eteeap Application Form Pangasinan State UDokumen1 halamanEteeap Application Form Pangasinan State UMarcial Jr. MilitanteBelum ada peringkat
- Stpi 3ApplicationTvm1Dokumen2 halamanStpi 3ApplicationTvm1Chetan SehgalBelum ada peringkat
- Application FormDokumen5 halamanApplication FormboyleBelum ada peringkat
- IIETM Application FormDokumen8 halamanIIETM Application FormPaarBelum ada peringkat
- Departmental PermissionDokumen1 halamanDepartmental PermissionIbrahim Mohmand100% (2)
- Job Application FormDokumen3 halamanJob Application Formsupri0% (1)
- Bio-Data Sheet of 6thDokumen2 halamanBio-Data Sheet of 6thTazim HossanBelum ada peringkat
- Jose RizalDokumen8 halamanJose RizalAica Rose Dela CruzBelum ada peringkat
- FEBC Info Sheet - NEWDokumen5 halamanFEBC Info Sheet - NEWnigel alinsug0% (1)
- CPPN Group Affiliation FormDokumen2 halamanCPPN Group Affiliation Formapi-264638229Belum ada peringkat
- Sample HR Forms Dhir & Partners 2021Dokumen26 halamanSample HR Forms Dhir & Partners 2021myszeykaBelum ada peringkat
- Employee Profile Form of EbacoDokumen2 halamanEmployee Profile Form of EbacoAniket GunjalBelum ada peringkat
- SEED Application FormDokumen4 halamanSEED Application FormTeasha Nika PetersBelum ada peringkat
- Bio DataDokumen3 halamanBio DataVhellery CorpuzBelum ada peringkat
- Employee Personal Profile Format 1Dokumen8 halamanEmployee Personal Profile Format 1Alpesh Patel50% (2)
- Application Form For Edsp For RegionsDokumen4 halamanApplication Form For Edsp For RegionsPagodBelum ada peringkat
- Karnatak Law SocietyDokumen2 halamanKarnatak Law Societyaftabshaikh04Belum ada peringkat
- FDDC Resource Member ApplicationDokumen6 halamanFDDC Resource Member ApplicationLarryPradaBelum ada peringkat
- AEP Form Region IVDokumen1 halamanAEP Form Region IVAllan YdiaBelum ada peringkat
- TugasDokumen4 halamanTugasbimawiguna16Belum ada peringkat
- Position Applied For I. Personal Identity: Pas FotoDokumen4 halamanPosition Applied For I. Personal Identity: Pas Fototri188Belum ada peringkat
- Application Form 2021 - KossanDokumen4 halamanApplication Form 2021 - KossanBoxaer ItiusBelum ada peringkat
- Vishwa Bharati Public School: Grams: VishwabhartiDokumen4 halamanVishwa Bharati Public School: Grams: Vishwabhartimittal_y2kBelum ada peringkat
- Wilderness North Summer Staff ApplicationDokumen4 halamanWilderness North Summer Staff ApplicationtentmakersofficeBelum ada peringkat
- Immersion HandbookDokumen15 halamanImmersion HandbookALMIRA PEGADBelum ada peringkat
- Employment Applicant FormDokumen2 halamanEmployment Applicant Formyasmin izzatiBelum ada peringkat
- CPS Intake FormDokumen4 halamanCPS Intake FormKathleen DearingerBelum ada peringkat
- Form BiodataDokumen3 halamanForm BiodataZain Az-zuhriBelum ada peringkat
- Sample HR FormDokumen4 halamanSample HR FormJesstoni CaniedoBelum ada peringkat
- JAC Delhi - Certificate For Pysically DisabledDokumen1 halamanJAC Delhi - Certificate For Pysically DisabledAnweshaBoseBelum ada peringkat
- Personnel Profile TemplateDokumen2 halamanPersonnel Profile TemplatezylfielBelum ada peringkat
- M SDP Job ApplicationformDokumen4 halamanM SDP Job ApplicationformSajjad AbbasiBelum ada peringkat
- Application FormDokumen4 halamanApplication Formchandra kusumaBelum ada peringkat
- AA - Application FormDokumen2 halamanAA - Application Formlagan2008Belum ada peringkat
- Employment Application Form ISODokumen6 halamanEmployment Application Form ISOAjay IyerBelum ada peringkat
- ATS Joining KitDokumen25 halamanATS Joining Kitmukeshkushwah01031993Belum ada peringkat
- Application Form V3 Jan 2022Dokumen4 halamanApplication Form V3 Jan 2022IT Gunungmas GroupBelum ada peringkat
- Systems AnalystDokumen2 halamanSystems Analystsandeep_nagar29Belum ada peringkat
- Job Application FormDokumen1 halamanJob Application FormApple AimanBelum ada peringkat
- 1x1 ID Photo: Insurance CommissionDokumen1 halaman1x1 ID Photo: Insurance CommissionBryan MagnayeBelum ada peringkat
- Department of Education: Background Investigation FormDokumen3 halamanDepartment of Education: Background Investigation FormAilyn Guindolan100% (2)
- Job Application Form (New Member Join)Dokumen2 halamanJob Application Form (New Member Join)Pinochio MonstaBelum ada peringkat
- Completete SET OF HR FORMSDokumen9 halamanCompletete SET OF HR FORMSALEXANDER DIMAFELIX JR.Belum ada peringkat
- QR 2.1-1-3-c Job Application FormDokumen3 halamanQR 2.1-1-3-c Job Application FormMochammad Aji HutamaBelum ada peringkat
- Copyofresumedevelopementorganizer RomeciolucateroDokumen3 halamanCopyofresumedevelopementorganizer Romeciolucateroapi-342008502Belum ada peringkat
- Dav Fertilizer Public School, Babrala: (Application Form)Dokumen2 halamanDav Fertilizer Public School, Babrala: (Application Form)Sunil PrasadBelum ada peringkat
- Interview Formats - 2 PagesDokumen2 halamanInterview Formats - 2 Pagespatelpuren36Belum ada peringkat
- Education Division Bio-Data Form422176620191220Dokumen3 halamanEducation Division Bio-Data Form422176620191220Nani VenkeyBelum ada peringkat
- BORANG ITS-biDokumen2 halamanBORANG ITS-biPhilip D'cruzBelum ada peringkat
- Interview Form 20.3.14Dokumen5 halamanInterview Form 20.3.14TanveshBelum ada peringkat
- Rqat CV Form 2010Dokumen2 halamanRqat CV Form 2010ramilsanchez@yahoo.comBelum ada peringkat
- Rqat CV Form 2010Dokumen2 halamanRqat CV Form 2010ramilsanchez@yahoo.comBelum ada peringkat
- CHED FDP Phase 2 Brochure With Forms Dhei and CmoDokumen21 halamanCHED FDP Phase 2 Brochure With Forms Dhei and Cmoramilsanchez@yahoo.com100% (3)
- Tentative Plan CHRDC Draft 1 RevisedDokumen112 halamanTentative Plan CHRDC Draft 1 Revisedramilsanchez@yahoo.comBelum ada peringkat
- Ched Ncae TemplateDokumen2 halamanChed Ncae Templateramilsanchez@yahoo.comBelum ada peringkat
- GPR-4B (To Be Notarized)Dokumen3 halamanGPR-4B (To Be Notarized)ramilsanchez@yahoo.comBelum ada peringkat
- CHED Caraga Survey 2010 - FormDokumen1 halamanCHED Caraga Survey 2010 - Formramilsanchez@yahoo.comBelum ada peringkat
- CV of The Nominee For CHED IQuAME AssessorDokumen3 halamanCV of The Nominee For CHED IQuAME Assessorramilsanchez@yahoo.comBelum ada peringkat
- CHED CMO No. 44 S. 2009Dokumen3 halamanCHED CMO No. 44 S. 2009Coolbuster.NetBelum ada peringkat
- Scholarship Requirements 2009 CHED CaragaDokumen1 halamanScholarship Requirements 2009 CHED Caragaramilsanchez@yahoo.comBelum ada peringkat
- Oss-Ched Scholarship FormDokumen1 halamanOss-Ched Scholarship Formramilsanchez@yahoo.com100% (5)
- CHRDC Proposed Health Research AgendaDokumen18 halamanCHRDC Proposed Health Research Agendaramilsanchez@yahoo.comBelum ada peringkat
- Oss-Ched Scholarship FormDokumen1 halamanOss-Ched Scholarship Formramilsanchez@yahoo.com100% (5)
- CMO 40 s.2008 MOR For Private H.EDokumen59 halamanCMO 40 s.2008 MOR For Private H.Eteng1981100% (22)
- Ched Caraga Hemis Report 2007-2008Dokumen14 halamanChed Caraga Hemis Report 2007-2008ramilsanchez@yahoo.comBelum ada peringkat
- Ched Caraga Hemis Ay 2006-2007Dokumen25 halamanChed Caraga Hemis Ay 2006-2007ramilsanchez@yahoo.comBelum ada peringkat
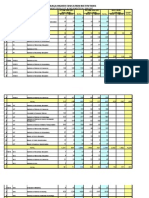
- Gradesheet Computation by RASanchezDokumen4 halamanGradesheet Computation by RASanchezramilsanchez@yahoo.com100% (1)
- Board For Professional Teachers-TOSDokumen107 halamanBoard For Professional Teachers-TOSramilsanchez@yahoo.comBelum ada peringkat
- Draft IP Policy Template As of Aug 26Dokumen24 halamanDraft IP Policy Template As of Aug 26ramilsanchez@yahoo.comBelum ada peringkat
- CHED E-Forms A B-C Institutional, Programs, Enrollment and Graduates For Private HEIs - AY0910Dokumen7 halamanCHED E-Forms A B-C Institutional, Programs, Enrollment and Graduates For Private HEIs - AY0910ramilsanchez@yahoo.com100% (2)
- Instructions For Faculty Form E5 - AY0910Dokumen5 halamanInstructions For Faculty Form E5 - AY0910ramilsanchez@yahoo.com100% (3)
- Tphs - Jpehs.jpenhs Alumni Directory FormDokumen1 halamanTphs - Jpehs.jpenhs Alumni Directory Formramilsanchez@yahoo.comBelum ada peringkat
- RQAT Summary Report W Instruction To HEIDokumen5 halamanRQAT Summary Report W Instruction To HEIramilsanchez@yahoo.com100% (1)
- CHED Form E5 - Faculty Form For Private HEIs - AY0910Dokumen2 halamanCHED Form E5 - Faculty Form For Private HEIs - AY0910ramilsanchez@yahoo.com100% (1)
- Instructions For CHED Forms A-B E-Forms - AY0910Dokumen5 halamanInstructions For CHED Forms A-B E-Forms - AY0910ramilsanchez@yahoo.comBelum ada peringkat
- LKG Math Question Paper: 1. Count and Write The Number in The BoxDokumen6 halamanLKG Math Question Paper: 1. Count and Write The Number in The BoxKunal Naidu60% (5)
- Packet Unit 3 - Atomic Structure-Answers ChemistryDokumen11 halamanPacket Unit 3 - Atomic Structure-Answers ChemistryMario J. KafatiBelum ada peringkat
- Health and Safety For The Meat Industry: Guidance NotesDokumen198 halamanHealth and Safety For The Meat Industry: Guidance NotesPredrag AndjelkovicBelum ada peringkat
- Unit 1 and 2Dokumen4 halamanUnit 1 and 2Aim Rubia100% (1)
- 0 BA Design ENDokumen12 halaman0 BA Design ENFilho AiltonBelum ada peringkat
- Brochure International ConferenceDokumen6 halamanBrochure International ConferenceAnubhav Sharma sf 12Belum ada peringkat
- Avid Final ProjectDokumen2 halamanAvid Final Projectapi-286463817Belum ada peringkat
- Ginger Final Report FIGTF 02Dokumen80 halamanGinger Final Report FIGTF 02Nihmathullah Kalanther Lebbe100% (2)
- Benko Gambit-Jacobs and Kinsman, 1999Dokumen163 halamanBenko Gambit-Jacobs and Kinsman, 1999johnson Greker100% (3)
- Product Specifications Product Specifications: LLPX411F LLPX411F - 00 - V1 V1Dokumen4 halamanProduct Specifications Product Specifications: LLPX411F LLPX411F - 00 - V1 V1David MooneyBelum ada peringkat
- Historical Exchange Rates - OANDA AUD-MYRDokumen1 halamanHistorical Exchange Rates - OANDA AUD-MYRML MLBelum ada peringkat
- 100 20210811 ICOPH 2021 Abstract BookDokumen186 halaman100 20210811 ICOPH 2021 Abstract Bookwafiq alibabaBelum ada peringkat
- Stewart, Mary - The Little BroomstickDokumen159 halamanStewart, Mary - The Little BroomstickYunon100% (1)
- Conveyor Control Using Programmable Logic ControllerDokumen7 halamanConveyor Control Using Programmable Logic ControllerWann RexroBelum ada peringkat
- Applied Physics (PHY-102) Course OutlineDokumen3 halamanApplied Physics (PHY-102) Course OutlineMuhammad RafayBelum ada peringkat
- Onset Hobo Trade T Cdi 5200 5400 User ManualDokumen3 halamanOnset Hobo Trade T Cdi 5200 5400 User Manualpaull20020% (1)
- Object-Oriented Design Patterns in The Kernel, Part 2 (LWN - Net)Dokumen15 halamanObject-Oriented Design Patterns in The Kernel, Part 2 (LWN - Net)Rishabh MalikBelum ada peringkat
- Why File A Ucc1Dokumen10 halamanWhy File A Ucc1kbarn389100% (4)
- Elastomeric Impression MaterialsDokumen6 halamanElastomeric Impression MaterialsMarlene CasayuranBelum ada peringkat
- Formal Letter LPDokumen2 halamanFormal Letter LPLow Eng Han100% (1)
- Pt. Trijaya Agro FoodsDokumen18 halamanPt. Trijaya Agro FoodsJie MaBelum ada peringkat
- Internship ReportDokumen36 halamanInternship ReportM.IMRAN0% (1)
- Geotechnical Aspects of Open Stope Design at BHP Cannington: G C StreetonDokumen7 halamanGeotechnical Aspects of Open Stope Design at BHP Cannington: G C StreetonJuan PerezBelum ada peringkat
- Code ExplanantionDokumen4 halamanCode ExplanantionVivek JadiyaBelum ada peringkat
- Building A Pentesting Lab For Wireless Networks - Sample ChapterDokumen29 halamanBuilding A Pentesting Lab For Wireless Networks - Sample ChapterPackt PublishingBelum ada peringkat
- Internet Bill FormatDokumen1 halamanInternet Bill FormatGopal Singh100% (1)
- Morse Potential CurveDokumen9 halamanMorse Potential Curvejagabandhu_patraBelum ada peringkat
- CL RouterAndSwitches AE Kn1of3 AnswerDokumen19 halamanCL RouterAndSwitches AE Kn1of3 Answereugene ngBelum ada peringkat
- IG Deck Seal PumpDokumen3 halamanIG Deck Seal PumpSergei KurpishBelum ada peringkat
- International Patient Referral - Part 2 - Revised - 29-04-2010 - 2Dokumen2 halamanInternational Patient Referral - Part 2 - Revised - 29-04-2010 - 2Fatah AssadBelum ada peringkat