Anda mungkin juga menyukai
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (890)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (587)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (119)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2219)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (265)
- Principles of Pharmacology - The Pathophysiologic Basis of Drug TherapyDokumen978 halamanPrinciples of Pharmacology - The Pathophysiologic Basis of Drug TherapyAvarvarei Moisa Raluca80% (5)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (73)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- Cigarette Smoking Increases Lung Cancer Risk by 9xDokumen4 halamanCigarette Smoking Increases Lung Cancer Risk by 9xMarc FosterBelum ada peringkat
- Oet StudyDokumen36 halamanOet StudyFatima Zehra Nishad89% (35)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- PREPARE ME: A DIFFERENT PERSPECTIVE ON END-OF-LIFE CAREDokumen5 halamanPREPARE ME: A DIFFERENT PERSPECTIVE ON END-OF-LIFE CARERazaCreciaLastrillaMeneses100% (1)
- Oncology NursingDokumen10 halamanOncology NursingMhaii Ameril88% (8)
- 47 PG 125Dokumen1 halaman47 PG 125sandman6548Belum ada peringkat
- Mosbys Medical Dictionary - 9E (PDF) (UnitedVRG)Dokumen1.986 halamanMosbys Medical Dictionary - 9E (PDF) (UnitedVRG)Avarvarei Moisa RalucaBelum ada peringkat
- DP Advanced PDFDokumen1 halamanDP Advanced PDFAvarvarei Moisa RalucaBelum ada peringkat
- CV Moisa MadalinDokumen1 halamanCV Moisa MadalinAvarvarei Moisa RalucaBelum ada peringkat
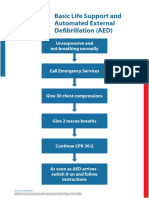
- Poster BLS Algorithm ENG V20151005 HRES SiteDokumen1 halamanPoster BLS Algorithm ENG V20151005 HRES SiteAvarvarei Moisa RalucaBelum ada peringkat
- DP Advanced PDFDokumen1 halamanDP Advanced PDFAvarvarei Moisa RalucaBelum ada peringkat
- Astmul BronsicDokumen90 halamanAstmul BronsicAvarvarei Moisa RalucaBelum ada peringkat
- Exam 2Dokumen5 halamanExam 2Avarvarei Moisa RalucaBelum ada peringkat
- Chartpilot 9330Dokumen8 halamanChartpilot 9330Avarvarei Moisa RalucaBelum ada peringkat
- Poster ALS Algorithm ENG V20151005 HRES SiteDokumen1 halamanPoster ALS Algorithm ENG V20151005 HRES SiteCosmina Alina MoscuBelum ada peringkat
- Poster SpecCircs Anaphylaxis Treatment Algorithm ENG V20151001 HRES Site PDFDokumen1 halamanPoster SpecCircs Anaphylaxis Treatment Algorithm ENG V20151001 HRES Site PDFPetrarkina LauraBelum ada peringkat
- Exam 1Dokumen6 halamanExam 1Avarvarei Moisa RalucaBelum ada peringkat
- DP Advanced PDFDokumen1 halamanDP Advanced PDFAvarvarei Moisa RalucaBelum ada peringkat
- ORAR - 2016-2017 - Semestrul II: Medicină - Anul V - Seria ADokumen1 halamanORAR - 2016-2017 - Semestrul II: Medicină - Anul V - Seria AadelinaBelum ada peringkat
- Sclerodermie Sistemica20161102001850448Dokumen31 halamanSclerodermie Sistemica20161102001850448Avarvarei Moisa RalucaBelum ada peringkat
- Cancer Rect Si Parologie PerianalaDokumen8 halamanCancer Rect Si Parologie PerianalaAvarvarei Moisa RalucaBelum ada peringkat
- APL Form Rhodos Moisa MadalinDokumen3 halamanAPL Form Rhodos Moisa MadalinAvarvarei Moisa RalucaBelum ada peringkat
- New Doc 2017-03-26Dokumen2 halamanNew Doc 2017-03-26Avarvarei Moisa RalucaBelum ada peringkat
- New Doc 2017-03-26 PDFDokumen2 halamanNew Doc 2017-03-26 PDFAvarvarei Moisa RalucaBelum ada peringkat
- CamScanner Document ScansDokumen80 halamanCamScanner Document ScansAvarvarei Moisa RalucaBelum ada peringkat
- Apendicita AcDokumen6 halamanApendicita AcAvarvarei Moisa RalucaBelum ada peringkat
- Toto Stomac Plus BilaDokumen24 halamanToto Stomac Plus BilaAvarvarei Moisa RalucaBelum ada peringkat
- New Doc 2017-02-27 PDFDokumen9 halamanNew Doc 2017-02-27 PDFAvarvarei Moisa RalucaBelum ada peringkat
- Fisa TBCDokumen22 halamanFisa TBCAvarvarei Moisa RalucaBelum ada peringkat
- Tae-Bo and Tabata Workout Schedule for Weeks I and IIDokumen2 halamanTae-Bo and Tabata Workout Schedule for Weeks I and IIAvarvarei Moisa RalucaBelum ada peringkat
- CamScanner Scans PDFs from PhotosDokumen9 halamanCamScanner Scans PDFs from PhotosAvarvarei Moisa RalucaBelum ada peringkat
- Traumatisme andDokumen6 halamanTraumatisme andAvarvarei Moisa RalucaBelum ada peringkat
- Pancr Ac CR Cancer Pamcr CHH Icter MecDokumen17 halamanPancr Ac CR Cancer Pamcr CHH Icter MecAvarvarei Moisa RalucaBelum ada peringkat
- Tu 2016 5711031582 6107 4725Dokumen138 halamanTu 2016 5711031582 6107 4725Jack WongBelum ada peringkat
- Oxygenation NotesDokumen23 halamanOxygenation NoteschikaycBelum ada peringkat
- Sree Chitra Tirunal Institute Course CurriculumsDokumen55 halamanSree Chitra Tirunal Institute Course Curriculumsfindingnemo667Belum ada peringkat
- ONCOLOGY MCQS PREPARATION FOR 5th Yr MBBSDokumen21 halamanONCOLOGY MCQS PREPARATION FOR 5th Yr MBBSDrRaghavender Reddy100% (12)
- Vaigai College of EngineeringDokumen3 halamanVaigai College of EngineeringBARANIDHARAN VBelum ada peringkat
- 1 PBDokumen8 halaman1 PBdeepak dashBelum ada peringkat
- Chest Surgery DelhiDokumen3 halamanChest Surgery DelhiAnonymous OrzzzvmnnDBelum ada peringkat
- Carlos M. Mery & Joseph W. Turek - TSRA Review of Cardiothoracic SurgeryDokumen371 halamanCarlos M. Mery & Joseph W. Turek - TSRA Review of Cardiothoracic SurgeryShawn Robinson100% (1)
- 楊志仁 肺結核與腫瘤判讀Dokumen109 halaman楊志仁 肺結核與腫瘤判讀au angelBelum ada peringkat
- Special Pathology Viva Questions by AMS 46Dokumen32 halamanSpecial Pathology Viva Questions by AMS 46Mohan Dass100% (1)
- Tobacco Smoking-Associated Alterations in The Immune Microenvironment of Squamous Cell CarcinomasDokumen7 halamanTobacco Smoking-Associated Alterations in The Immune Microenvironment of Squamous Cell CarcinomasKamado NezukoBelum ada peringkat
- Lung Cancer PathoDokumen5 halamanLung Cancer PathoMahlonee LinBelum ada peringkat
- Gen. and Systemic Pathology Course Description & Lab. Manual Vol. 2 (AY 2021-2022) - Protected43Dokumen245 halamanGen. and Systemic Pathology Course Description & Lab. Manual Vol. 2 (AY 2021-2022) - Protected43Drashti kamodiaBelum ada peringkat
- Dr. Handoko T, SPP: Sub Departemen Penyakit Paru Dan AlergiDokumen54 halamanDr. Handoko T, SPP: Sub Departemen Penyakit Paru Dan AlergiMUHAMMAD BAGIR ALJUFRIBelum ada peringkat
- Michael S. Niederman Severe Pneumonia Lung Biology in Health and Disease, Volume 206Dokumen450 halamanMichael S. Niederman Severe Pneumonia Lung Biology in Health and Disease, Volume 206Alirio Bastidas0% (1)
- Lung Cancer Epidemiology Etiology and PreventionDokumen41 halamanLung Cancer Epidemiology Etiology and Preventiontonirian99Belum ada peringkat
- MBChB Year 4 & 5 Past Papers + Answers for Respiratory, Gastrointestinal, Neurology and MoreDokumen172 halamanMBChB Year 4 & 5 Past Papers + Answers for Respiratory, Gastrointestinal, Neurology and MoreHariharan NarendranBelum ada peringkat
- Rodriguez Canales2016Dokumen22 halamanRodriguez Canales2016Triaprasetya HadiBelum ada peringkat
- SmokingDokumen198 halamanSmokingRoman Ash100% (2)
- Lung Tumors: Dr. Mohammed Natiq Pulmonary PathologyDokumen4 halamanLung Tumors: Dr. Mohammed Natiq Pulmonary PathologyNoor AL Deen SabahBelum ada peringkat
- The National Commission On Marihuana and Drug Abuse - 1972 NixonDokumen473 halamanThe National Commission On Marihuana and Drug Abuse - 1972 NixonJames LindonBelum ada peringkat
- Cancer and Climate ChangeDokumen9 halamanCancer and Climate ChangeRicardo VegaBelum ada peringkat
- Nursing Care Plan: Western Mindanao State University College of NursingDokumen11 halamanNursing Care Plan: Western Mindanao State University College of NursingPatricia VasquezBelum ada peringkat
- What Is A LobectomyDokumen6 halamanWhat Is A LobectomyMaria Carmela TormesBelum ada peringkat
- Jurnal Stigma Kanker Paru PDFDokumen16 halamanJurnal Stigma Kanker Paru PDFsri subektiBelum ada peringkat
- Diagnostic Imaging and Procedures for Respiratory DiseaseDokumen41 halamanDiagnostic Imaging and Procedures for Respiratory DiseaseVio Mincu100% (1)