Anda mungkin juga menyukai
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5795)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (74)
- MSM Sulphur For HealthDokumen7 halamanMSM Sulphur For HealthMasterOfHotGlass100% (1)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- MAPEH 9 TOS 1st GradingDokumen4 halamanMAPEH 9 TOS 1st Gradingelyn50% (2)
- The Preparation of The True Sulphur of AntimonyDokumen20 halamanThe Preparation of The True Sulphur of AntimonyAlex BellBelum ada peringkat
- Diabetes Mellitus Overview LayDokumen17 halamanDiabetes Mellitus Overview LaychelitvaleramdBelum ada peringkat
- Downstream ProcessingDokumen45 halamanDownstream ProcessingRelyboy de Fiesta100% (2)
- NCP GastroenteritisDokumen1 halamanNCP GastroenteritisFranchesca PaunganBelum ada peringkat
- Board 4-CHNDokumen30 halamanBoard 4-CHNKira100% (22)
- TB Case PresDokumen5 halamanTB Case PresAlwina May Parojinog BarlisanBelum ada peringkat
- Constipation With Scylabous Stools, Intermittent: IncreasedDokumen1 halamanConstipation With Scylabous Stools, Intermittent: IncreasedAlwina May Parojinog BarlisanBelum ada peringkat
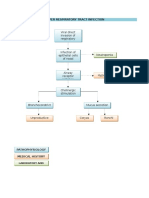
- Pathophysiology of Upper Respiratory Tract InfectionDokumen1 halamanPathophysiology of Upper Respiratory Tract InfectionAlwina May Parojinog BarlisanBelum ada peringkat
- Skin Grafts and Skin SubstitutesDokumen5 halamanSkin Grafts and Skin SubstitutesAlwina May Parojinog BarlisanBelum ada peringkat
- AoW 9 Sugar OverloadDokumen2 halamanAoW 9 Sugar OverloadkristymadimikeBelum ada peringkat
- Amrit Bindu A4 Display PosterDokumen1 halamanAmrit Bindu A4 Display PostersdoctorBelum ada peringkat
- Questions of The AnthraxDokumen4 halamanQuestions of The AnthraxJosé Luis RaymundoBelum ada peringkat
- Common Health Problems of Infancy PowptDokumen78 halamanCommon Health Problems of Infancy PowptCiella Dela CruzBelum ada peringkat
- Haad QuestionDokumen20 halamanHaad QuestionNimraj PatelBelum ada peringkat
- An Approach To Small Bowel ObstructionDokumen3 halamanAn Approach To Small Bowel ObstructionHardik JeenaBelum ada peringkat
- Nipah Virus PDFDokumen2 halamanNipah Virus PDFRakesh SahuBelum ada peringkat
- Biers BlockDokumen4 halamanBiers Blockemkay1234Belum ada peringkat
- Grade 5 Term 4 Life Skills Lesson Plan Name of Lesson: Become A Disease Detective!Dokumen3 halamanGrade 5 Term 4 Life Skills Lesson Plan Name of Lesson: Become A Disease Detective!Raeesa SBelum ada peringkat
- KalingaDLL-scientific Literacy & Critical ThinkingDokumen4 halamanKalingaDLL-scientific Literacy & Critical ThinkingMary Joy Lucob TangbawanBelum ada peringkat
- Respiratory SystemDokumen16 halamanRespiratory Systemapi-277775953Belum ada peringkat
- Lactational Mastitis Puerperal 2020Dokumen12 halamanLactational Mastitis Puerperal 2020bgBelum ada peringkat
- Panadeine: What Is in This LeafletDokumen3 halamanPanadeine: What Is in This Leafletradzi66Belum ada peringkat
- Guarantee: Life Insurance Fortune PlusDokumen14 halamanGuarantee: Life Insurance Fortune PlusvijayBelum ada peringkat
- CTG Interpretation of CTG and CFHM During Antepartum and Intrapartum Periods Ho Lai FongDokumen33 halamanCTG Interpretation of CTG and CFHM During Antepartum and Intrapartum Periods Ho Lai FongSabrina AzizBelum ada peringkat
- Spinal Exercise Home ProgrammeDokumen19 halamanSpinal Exercise Home ProgrammePrabha VetrichelvanBelum ada peringkat
- Orbit (Kankis)Dokumen42 halamanOrbit (Kankis)Jel JelitaaaBelum ada peringkat
- ABC Imaging 1 - The SpineDokumen145 halamanABC Imaging 1 - The SpineAna-Maria PaunescuBelum ada peringkat
- JKMJKDokumen5 halamanJKMJKSuci IrianiBelum ada peringkat
- Evolution of NeonatologyDokumen17 halamanEvolution of NeonatologyClaudia KosztelnikBelum ada peringkat
- Prosthodontic DiagnosisDokumen15 halamanProsthodontic DiagnosisYashpreetsingh Bhatia100% (1)
- Antenatal CareDokumen50 halamanAntenatal CareHari HardanaBelum ada peringkat
- SGD 3 Case ProtocolDokumen2 halamanSGD 3 Case ProtocolJulie Ann TrinidadBelum ada peringkat