Anda mungkin juga menyukai
- 1995 S320 S420 S500 Owner's Manual Edition C PDFDokumen153 halaman1995 S320 S420 S500 Owner's Manual Edition C PDFnpachecorecabarrenBelum ada peringkat
- Obesity in Children & AdolescentsDokumen14 halamanObesity in Children & AdolescentsAvif PutraBelum ada peringkat
- Excel NotesDokumen9 halamanExcel NotesAhnBelum ada peringkat
- Resumo: Artigos Originais / Original ArticlesDokumen7 halamanResumo: Artigos Originais / Original ArticlesRafael SedlmaierBelum ada peringkat
- Obese Lotas Brief 2010Dokumen4 halamanObese Lotas Brief 2010bbmantapBelum ada peringkat
- Sanja Obes ResDokumen11 halamanSanja Obes Resrc513Belum ada peringkat
- QoL Obese ChildrenDokumen7 halamanQoL Obese ChildrenLiga Sabatina de BaloncestoBelum ada peringkat
- AAP Committee On Nutrition-Pediatrics. 2003 112Dokumen9 halamanAAP Committee On Nutrition-Pediatrics. 2003 112Rang PasamanBelum ada peringkat
- Childhood Obesity and ComorbiditiesDokumen7 halamanChildhood Obesity and Comorbiditiesapi-260548731Belum ada peringkat
- Woobaidal 2016Dokumen19 halamanWoobaidal 2016Visa LaserBelum ada peringkat
- Obesidad InfantilDokumen13 halamanObesidad InfantilBrenda Anali Pariona NapaBelum ada peringkat
- Factors Aff GrowthDokumen3 halamanFactors Aff GrowthgratianusbBelum ada peringkat
- Obesidad en PreescolaresDokumen8 halamanObesidad en PreescolaresSebastian Ernesto Siegmund SanhuezaBelum ada peringkat
- Prevalence and Risk Factors For Obesity and Overweight Among Elementarystudents at West Visayas State University - Integrated Laboratory School in 2013Dokumen53 halamanPrevalence and Risk Factors For Obesity and Overweight Among Elementarystudents at West Visayas State University - Integrated Laboratory School in 2013Bryan AtasBelum ada peringkat
- Understanding The CauseDokumen1 halamanUnderstanding The CauseMay Dianne Mansia BautistaBelum ada peringkat
- Maternal and Child Undernutrition 2: SeriesDokumen18 halamanMaternal and Child Undernutrition 2: SeriesBudirmanBelum ada peringkat
- Running Head: Review of Literature in Childhood Obesity 1Dokumen7 halamanRunning Head: Review of Literature in Childhood Obesity 1Gibbs MiguelBelum ada peringkat
- Nutritional Status of Grade Pupils of San Roque Elementary School San Jacinto, PangasinanDokumen39 halamanNutritional Status of Grade Pupils of San Roque Elementary School San Jacinto, PangasinanmharicharBelum ada peringkat
- Flavio Art2art08 PDFDokumen7 halamanFlavio Art2art08 PDFAngie EspinozaBelum ada peringkat
- Obesity in Children & Adolescents: Review ArticleDokumen11 halamanObesity in Children & Adolescents: Review ArticleMatt QBelum ada peringkat
- Review Article: Need For Early Interventions in The Prevention of Pediatric Overweight: A Review and Upcoming DirectionsDokumen18 halamanReview Article: Need For Early Interventions in The Prevention of Pediatric Overweight: A Review and Upcoming DirectionsIsabel ReyBelum ada peringkat
- Research ProposalDokumen17 halamanResearch Proposalapi-297065332Belum ada peringkat
- EnglishDokumen9 halamanEnglishapi-245723352Belum ada peringkat
- Childhood Obesity2Dokumen4 halamanChildhood Obesity2noraisa sapilinBelum ada peringkat
- 6 UN Reddy EtalDokumen6 halaman6 UN Reddy EtaleditorijmrhsBelum ada peringkat
- Literature Review On Causes of Childhood ObesityDokumen4 halamanLiterature Review On Causes of Childhood Obesityjsmyxkvkg100% (1)
- Literature Review Article On Childhood ObesityDokumen8 halamanLiterature Review Article On Childhood Obesityc5qvf1q1100% (1)
- Early Childhood Caries and Body Mass Index in Young Children From Low Income FamiliesDokumen12 halamanEarly Childhood Caries and Body Mass Index in Young Children From Low Income FamiliesAmandeep ChopraBelum ada peringkat
- Articulo para LeerDokumen8 halamanArticulo para LeerMarianaBelum ada peringkat
- HS390 Group6 ResearchDokumen6 halamanHS390 Group6 Researchjoseyalm2323Belum ada peringkat
- Assessment of Nutritional Status of Children in Al Hilla CityDokumen8 halamanAssessment of Nutritional Status of Children in Al Hilla CityKamruzzaman ManikBelum ada peringkat
- Literature Review FinalDokumen11 halamanLiterature Review Finalapi-253949835Belum ada peringkat
- Pediatric Obesity and Gallstone Disease.18Dokumen6 halamanPediatric Obesity and Gallstone Disease.18Merari Lugo OcañaBelum ada peringkat
- 06 Original 02Dokumen7 halaman06 Original 02normanahmad92Belum ada peringkat
- Obesity and Physical Activity Literature ReviewDokumen5 halamanObesity and Physical Activity Literature Reviewea8d1b6n100% (1)
- Obesity Is The Most Nutritional Among Children Developed CountriesDokumen14 halamanObesity Is The Most Nutritional Among Children Developed CountriesBulanBiruBelum ada peringkat
- Maternal Nutritional AssessmentDokumen7 halamanMaternal Nutritional AssessmentchinchuBelum ada peringkat
- Untitled 1Dokumen8 halamanUntitled 1Sri HariBelum ada peringkat
- J Public Health-2011-Kovalskys-403-11 PDFDokumen9 halamanJ Public Health-2011-Kovalskys-403-11 PDFFlori GeorgianaBelum ada peringkat
- Dillender - Final PaperDokumen7 halamanDillender - Final Paperapi-381502154Belum ada peringkat
- Health 634 e Portfolio 3 Literature ReviewDokumen5 halamanHealth 634 e Portfolio 3 Literature Reviewapi-370740412Belum ada peringkat
- Articless41572 023 00435 4.Pdfpdf Button20stickyDokumen19 halamanArticless41572 023 00435 4.Pdfpdf Button20stickyTabitha MenezesBelum ada peringkat
- Research ReviewDokumen4 halamanResearch ReviewLiikascypherBelum ada peringkat
- Childhood Obesity Research Paper ThesisDokumen5 halamanChildhood Obesity Research Paper ThesisCourtney Esco100% (2)
- Research ArticleDokumen10 halamanResearch Articleindah sundariBelum ada peringkat
- Nutrition and Childhood ObesityDokumen8 halamanNutrition and Childhood ObesityErick MuthengiBelum ada peringkat
- The Normal Anthropometric Measurements For HealthyDokumen43 halamanThe Normal Anthropometric Measurements For HealthyAli Mohamed BurhanBelum ada peringkat
- Article (5) ElcDokumen20 halamanArticle (5) ElcSyaqiraBelum ada peringkat
- Dafonseca 2017Dokumen45 halamanDafonseca 2017visiniBelum ada peringkat
- ID Hubungan Jarak Kelahiran Dan Jumlah AnakDokumen9 halamanID Hubungan Jarak Kelahiran Dan Jumlah AnakfaidinBelum ada peringkat
- Factors Related To Overweight in Kindergarten School ChildrenDokumen6 halamanFactors Related To Overweight in Kindergarten School ChildrenImam Wiro MardoyoBelum ada peringkat
- Keywords:: Go ToDokumen52 halamanKeywords:: Go ToEvaristus Lokuruka EkadeliBelum ada peringkat
- Research Paper - Katie Hawn - 7-31-2012Dokumen18 halamanResearch Paper - Katie Hawn - 7-31-2012api-220705744Belum ada peringkat
- Dinapoli 2011Dokumen8 halamanDinapoli 2011Abid SherazBelum ada peringkat
- Artículo Original: Frecuencia de Sobrepeso y Obesidad Infantil en Un Centro de Salud de Rosario, ArgentinaDokumen4 halamanArtículo Original: Frecuencia de Sobrepeso y Obesidad Infantil en Un Centro de Salud de Rosario, ArgentinaLalolalolalolaBelum ada peringkat
- J. Pediatr. Psychol. 2014 Gowey 552 61Dokumen10 halamanJ. Pediatr. Psychol. 2014 Gowey 552 61Flavia DenisaBelum ada peringkat
- Bete Bo 2017Dokumen18 halamanBete Bo 2017Zemenu AddissBelum ada peringkat
- Obesity in Children and AdolescentsDokumen2 halamanObesity in Children and Adolescentsrenas23Belum ada peringkat
- MainDokumen11 halamanMainanita pratiwiBelum ada peringkat
- Influence of Nutritional Variables and Obesity On Health and MetabolismDokumen10 halamanInfluence of Nutritional Variables and Obesity On Health and MetabolismThaisBelum ada peringkat
- Childhood Obesity: Causes and Consequences, Prevention and Management.Dari EverandChildhood Obesity: Causes and Consequences, Prevention and Management.Belum ada peringkat
- Am J Clin Nutr 2007 Freedman 33 40Dokumen8 halamanAm J Clin Nutr 2007 Freedman 33 40Firaz R AkbarBelum ada peringkat
- TaskForce On Childhood Obesity May2010 FullReport PDFDokumen124 halamanTaskForce On Childhood Obesity May2010 FullReport PDFFiraz R AkbarBelum ada peringkat
- The Rome III Criteria For The Functional GI DisordersDokumen3 halamanThe Rome III Criteria For The Functional GI DisordersFiraz R AkbarBelum ada peringkat
- Daftar Pustaka: Borges, G. Et AlDokumen1 halamanDaftar Pustaka: Borges, G. Et AlFiraz R AkbarBelum ada peringkat
- Bmi Screening Guidelines For Schools PDFDokumen31 halamanBmi Screening Guidelines For Schools PDFFiraz R Akbar100% (1)
- Fiberlogic CarrierEthernet 842 5300 PresentationDokumen41 halamanFiberlogic CarrierEthernet 842 5300 PresentationDuong Thanh Lam0% (1)
- CSC:361-Software Engineering: Semester: Fall2020Dokumen39 halamanCSC:361-Software Engineering: Semester: Fall2020hamsfayyazBelum ada peringkat
- EConsole1 Quick Start Guide ENGDokumen21 halamanEConsole1 Quick Start Guide ENGManuel Casais TajesBelum ada peringkat
- NumpyDokumen23 halamanNumpymuzammil jawedBelum ada peringkat
- Solutionbank D1: Edexcel AS and A Level Modular MathematicsDokumen30 halamanSolutionbank D1: Edexcel AS and A Level Modular MathematicsMaruf_007Belum ada peringkat
- Sympoly Toolbox IssuesDokumen7 halamanSympoly Toolbox IssuesAli FahemBelum ada peringkat
- SR-X Script Reference - EDokumen24 halamanSR-X Script Reference - EDomagoj ZagoracBelum ada peringkat
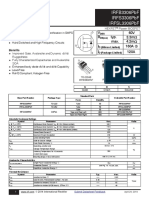
- Irfb3306Pbf Irfs3306Pbf Irfsl3306Pbf: V 60V R Typ. 3.3M: Max. 4.2M I 160A C I 120ADokumen12 halamanIrfb3306Pbf Irfs3306Pbf Irfsl3306Pbf: V 60V R Typ. 3.3M: Max. 4.2M I 160A C I 120ADirson Volmir WilligBelum ada peringkat
- Chapter 16 - Oral Radiography (Essentials of Dental Assisting)Dokumen96 halamanChapter 16 - Oral Radiography (Essentials of Dental Assisting)mussanteBelum ada peringkat
- Test ElectrolysisDokumen3 halamanTest ElectrolysisNatalia WhyteBelum ada peringkat
- Plagiarism - ReportDokumen6 halamanPlagiarism - ReportDipesh NagpalBelum ada peringkat
- Exploring Music ContentsDokumen370 halamanExploring Music ContentsRoby SamboraBelum ada peringkat
- Various Image Enhancement Techniques-A Critical Review: S.S. Bedi, Rati KhandelwalDokumen5 halamanVarious Image Enhancement Techniques-A Critical Review: S.S. Bedi, Rati KhandelwalArina AndriesBelum ada peringkat
- GTG - TFA Belt DrivenDokumen2 halamanGTG - TFA Belt Drivensuan170Belum ada peringkat
- PassivityDokumen15 halamanPassivitySmarties AcademyBelum ada peringkat
- ST7201-Finite Element MethodDokumen14 halamanST7201-Finite Element MethodVishal RanganathanBelum ada peringkat
- EC 201 Network TheoryDokumen2 halamanEC 201 Network TheoryJoseph JohnBelum ada peringkat
- Driver LCI 150W 500-850ma FlexC NF h28 EXC3 enDokumen7 halamanDriver LCI 150W 500-850ma FlexC NF h28 EXC3 enMoustafa HelalyBelum ada peringkat
- PDC NitDokumen6 halamanPDC NitrpshvjuBelum ada peringkat
- DCM-I&II Lab Equipments ListDokumen2 halamanDCM-I&II Lab Equipments ListPrashant ChinamalliBelum ada peringkat
- Edan M3B Vital Signs Monitor User ManualDokumen92 halamanEdan M3B Vital Signs Monitor User ManualJosé marino Franco AlzateBelum ada peringkat
- Week 1 Lesson 1 2nd QuarterDokumen2 halamanWeek 1 Lesson 1 2nd QuarterKristine Jewel MacatiagBelum ada peringkat
- Microcontroller Based Vehicle Security SystemDokumen67 halamanMicrocontroller Based Vehicle Security Systemlokesh_045Belum ada peringkat
- Syllabus EMSE6760 DDLDokumen4 halamanSyllabus EMSE6760 DDLlphiekickmydogBelum ada peringkat
- SPE-183743-MS Maintaining Injectivity of Disposal Wells: From Water Quality To Formation PermeabilityDokumen19 halamanSPE-183743-MS Maintaining Injectivity of Disposal Wells: From Water Quality To Formation PermeabilityAminBelum ada peringkat
- TitleDokumen142 halamanTitleAmar PašićBelum ada peringkat
- Nursing Research Lecture 4aDokumen26 halamanNursing Research Lecture 4asyamsul anwarBelum ada peringkat
- JNJNKDokumen11 halamanJNJNKjatin gargBelum ada peringkat