Anda mungkin juga menyukai
- Predictors of Cognitive Impairment in An Early Stage Parkinson S Disease CohortDokumen9 halamanPredictors of Cognitive Impairment in An Early Stage Parkinson S Disease CohortGeorgiana PrisoschiBelum ada peringkat
- PAPER (ENG) - New Subtype of Spinocerebellar Ataxia With Altered Vertical Eye Movements Mapping To Chromosome 1p32Dokumen9 halamanPAPER (ENG) - New Subtype of Spinocerebellar Ataxia With Altered Vertical Eye Movements Mapping To Chromosome 1p32Aldo Hip NaranjoBelum ada peringkat
- PAPER (ENG) - Cardiovascular Risk Profile and Cognitive Function in Young, Middle-Aged, and Elderly SubjectsDokumen14 halamanPAPER (ENG) - Cardiovascular Risk Profile and Cognitive Function in Young, Middle-Aged, and Elderly SubjectsAldo Hip NaranjoBelum ada peringkat
- PAPER (ENG) - Tracheostomy Decannulation and Cough Peak Flows in Patients With Neuromuscular WeaknessDokumen5 halamanPAPER (ENG) - Tracheostomy Decannulation and Cough Peak Flows in Patients With Neuromuscular WeaknessAldo Hip NaranjoBelum ada peringkat
- PAPER (ENG) - The Coordination of Respiration and Swallowing For Volitional and Reflex Swallows - A Pilot StudyDokumen11 halamanPAPER (ENG) - The Coordination of Respiration and Swallowing For Volitional and Reflex Swallows - A Pilot StudyAldo Hip NaranjoBelum ada peringkat
- PAPER (ENG) - (Alencar M., Et Al., 2012 BRA) Correlation Between Brain Injury and Dysphagia in Adult Patients With StrokeDokumen9 halamanPAPER (ENG) - (Alencar M., Et Al., 2012 BRA) Correlation Between Brain Injury and Dysphagia in Adult Patients With StrokeAldo Hip NaranjoBelum ada peringkat
- PAPER (ENG) - Life-Span Cognitive Activity, Neuropathologic Burden, and Cognitive AgingDokumen8 halamanPAPER (ENG) - Life-Span Cognitive Activity, Neuropathologic Burden, and Cognitive AgingAldo Hip NaranjoBelum ada peringkat
- PAPER (ENG) - Swallowing Dysfunction in Patients Receiving Prolonged Mechanical VentilationDokumen6 halamanPAPER (ENG) - Swallowing Dysfunction in Patients Receiving Prolonged Mechanical VentilationAldo Hip NaranjoBelum ada peringkat
- PAPER (ENG) - The Early Feeding Skills Assessment For Preterm InfantsDokumen15 halamanPAPER (ENG) - The Early Feeding Skills Assessment For Preterm InfantsAldo Hip NaranjoBelum ada peringkat
- Stimulation of sucking and swallowing in preterm infantsDokumen3 halamanStimulation of sucking and swallowing in preterm infantsAldo Hip NaranjoBelum ada peringkat
- PAPER (ENG) - The Safety of FEESST - An Analysis of 500 Consecutive EvaluationsDokumen7 halamanPAPER (ENG) - The Safety of FEESST - An Analysis of 500 Consecutive EvaluationsAldo Hip NaranjoBelum ada peringkat
- PAPER (ENG) - The Dysphagia Outcome and Severity Scale (DOSS Scale)Dokumen8 halamanPAPER (ENG) - The Dysphagia Outcome and Severity Scale (DOSS Scale)Aldo Hip NaranjoBelum ada peringkat
- PAPER (ENG) - New Subtype of Spinocerebellar Ataxia With Altered Vertical Eye Movements Mapping To Chromosome 1p32Dokumen9 halamanPAPER (ENG) - New Subtype of Spinocerebellar Ataxia With Altered Vertical Eye Movements Mapping To Chromosome 1p32Aldo Hip NaranjoBelum ada peringkat
- PAPER (ENG) - The Presentation and Management of Laryngeal Cleft - A 10 Years ExperienceDokumen7 halamanPAPER (ENG) - The Presentation and Management of Laryngeal Cleft - A 10 Years ExperienceAldo Hip NaranjoBelum ada peringkat
- PAPER (ENG) - The Early Impact of Feeding On Infant Breathing-Swallowing CoordinationDokumen7 halamanPAPER (ENG) - The Early Impact of Feeding On Infant Breathing-Swallowing CoordinationAldo Hip NaranjoBelum ada peringkat
- Dysphagia Handicap Index, Development and ValidationDokumen7 halamanDysphagia Handicap Index, Development and ValidationWlf OoBelum ada peringkat
- PAPER (ENG) - Mechanics of Sucking - Comparison Between Bottle Feeding and BreastfeedingDokumen8 halamanPAPER (ENG) - Mechanics of Sucking - Comparison Between Bottle Feeding and BreastfeedingAldo Hip NaranjoBelum ada peringkat
- 6th Central Pay Commission Salary CalculatorDokumen15 halaman6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- PAPER (ENG) - Swallowing Disturbance Questionnaire For Detecting DysphagiaDokumen5 halamanPAPER (ENG) - Swallowing Disturbance Questionnaire For Detecting DysphagiaAldo Hip NaranjoBelum ada peringkat
- PAPER (ENG) - The Accuary of The Modified Evan's Bue Dye Test in Predicting AspirationDokumen5 halamanPAPER (ENG) - The Accuary of The Modified Evan's Bue Dye Test in Predicting AspirationAldo Hip NaranjoBelum ada peringkat
- Jpts 27 3355Dokumen3 halamanJpts 27 3355Gabriel GonzalezBelum ada peringkat
- PAPER (ENG) - Speech-Language Pathologist-Led Fiberoptic Endoscopic Evaluation of Swallowing Functional Outcomes For Patients After StrokeDokumen6 halamanPAPER (ENG) - Speech-Language Pathologist-Led Fiberoptic Endoscopic Evaluation of Swallowing Functional Outcomes For Patients After StrokeAldo Hip NaranjoBelum ada peringkat
- PAPER (ENG) - Relevance of Subcortical Stroke in DysphagiaDokumen6 halamanPAPER (ENG) - Relevance of Subcortical Stroke in DysphagiaAldo Hip NaranjoBelum ada peringkat
- PAPER (ENG) - Swallowing Disorders in Clinical Practice - Funtional Anatomy, Assessment and Rehabilitation StrategiesDokumen7 halamanPAPER (ENG) - Swallowing Disorders in Clinical Practice - Funtional Anatomy, Assessment and Rehabilitation StrategiesAldo Hip NaranjoBelum ada peringkat
- PAPER (ENG) - Screening Test For Silent Aspiration at The BedsideDokumen8 halamanPAPER (ENG) - Screening Test For Silent Aspiration at The BedsideAldo Hip NaranjoBelum ada peringkat
- PAPER (ENG) - Pseudodysphagia Due To Omohyoid Muscle SyndromeDokumen6 halamanPAPER (ENG) - Pseudodysphagia Due To Omohyoid Muscle SyndromeAldo Hip NaranjoBelum ada peringkat
- Measuring Breathing and Swallowing Coordination in Human Infants Using The Kay Elemetrics Swallowing WorkstationDokumen9 halamanMeasuring Breathing and Swallowing Coordination in Human Infants Using The Kay Elemetrics Swallowing WorkstationAldo Hip NaranjoBelum ada peringkat
- PAPER (ENG) - Otolaryngology and Speech Therapy Evaluation in The Assessment of Oropharyngeal Dysphagia - A Combined Protocol ProposalDokumen13 halamanPAPER (ENG) - Otolaryngology and Speech Therapy Evaluation in The Assessment of Oropharyngeal Dysphagia - A Combined Protocol ProposalAldo Hip NaranjoBelum ada peringkat
- PAPER (ENG) - Predictors of Nutritive Sucking in Preterm InfantsDokumen11 halamanPAPER (ENG) - Predictors of Nutritive Sucking in Preterm InfantsAldo Hip NaranjoBelum ada peringkat
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (399)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (890)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (587)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (265)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (72)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2219)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (119)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- Aspergillosis GuideDokumen10 halamanAspergillosis GuideTiza JulyanBelum ada peringkat
- COVID 19 ProjectDokumen4 halamanCOVID 19 ProjectSam SezBelum ada peringkat
- Epidemiology TriangleDokumen1 halamanEpidemiology TriangleMelDred Cajes BolandoBelum ada peringkat
- Mycoplasma and UreaplasmaDokumen17 halamanMycoplasma and UreaplasmaSteph ReyesBelum ada peringkat
- Bipolar Disorder & Depression: Understanding the LinkDokumen17 halamanBipolar Disorder & Depression: Understanding the LinkHasan Ahmed KhanBelum ada peringkat
- FCPS Part 1 Medicine Syllabus FinalDokumen37 halamanFCPS Part 1 Medicine Syllabus FinalMd. Afraem Hossain SeamBelum ada peringkat
- RATHL Trial SummaryDokumen5 halamanRATHL Trial SummaryDr.ImaanBelum ada peringkat
- NCP DiarrheaDokumen2 halamanNCP DiarrheaPrincess Xzmae RamirezBelum ada peringkat
- Progyluton-26 1DDokumen16 halamanProgyluton-26 1DUsma aliBelum ada peringkat
- Pediatrics Slides 23C 2020 8 Banvir 1aDokumen344 halamanPediatrics Slides 23C 2020 8 Banvir 1aBanvir SinghBelum ada peringkat
- September 7/20/21 Letter From Superintendent Brian CoreyDokumen2 halamanSeptember 7/20/21 Letter From Superintendent Brian CoreyNews10NBCBelum ada peringkat
- This Study Resource WasDokumen3 halamanThis Study Resource WasSam CuevasBelum ada peringkat
- The Patient With Recurrent Oral UlcerationDokumen9 halamanThe Patient With Recurrent Oral UlcerationintanBelum ada peringkat
- Acute Respiratory Distress Syndrome (ARDS) Causes, Symptoms, TreatmentDokumen2 halamanAcute Respiratory Distress Syndrome (ARDS) Causes, Symptoms, Treatmentmanish086Belum ada peringkat
- Hi - Precision Diagnostics: Medical ReportDokumen3 halamanHi - Precision Diagnostics: Medical ReportMarie Ann SeraficaBelum ada peringkat
- Natural History of Disease and Levels of Prevention ExplainedDokumen39 halamanNatural History of Disease and Levels of Prevention ExplainedNadine VillaretBelum ada peringkat
- Mental Health Disorders Among TeenagersDokumen1 halamanMental Health Disorders Among TeenagersEᔕTᕼEᖇBelum ada peringkat
- WHO ASEAN Workshop On Priority Actions For Dengue Prevention and CorltrolDokumen35 halamanWHO ASEAN Workshop On Priority Actions For Dengue Prevention and CorltrolIvy joan jomocBelum ada peringkat
- IDSR Checklist PDFDokumen54 halamanIDSR Checklist PDFKen KabaliBelum ada peringkat
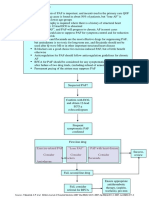
- Pathway DIAGNOSIS OF PAF FTRDokumen1 halamanPathway DIAGNOSIS OF PAF FTRYoan Eka Putra PalilingBelum ada peringkat
- Coronavirus MemoDokumen3 halamanCoronavirus MemoWXXI News100% (2)
- Intro to Shelter Medicine: Segregation, Quarantine, Isolation HousingDokumen29 halamanIntro to Shelter Medicine: Segregation, Quarantine, Isolation HousingChadBelum ada peringkat
- Nejmicm 2116076Dokumen1 halamanNejmicm 2116076Hugo GarciaBelum ada peringkat
- Tugas PKBB Artikel PicotDokumen9 halamanTugas PKBB Artikel PicotEsri DewiBelum ada peringkat
- OCD in Post-Covid EraDokumen47 halamanOCD in Post-Covid EraSaadia TalibBelum ada peringkat
- Active vs Passive Immunity & Vaccination ExplainedDokumen13 halamanActive vs Passive Immunity & Vaccination Explainedsha_man029Belum ada peringkat
- Lung Disease: PneumoniaDokumen2 halamanLung Disease: Pneumoniacayla mae carlosBelum ada peringkat
- Ischaemic Teat Necrosis in Dairy Cattle: LettersDokumen1 halamanIschaemic Teat Necrosis in Dairy Cattle: LetterscsigafiBelum ada peringkat
- AspergillosisDokumen2 halamanAspergillosisRizki RomadaniBelum ada peringkat
- Diseases (Magonjwa)Dokumen3 halamanDiseases (Magonjwa)Divine MuwanguziBelum ada peringkat