Anda mungkin juga menyukai
- Gastric Outlet Obstruction, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsDari EverandGastric Outlet Obstruction, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsBelum ada peringkat
- Pyloric Stenosis GuideDokumen5 halamanPyloric Stenosis GuideMichael AlexanderBelum ada peringkat
- Community Health NursingDokumen4 halamanCommunity Health Nursingd-fbuser-68662439Belum ada peringkat
- Aklan State University Nursing Readings on Pyloric StenosisDokumen5 halamanAklan State University Nursing Readings on Pyloric Stenosisensoooooooooo100% (1)
- Hirschsprung’s Disease, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsDari EverandHirschsprung’s Disease, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsBelum ada peringkat
- Case Study 51Dokumen21 halamanCase Study 51henryrchouinard100% (2)
- Managing Nause and Vomiting-Crit-Care-Nurse-2003-Garrett-31-50 PDFDokumen22 halamanManaging Nause and Vomiting-Crit-Care-Nurse-2003-Garrett-31-50 PDFpmuftiaBelum ada peringkat
- Chronic PyelonephritisDokumen5 halamanChronic PyelonephritisIsak ShatikaBelum ada peringkat
- Basal Metabolic Rate, Calories, Ideal Body WeightDokumen12 halamanBasal Metabolic Rate, Calories, Ideal Body WeightMary Claire ReyesBelum ada peringkat
- ICU Case Study PDFDokumen19 halamanICU Case Study PDFYashvi SinghBelum ada peringkat
- Chronic Liver Disease and CirrhosisDokumen5 halamanChronic Liver Disease and Cirrhosisaqil ithninBelum ada peringkat
- Case Study SurgW FinalDokumen59 halamanCase Study SurgW FinalLovely CacapitBelum ada peringkat
- Pancreatic AdenocarcinomaDokumen6 halamanPancreatic AdenocarcinomafikriafisBelum ada peringkat
- NAFLD - NASH and Present & Future Management OptionsDokumen78 halamanNAFLD - NASH and Present & Future Management OptionsSantosh AnandBelum ada peringkat
- Complicated Utis: Mohammad Amoran M. SampalDokumen11 halamanComplicated Utis: Mohammad Amoran M. SampalMohammad Amoran SampalBelum ada peringkat
- Complementary and Alternative Approach For Pain Management in LabourDokumen9 halamanComplementary and Alternative Approach For Pain Management in LabourPujianti LestarinaBelum ada peringkat
- Systemic Lupus ErythematosusDokumen46 halamanSystemic Lupus ErythematosuspriscillaBelum ada peringkat
- Nutrition & Bio-Chemistry PDFDokumen10 halamanNutrition & Bio-Chemistry PDFRãj Pôtti ÑâîkBelum ada peringkat
- 12G Lab3 GARCIADokumen3 halaman12G Lab3 GARCIARuthangela GarciaBelum ada peringkat
- CHNDokumen12 halamanCHNJhara100% (1)
- Problem With The PassageDokumen3 halamanProblem With The PassageLuiciaBelum ada peringkat
- Transient Tachypnea of The NewbornDokumen6 halamanTransient Tachypnea of The NewbornTarquin TomadaBelum ada peringkat
- College of NursingDokumen54 halamanCollege of NursingJan VillaminBelum ada peringkat
- Psychological Changes of PregnancyDokumen30 halamanPsychological Changes of PregnancyyuddBelum ada peringkat
- Coxsackievirus NCP W Patho 3Dokumen3 halamanCoxsackievirus NCP W Patho 3Chryst Louise SaavedraBelum ada peringkat
- Idiopathic Thrombocytopenic Purpura (ITP)Dokumen7 halamanIdiopathic Thrombocytopenic Purpura (ITP)Rizqka PertiwiBelum ada peringkat
- Acute Glomerulonephritis (AGN) : Group A Beta Hemolytic StretococcusDokumen3 halamanAcute Glomerulonephritis (AGN) : Group A Beta Hemolytic StretococcusKristine Danielle DejeloBelum ada peringkat
- Nursing Management Pancreatic CancerDokumen2 halamanNursing Management Pancreatic CancerKit NameKo100% (2)
- Gastric Ulcers: Presented By: Dr. Jawaria Memon & Dr. Deep KumarDokumen31 halamanGastric Ulcers: Presented By: Dr. Jawaria Memon & Dr. Deep KumarDeep KhemaniBelum ada peringkat
- Abortion BSN 0PR-2: Case Study of BelleDokumen27 halamanAbortion BSN 0PR-2: Case Study of BellekervinBelum ada peringkat
- MalnutritionDokumen5 halamanMalnutritionCarlo Pasaol Alang Jr.Belum ada peringkat
- Tranexamic AcidDokumen3 halamanTranexamic AcidMuhammad AliBelum ada peringkat
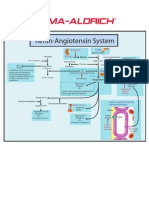
- Renin-Angiotensin SystemDokumen1 halamanRenin-Angiotensin SystemSigma-Aldrich100% (2)
- ONCOLOGIC NURSING: CELLULAR ABERRATIONDokumen68 halamanONCOLOGIC NURSING: CELLULAR ABERRATIONIsrael AgrisBelum ada peringkat
- EndometriosisDokumen6 halamanEndometriosissalamredBelum ada peringkat
- Readings about SplenectomyDokumen7 halamanReadings about SplenectomynessajoanBelum ada peringkat
- Teaching Plan (Diet and Treatment)Dokumen6 halamanTeaching Plan (Diet and Treatment)King Aldus ConstantinoBelum ada peringkat
- Breast FeedingDokumen18 halamanBreast FeedingAnis Rakhmawati100% (1)
- Case 052: Biliary ColicDokumen4 halamanCase 052: Biliary ColicZauzaBelum ada peringkat
- Dysfunctional Labor DystociaDokumen8 halamanDysfunctional Labor Dystociamardsz100% (2)
- BronchiolitisDokumen45 halamanBronchiolitisYuusuf MubarikBelum ada peringkat
- Weaning Foods For InfantsDokumen24 halamanWeaning Foods For InfantsMandeep SinghBelum ada peringkat
- CholelitiasisDokumen42 halamanCholelitiasisEdwin YosuaBelum ada peringkat
- Acute Cholecystitis SeminarDokumen42 halamanAcute Cholecystitis SeminarNatnaelBelum ada peringkat
- Critical Thinking Case Study PharmaDokumen2 halamanCritical Thinking Case Study Pharmakimberly magsipocBelum ada peringkat
- Live Preterm Baby Delivered NSDDokumen13 halamanLive Preterm Baby Delivered NSDKristine Anne SorianoBelum ada peringkat
- Malnutritiom and Anemia ImciDokumen30 halamanMalnutritiom and Anemia ImcibaridacheBelum ada peringkat
- ETHICO OutlineDokumen5 halamanETHICO Outline'emotera' Gudbai DotaBelum ada peringkat
- Case Study CholecytitisDokumen3 halamanCase Study CholecytitisLucero HyacinthBelum ada peringkat
- Sexually Transmitted InfectionsDokumen5 halamanSexually Transmitted InfectionsKANT JAMES D. MAHANBelum ada peringkat
- Fetal Growth DisordersDokumen26 halamanFetal Growth DisordersEdalyn CapiliBelum ada peringkat
- Medical Nutrition Therapy For Accessory OrgansDokumen83 halamanMedical Nutrition Therapy For Accessory OrgansIan MendezBelum ada peringkat
- Hepatic EncephalopathyDokumen3 halamanHepatic EncephalopathyAnonymous GIGXKjfLBelum ada peringkat
- Breast AbscessDokumen2 halamanBreast AbscessJoanna Agustin0% (1)
- Endometrial Hyperplasia - Gyn ReviewDokumen18 halamanEndometrial Hyperplasia - Gyn ReviewFedrik Monte Kristo LimbongBelum ada peringkat
- Gallstone DiseaseDokumen14 halamanGallstone DiseaseSuryaAtmajayaBelum ada peringkat
- Complications in PregnancyDokumen36 halamanComplications in PregnancyJADE PATEGABelum ada peringkat
- Reflection PaperDokumen2 halamanReflection PapershanoiapowelllBelum ada peringkat
- Jesinta Kaparang, 2012 PDFDokumen6 halamanJesinta Kaparang, 2012 PDFCornelia AvishaBelum ada peringkat
- Hepatic Abscesses in Immunocompromised Patients - Ultrasonically Guided Percutaneous DrainageDokumen4 halamanHepatic Abscesses in Immunocompromised Patients - Ultrasonically Guided Percutaneous DrainageDicky SangadjiBelum ada peringkat
- Digest 2021 11 07 062604Dokumen2 halamanDigest 2021 11 07 062604Dicky SangadjiBelum ada peringkat
- Intravascular Catheter-Related Infection - Treatment - UpToDateDokumen18 halamanIntravascular Catheter-Related Infection - Treatment - UpToDateDicky SangadjiBelum ada peringkat
- Southern African Journal of Hiv Medicine, Vol 17, No 1 (2016)Dokumen3 halamanSouthern African Journal of Hiv Medicine, Vol 17, No 1 (2016)Dicky SangadjiBelum ada peringkat
- CE (Ra1) F (AK) PF1 (AGAK) PFA (AK) PF2 (PAG)Dokumen2 halamanCE (Ra1) F (AK) PF1 (AGAK) PFA (AK) PF2 (PAG)Dicky SangadjiBelum ada peringkat
- HFHS CKD V6Dokumen76 halamanHFHS CKD V6medicalBelum ada peringkat
- Intravascular Catheter-Related Infectio... Anifestations and Diagnosis - UpToDateDokumen7 halamanIntravascular Catheter-Related Infectio... Anifestations and Diagnosis - UpToDateDicky SangadjiBelum ada peringkat
- Case Report Tropical Disease Journal BaruDokumen4 halamanCase Report Tropical Disease Journal BaruDicky SangadjiBelum ada peringkat
- Amebiasis in HIV-1-Infected Japanese Men: Clinical Features and Response To TherapyDokumen6 halamanAmebiasis in HIV-1-Infected Japanese Men: Clinical Features and Response To TherapyDicky SangadjiBelum ada peringkat
- Stevens-Johnson Syndrome and Toxic Epidermal Necrolysis - Pathogenesis, Clinical Manifestations, and Diagnosis - UpToDateDokumen41 halamanStevens-Johnson Syndrome and Toxic Epidermal Necrolysis - Pathogenesis, Clinical Manifestations, and Diagnosis - UpToDateDicky SangadjiBelum ada peringkat
- Gallstone Pancreatitis Without Cholecystectomy: Original InvestigationDokumen6 halamanGallstone Pancreatitis Without Cholecystectomy: Original InvestigationDicky SangadjiBelum ada peringkat
- 1756 0500 4 80Dokumen8 halaman1756 0500 4 80Dicky SangadjiBelum ada peringkat
- Longworth 2015Dokumen4 halamanLongworth 2015Dicky SangadjiBelum ada peringkat
- Vascularaccess - 508 HemoDokumen8 halamanVascularaccess - 508 HemoAnnisa KartikasariBelum ada peringkat
- Pathogenesis and Diagnosis of Anti-GBM Antibody (Goodpasture's) DiseaseDokumen18 halamanPathogenesis and Diagnosis of Anti-GBM Antibody (Goodpasture's) DiseaseDicky SangadjiBelum ada peringkat
- GOLD Report 2015 Sept2Dokumen117 halamanGOLD Report 2015 Sept2Dicky SangadjiBelum ada peringkat
- Billiary Sludge and Pancreatitis During PregnancyDokumen5 halamanBilliary Sludge and Pancreatitis During PregnancyDicky SangadjiBelum ada peringkat
- Immunological Mechanisms For Desensitization and Tolerance in Food Allergy (Rachid, 2012)Dokumen14 halamanImmunological Mechanisms For Desensitization and Tolerance in Food Allergy (Rachid, 2012)Dicky SangadjiBelum ada peringkat
- Paliative Care GuidelineDokumen12 halamanPaliative Care GuidelineDicky SangadjiBelum ada peringkat
- Gallstone Pancreatitis Without Cholecystectomy: Original InvestigationDokumen6 halamanGallstone Pancreatitis Without Cholecystectomy: Original InvestigationDicky SangadjiBelum ada peringkat
- Prevention and Management of Postpartum FiaemorrhageDokumen1 halamanPrevention and Management of Postpartum FiaemorrhageDicky SangadjiBelum ada peringkat
- HPP KuDokumen1 halamanHPP KuDicky SangadjiBelum ada peringkat
- Supplementary Feeding ProgramDokumen2 halamanSupplementary Feeding ProgramVictor Anthony CuaresmaBelum ada peringkat
- Seizure Acute ManagementDokumen29 halamanSeizure Acute ManagementFridayana SekaiBelum ada peringkat
- Comparison of Infrastructure in Punjab and Andhra PradeshDokumen7 halamanComparison of Infrastructure in Punjab and Andhra PradeshDivyam GXBelum ada peringkat
- Ipao Program Flyer 17novDokumen1 halamanIpao Program Flyer 17novapi-246252391Belum ada peringkat
- Pvpsit Department of Mechanical Engineering PVP19Dokumen2 halamanPvpsit Department of Mechanical Engineering PVP19Satya NarayanaBelum ada peringkat
- Certificate of Employment Document TitleDokumen1 halamanCertificate of Employment Document TitleAyni ReyesBelum ada peringkat
- Q A With Jaquelyn BurrerDokumen3 halamanQ A With Jaquelyn Burrerapi-480718823Belum ada peringkat
- Adrv9008 1Dokumen68 halamanAdrv9008 1doubleBelum ada peringkat
- What It Is and The Six Steps Necessary To Achieve ItDokumen40 halamanWhat It Is and The Six Steps Necessary To Achieve ItMalory RobayoBelum ada peringkat
- Acute Atelectasis Prevention & TreatmentDokumen9 halamanAcute Atelectasis Prevention & TreatmentmetabolismeproteinBelum ada peringkat
- ECG ProjectDokumen34 halamanECG Projectsamsai888Belum ada peringkat
- B152 01 00 00 00Dokumen517 halamanB152 01 00 00 00lsep_bellaBelum ada peringkat
- Eng & FLS Standards Rev.1 (Dec. 2018)Dokumen72 halamanEng & FLS Standards Rev.1 (Dec. 2018)Nalan BAHCEKAPILIBelum ada peringkat
- Questions That Appear On Every NBMEDokumen6 halamanQuestions That Appear On Every NBMESanz100% (1)
- Materi Bahasa Inggris Kelas 9 - LabelsDokumen12 halamanMateri Bahasa Inggris Kelas 9 - LabelsEnglish Is fun67% (3)
- Archives of Oral Biology 100 (2019) 42-48Dokumen7 halamanArchives of Oral Biology 100 (2019) 42-48pedro cuellar proBelum ada peringkat
- Dimensions-Mm (Inch) : Valve Regulated Lead Acid Battery (VRLA)Dokumen2 halamanDimensions-Mm (Inch) : Valve Regulated Lead Acid Battery (VRLA)orunmila123Belum ada peringkat
- Manual Murray 20Dokumen28 halamanManual Murray 20freebanker777741Belum ada peringkat
- Weld Procedure Specification (WPS) : Joint Design Welding SequenceDokumen1 halamanWeld Procedure Specification (WPS) : Joint Design Welding SequenceRicardo SoaresBelum ada peringkat
- Gas Booster Systems Brochure r7Dokumen12 halamanGas Booster Systems Brochure r7ridwansaungnage_5580Belum ada peringkat
- Excel - All Workout Routines Exercises Reps Sets EtcDokumen10 halamanExcel - All Workout Routines Exercises Reps Sets EtcJanus Blacklight100% (1)
- Annotated Bibliography Graphic OrganizerDokumen4 halamanAnnotated Bibliography Graphic Organizerapi-348035481Belum ada peringkat
- EIM GRADE 9 10 Q4 Module 1b - National Electrical Code NEC Provisions in Installing Wiring Devices - GFCI. - FinalDokumen23 halamanEIM GRADE 9 10 Q4 Module 1b - National Electrical Code NEC Provisions in Installing Wiring Devices - GFCI. - FinalTitser Ramca100% (3)
- Arthropods: A Guide to the Diverse PhylumDokumen10 halamanArthropods: A Guide to the Diverse Phylumpkkalai112Belum ada peringkat
- Ganga Pollution CasesDokumen3 halamanGanga Pollution CasesRuchita KaundalBelum ada peringkat
- Bhima Devi Poudel Adhikari Year 2 Assignment 1 - 220179000Dokumen10 halamanBhima Devi Poudel Adhikari Year 2 Assignment 1 - 220179000api-525310113Belum ada peringkat
- ISO 9001 2008-List of Sample Audit QuestionsDokumen5 halamanISO 9001 2008-List of Sample Audit QuestionsSaut Maruli Tua SamosirBelum ada peringkat
- Agri & Food Processing - Biscuit Manufacturing UnitDokumen6 halamanAgri & Food Processing - Biscuit Manufacturing Unitvijayind2006Belum ada peringkat
- Islamic Personal Law Course OutlineDokumen27 halamanIslamic Personal Law Course OutlineBilal MalikBelum ada peringkat
- Bio23 LindenDokumen34 halamanBio23 LindenDjamal ToeBelum ada peringkat
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionDari EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionPenilaian: 4 dari 5 bintang4/5 (402)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessDari EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessPenilaian: 4.5 dari 5 bintang4.5/5 (327)
- The Age of Magical Overthinking: Notes on Modern IrrationalityDari EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityPenilaian: 4 dari 5 bintang4/5 (13)
- The Ultimate Guide To Memory Improvement TechniquesDari EverandThe Ultimate Guide To Memory Improvement TechniquesPenilaian: 5 dari 5 bintang5/5 (34)
- Techniques Exercises And Tricks For Memory ImprovementDari EverandTechniques Exercises And Tricks For Memory ImprovementPenilaian: 4.5 dari 5 bintang4.5/5 (40)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsDari EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsPenilaian: 3.5 dari 5 bintang3.5/5 (3)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeDari EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeBelum ada peringkat
- The Comfort of Crows: A Backyard YearDari EverandThe Comfort of Crows: A Backyard YearPenilaian: 4.5 dari 5 bintang4.5/5 (23)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedDari EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedPenilaian: 5 dari 5 bintang5/5 (78)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisDari EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisPenilaian: 4 dari 5 bintang4/5 (1)
- Why We Die: The New Science of Aging and the Quest for ImmortalityDari EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityPenilaian: 3.5 dari 5 bintang3.5/5 (2)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsDari EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsBelum ada peringkat
- The Obesity Code: Unlocking the Secrets of Weight LossDari EverandThe Obesity Code: Unlocking the Secrets of Weight LossPenilaian: 5 dari 5 bintang5/5 (3)
- The Happiness Trap: How to Stop Struggling and Start LivingDari EverandThe Happiness Trap: How to Stop Struggling and Start LivingPenilaian: 4 dari 5 bintang4/5 (1)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingDari EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingPenilaian: 5 dari 5 bintang5/5 (4)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingDari EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingPenilaian: 3.5 dari 5 bintang3.5/5 (31)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsDari EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsPenilaian: 4.5 dari 5 bintang4.5/5 (169)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaDari EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- The Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsDari EverandThe Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsBelum ada peringkat
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisDari EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisPenilaian: 4.5 dari 5 bintang4.5/5 (41)
- The Tennis Partner: A Doctor's Story of Friendship and LossDari EverandThe Tennis Partner: A Doctor's Story of Friendship and LossPenilaian: 4.5 dari 5 bintang4.5/5 (4)
- Summary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisDari EverandSummary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisPenilaian: 5 dari 5 bintang5/5 (3)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Dari EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Penilaian: 4.5 dari 5 bintang4.5/5 (110)
- Summary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisDari EverandSummary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisPenilaian: 5 dari 5 bintang5/5 (8)