Anda mungkin juga menyukai
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- Lab Result in EnglishDokumen3 halamanLab Result in EnglishirdinamarchsyaBelum ada peringkat
- Terms of ReferenceDokumen3 halamanTerms of ReferenceirdinamarchsyaBelum ada peringkat
- Pre Training Discussion - BD FACSLyricDokumen48 halamanPre Training Discussion - BD FACSLyricirdinamarchsyaBelum ada peringkat
- 2021 Course Outline Operations Management Tutorial MTM C10Dokumen5 halaman2021 Course Outline Operations Management Tutorial MTM C10irdinamarchsyaBelum ada peringkat
- Competency Are Your Staff Adequately TrainedDokumen22 halamanCompetency Are Your Staff Adequately TrainedirdinamarchsyaBelum ada peringkat
- The Challenges and Benefit of Internal Auditing PDFDokumen27 halamanThe Challenges and Benefit of Internal Auditing PDFirdinamarchsyaBelum ada peringkat
- Manufacture of QCDokumen19 halamanManufacture of QCirdinamarchsyaBelum ada peringkat
- Blood Transfusion: Teoman SOYSAL Prof. MDDokumen38 halamanBlood Transfusion: Teoman SOYSAL Prof. MDirdinamarchsyaBelum ada peringkat
- Physicians Statement 0-2Dokumen1 halamanPhysicians Statement 0-2irdinamarchsyaBelum ada peringkat
- Antibiotik Yg Ada D RSKDDokumen1 halamanAntibiotik Yg Ada D RSKDirdinamarchsyaBelum ada peringkat
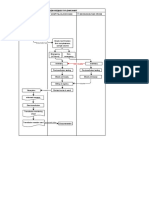
- Blood Request FlowchartDokumen1 halamanBlood Request FlowchartirdinamarchsyaBelum ada peringkat
- 01 - Current Draft WHO-CDC Biosafety RecommendationsDokumen32 halaman01 - Current Draft WHO-CDC Biosafety RecommendationsitsruriBelum ada peringkat
- Uji Validasi Metode Tes Alat Hematologi Sysmex Xnl350Dokumen1 halamanUji Validasi Metode Tes Alat Hematologi Sysmex Xnl350irdinamarchsyaBelum ada peringkat
- TAT For Issuing Blood Products in EmergencyDokumen4 halamanTAT For Issuing Blood Products in Emergencyirdinamarchsya100% (1)
- Malignant or Benign Leukocytosis: Tracy I. GeorgeDokumen10 halamanMalignant or Benign Leukocytosis: Tracy I. GeorgeirdinamarchsyaBelum ada peringkat
- Establishment of Reference Ranges For SPE in The Pediatric Population - A. FogliDokumen1 halamanEstablishment of Reference Ranges For SPE in The Pediatric Population - A. FogliirdinamarchsyaBelum ada peringkat
- Prinsip Kerja MGITDokumen6 halamanPrinsip Kerja MGITirdinamarchsyaBelum ada peringkat
- Myeloproliferative Disorders by T1kaDokumen48 halamanMyeloproliferative Disorders by T1kairdinamarchsyaBelum ada peringkat
- Neonatal Fungal InfectionDokumen4 halamanNeonatal Fungal InfectionirdinamarchsyaBelum ada peringkat
- Use of IGRA For Diagnosis of TB PleurisyDokumen7 halamanUse of IGRA For Diagnosis of TB PleurisyirdinamarchsyaBelum ada peringkat
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (400)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (74)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- TPT 510 Topic 3 - Warehouse in Relief OperationDokumen41 halamanTPT 510 Topic 3 - Warehouse in Relief OperationDR ABDUL KHABIR RAHMATBelum ada peringkat
- Soal PTS Vii BigDokumen6 halamanSoal PTS Vii Bigdimas awe100% (1)
- 5024Dokumen2 halaman5024Luis JesusBelum ada peringkat
- Instructional Decision MakingDokumen5 halamanInstructional Decision Makingapi-257693907Belum ada peringkat
- Roles of Community Health NursingDokumen2 halamanRoles of Community Health Nursingdy kimBelum ada peringkat
- 8 TH Linear Equations DBDokumen1 halaman8 TH Linear Equations DBParth GoyalBelum ada peringkat
- Application Tracking System: Mentor - Yamini Ma'AmDokumen10 halamanApplication Tracking System: Mentor - Yamini Ma'AmBHuwanBelum ada peringkat
- A B&C - List of Residents - VKRWA 12Dokumen10 halamanA B&C - List of Residents - VKRWA 12blr.visheshBelum ada peringkat
- Grand Chapter Mentor ProgramDokumen13 halamanGrand Chapter Mentor ProgramJulius Wright100% (1)
- Ericsson AXE 810: Switch (ROTD)Dokumen4 halamanEricsson AXE 810: Switch (ROTD)Kao Sun HoBelum ada peringkat
- How To Spend An Hour A Day in Prayer - Matthew 26:40-41Dokumen1 halamanHow To Spend An Hour A Day in Prayer - Matthew 26:40-41Steve GainesBelum ada peringkat
- SAMPLE Forklift Safety ProgramDokumen5 halamanSAMPLE Forklift Safety ProgramSudiatmoko SupangkatBelum ada peringkat
- ArticleDokumen9 halamanArticleElly SufriadiBelum ada peringkat
- ASC 2020-21 Questionnaire PDFDokumen11 halamanASC 2020-21 Questionnaire PDFShama PhotoBelum ada peringkat
- Introduction of Woman Role in SocietyDokumen12 halamanIntroduction of Woman Role in SocietyApple DogBelum ada peringkat
- Differentiating Language Difference and Language Disorder - Information For Teachers Working With English Language Learners in The Schools PDFDokumen23 halamanDifferentiating Language Difference and Language Disorder - Information For Teachers Working With English Language Learners in The Schools PDFIqra HassanBelum ada peringkat
- Menu Planning in HospitalDokumen4 halamanMenu Planning in HospitalERva Soelkarnaen100% (1)
- IO5 Future Skills Foresight 2030 ReportDokumen96 halamanIO5 Future Skills Foresight 2030 ReportjuliavalleBelum ada peringkat
- To Word AkheebDokumen31 halamanTo Word AkheebDavid Raju GollapudiBelum ada peringkat
- Beyond The Breech Trial. Maggie BanksDokumen4 halamanBeyond The Breech Trial. Maggie Bankspurpleanvil100% (2)
- Dr. N. Kumarappan IE (I) Council Candidate - Electrical DivisionDokumen1 halamanDr. N. Kumarappan IE (I) Council Candidate - Electrical Divisionshanmugasundaram32Belum ada peringkat
- 12.3 What Is The Nomenclature System For CFCS/HCFCS/HFCS? (Chemistry)Dokumen3 halaman12.3 What Is The Nomenclature System For CFCS/HCFCS/HFCS? (Chemistry)Riska IndriyaniBelum ada peringkat
- Challenges Affecting Devolution PDFDokumen94 halamanChallenges Affecting Devolution PDFELIJAH M. OMBEOBelum ada peringkat
- KRPL Shahjahanpur Check List For Arc Welding MachineDokumen1 halamanKRPL Shahjahanpur Check List For Arc Welding MachineA S YadavBelum ada peringkat
- FRQ Vocabulary ReviewDokumen1 halamanFRQ Vocabulary ReviewDrew AbbottBelum ada peringkat
- Answer KeyDokumen4 halamanAnswer KeyLouina YnciertoBelum ada peringkat
- The Four Types of Gaps and How To Play Them PDFDokumen17 halamanThe Four Types of Gaps and How To Play Them PDFshaikiftakar100% (2)
- User Manual PocketBookDokumen74 halamanUser Manual PocketBookmisu2001Belum ada peringkat
- Questionnaire OriginalDokumen6 halamanQuestionnaire OriginalJAGATHESANBelum ada peringkat
- Adolescents and Career DevelopmentDokumen10 halamanAdolescents and Career DevelopmentMasrijah MasirBelum ada peringkat