Anda mungkin juga menyukai
- Management DeshidratationDokumen15 halamanManagement DeshidratationDani G CeñalBelum ada peringkat
- Guide For History Taking, Physical Exam and Diagnosis of Pediatric PatientsDokumen19 halamanGuide For History Taking, Physical Exam and Diagnosis of Pediatric PatientsKendall Marie BuenavistaBelum ada peringkat
- Assessing and Treating Dehydration in ChildrenDokumen3 halamanAssessing and Treating Dehydration in ChildrenzikraalfaBelum ada peringkat
- Apgar Scoring: 1. Congenital Hypothyroidism (CH)Dokumen2 halamanApgar Scoring: 1. Congenital Hypothyroidism (CH)Khie-An OcampoBelum ada peringkat
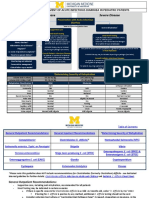
- CPG Acute Infectious Diarrhea Pocket Guide v2Dokumen21 halamanCPG Acute Infectious Diarrhea Pocket Guide v2Moonyeen Jann Casera BalicBelum ada peringkat
- Evaluationandmanagement Ofdehydrationinchildren: Genevieve Santillanes,, Emily RoseDokumen15 halamanEvaluationandmanagement Ofdehydrationinchildren: Genevieve Santillanes,, Emily RoseSandra Díaz MercadoBelum ada peringkat
- 4-Lifespan-Ch 4 - Birth & Physical Dev 1st 3 YearsDokumen15 halaman4-Lifespan-Ch 4 - Birth & Physical Dev 1st 3 YearsJoseph Barnes100% (1)
- DehydrationDokumen23 halamanDehydrationEusebius01Belum ada peringkat
- Hypoxic-Ischaemic Encephalopathy (HIE) : Maternity and Neonatal Clinical GuidelineDokumen27 halamanHypoxic-Ischaemic Encephalopathy (HIE) : Maternity and Neonatal Clinical GuidelineGordon InformationBelum ada peringkat
- Exam 3 Blueprint: Normal Bowel and Bladder PatternsDokumen63 halamanExam 3 Blueprint: Normal Bowel and Bladder Patternswedad jumaBelum ada peringkat
- Bronchiolitis Assessment and Care PathwayDokumen2 halamanBronchiolitis Assessment and Care PathwaydrgrizahBelum ada peringkat
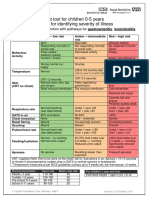
- cs50218 Nhs Fever Pathway For Remote Assessment in Primary Care Oct 19 v4Dokumen1 halamancs50218 Nhs Fever Pathway For Remote Assessment in Primary Care Oct 19 v4api-368117988Belum ada peringkat
- Protocol of DehydrationDokumen3 halamanProtocol of DehydrationHamza El-ȜfifiBelum ada peringkat
- Pediatrics Fluid and Electrolyte Maintenance CalculationDokumen26 halamanPediatrics Fluid and Electrolyte Maintenance CalculationAliaaBelum ada peringkat
- Nursing Care of The New Born InfantDokumen37 halamanNursing Care of The New Born Infantnila_sarichandraBelum ada peringkat
- Kuliah S2 AirDokumen23 halamanKuliah S2 AirViany RehansyahBelum ada peringkat
- Preterm Complications..Dokumen89 halamanPreterm Complications..UdayBhaskar ChinthaBelum ada peringkat
- Immediate Newborn CareDokumen9 halamanImmediate Newborn CareLj FerolinoBelum ada peringkat
- 3.15 Febrile Child Under 5 Years Without A FocusDokumen8 halaman3.15 Febrile Child Under 5 Years Without A Focusiffi82Belum ada peringkat
- Neonatal Jaundice: ObjectivesDokumen12 halamanNeonatal Jaundice: ObjectivesMadx VBelum ada peringkat
- PEDIATRIC ASSESSMENT OVERVIEWDokumen2 halamanPEDIATRIC ASSESSMENT OVERVIEWAghnia Nafila100% (1)
- Total Daily Fluid Requirement For Infants 3.5 To 10 KG 100 ML/KGDokumen4 halamanTotal Daily Fluid Requirement For Infants 3.5 To 10 KG 100 ML/KGKim AlvarezBelum ada peringkat
- Traffic Light SystemDokumen2 halamanTraffic Light SystemErick PrasetyaBelum ada peringkat
- Neonatal Jaundice: Carolyn Joy Mendoza-Capisnon Geraldine Marie SalvoDokumen46 halamanNeonatal Jaundice: Carolyn Joy Mendoza-Capisnon Geraldine Marie SalvoCarolyn CapisnonBelum ada peringkat
- Guidelines for treating pediatric infectious diarrheaDokumen10 halamanGuidelines for treating pediatric infectious diarrheaOasis LimitedBelum ada peringkat
- Principles of Physical AssessmentDokumen58 halamanPrinciples of Physical AssessmentAnna Fayeziah YussophBelum ada peringkat
- Paediatrics LOs for Newborn ExaminationDokumen4 halamanPaediatrics LOs for Newborn ExaminationjassbhanguBelum ada peringkat
- Mother & Baby Together Warm Room Fresh Clean Sheet/clothes Thermometer Weighing Scale Watch With Seconds StethoscopeDokumen50 halamanMother & Baby Together Warm Room Fresh Clean Sheet/clothes Thermometer Weighing Scale Watch With Seconds StethoscopeAnna Fayeziah YussophBelum ada peringkat
- UIAA MedCom Rec No 9 Children at Altitude 2008 V1-1 PDFDokumen14 halamanUIAA MedCom Rec No 9 Children at Altitude 2008 V1-1 PDFHussain SyedBelum ada peringkat
- Medical Management Diabetes BWDokumen7 halamanMedical Management Diabetes BWKe ShBelum ada peringkat
- Palpation: Using The Sense of TouchDokumen54 halamanPalpation: Using The Sense of TouchAnna Fayeziah YussophBelum ada peringkat
- PIL4Dokumen4 halamanPIL4Balmukund kumarBelum ada peringkat
- Ina Pedia1Dokumen14 halamanIna Pedia1Kristil ChavezBelum ada peringkat
- PediaDokumen52 halamanPediakayperez100% (1)
- Nursing Care of Newborn 1 PDFDokumen15 halamanNursing Care of Newborn 1 PDFLaeli Nur HanifahBelum ada peringkat
- Juwak, Jassim - Act 2Dokumen4 halamanJuwak, Jassim - Act 2JASSIM JUWAKBelum ada peringkat
- Managing Dehydration and Electrolyte ImbalancesDokumen14 halamanManaging Dehydration and Electrolyte ImbalancesAzariah EbenezerBelum ada peringkat
- Care of The NewbornDokumen5 halamanCare of The Newbornbuzz Q100% (2)
- Newborn Assessment Prepared PDFDokumen9 halamanNewborn Assessment Prepared PDFBasmalah AlzabenBelum ada peringkat
- Malnutrition Ug ManualDokumen6 halamanMalnutrition Ug ManualJagdish KalsariyaBelum ada peringkat
- 8 PaediatricsDokumen74 halaman8 PaediatricsJeff CrocombeBelum ada peringkat
- CasePres (OLMGH) Germanorig.Dokumen81 halamanCasePres (OLMGH) Germanorig.Jenness VillanuevaBelum ada peringkat
- IMCIDokumen7 halamanIMCImarlou agananBelum ada peringkat
- Classification by Gestational Age Preterm 42 WksDokumen46 halamanClassification by Gestational Age Preterm 42 WksAnna Fayeziah YussophBelum ada peringkat
- Cornell's Note 4Dokumen5 halamanCornell's Note 4Angel BriboneriaBelum ada peringkat
- Pediatric Triage PatDokumen52 halamanPediatric Triage Patdrsapnataneja100% (1)
- MSU Newborn Practices GuideDokumen3 halamanMSU Newborn Practices GuideMimie CaliBelum ada peringkat
- Case PresentationDokumen15 halamanCase PresentationJohn PaciaBelum ada peringkat
- Penatalaksanaan Nutrisi Pada KepDokumen42 halamanPenatalaksanaan Nutrisi Pada KepyufapipiBelum ada peringkat
- Diarrhea PediaDokumen10 halamanDiarrhea PediaSuneeth Kumar MohantyBelum ada peringkat
- Physical Examination of The Pediatric Client: Childhood Developmental StagesDokumen14 halamanPhysical Examination of The Pediatric Client: Childhood Developmental Stagesshannon c. lewisBelum ada peringkat
- 1 - Drugs Affecting Breast and Milk LactationDokumen14 halaman1 - Drugs Affecting Breast and Milk LactationAmmar Bin KhalilBelum ada peringkat
- Dehydration in Peads: Nora Edora Francis PPW 23, Etd Hqe 2Dokumen16 halamanDehydration in Peads: Nora Edora Francis PPW 23, Etd Hqe 2Maman GundohingBelum ada peringkat
- Neonatal JaundiveDokumen15 halamanNeonatal JaundiveCarolyn CapisnonBelum ada peringkat
- Pediatrics MnemonicsDokumen21 halamanPediatrics Mnemonicsdrabhisheck50% (2)
- HomeworkDokumen22 halamanHomeworkLiane BartolomeBelum ada peringkat
- Techniques of Physical Assessment: Observation /inspection Palpation Percussion AuscultationDokumen56 halamanTechniques of Physical Assessment: Observation /inspection Palpation Percussion AuscultationAnna Fayeziah YussophBelum ada peringkat
- Paediatric Booklet by Win Nursing CoachingDokumen116 halamanPaediatric Booklet by Win Nursing CoachingAkshya YadavBelum ada peringkat
- Overview IEMDokumen42 halamanOverview IEMSanti PadmasariBelum ada peringkat
- Cross-Sectional Studies and Measures of Disease Occurrence and AssociationDokumen25 halamanCross-Sectional Studies and Measures of Disease Occurrence and AssociationSanti PadmasariBelum ada peringkat
- Pediatric Trauma - David E Wesson PDFDokumen446 halamanPediatric Trauma - David E Wesson PDFSanti Padmasari100% (1)
- Mechanical Intestinal Obstruction Causes and SymptomsDokumen10 halamanMechanical Intestinal Obstruction Causes and SymptomstatadhBelum ada peringkat
- The Basics of A Modular System: Karolina KósaDokumen15 halamanThe Basics of A Modular System: Karolina KósaSanti PadmasariBelum ada peringkat
- CARDIOVASC06Dokumen73 halamanCARDIOVASC06Santi PadmasariBelum ada peringkat
- TRP HormonDokumen25 halamanTRP HormonSanti PadmasariBelum ada peringkat
- Nutrition in Aging: Endy P. PrawirohartonoDokumen30 halamanNutrition in Aging: Endy P. PrawirohartonoSanti PadmasariBelum ada peringkat
- Anti-virus GuideDokumen57 halamanAnti-virus GuideSanti PadmasariBelum ada peringkat
- Cardiotonics: Dept. of Pharmacology and Toxicology Faculty of Medicine GMUDokumen44 halamanCardiotonics: Dept. of Pharmacology and Toxicology Faculty of Medicine GMUSanti PadmasariBelum ada peringkat
- Cardiotonics: Dept. of Pharmacology and Toxicology Faculty of Medicine GMUDokumen44 halamanCardiotonics: Dept. of Pharmacology and Toxicology Faculty of Medicine GMUSanti PadmasariBelum ada peringkat
- Introduction To Clinical Epidemiology: Spring 1999 ElectiveDokumen29 halamanIntroduction To Clinical Epidemiology: Spring 1999 ElectiveSanti PadmasariBelum ada peringkat
- Angp CadDokumen22 halamanAngp CadSanti PadmasariBelum ada peringkat
- FARMAKOTERAPI OBAT PADA PENYAKIT BATU SALURAN KEMIHDokumen38 halamanFARMAKOTERAPI OBAT PADA PENYAKIT BATU SALURAN KEMIHSanti PadmasariBelum ada peringkat
- Lecture 8b Inference June 22Dokumen55 halamanLecture 8b Inference June 22Santi PadmasariBelum ada peringkat
- Matching & Confounding AnalysisDokumen51 halamanMatching & Confounding AnalysisSanti PadmasariBelum ada peringkat
- 03N 0201 TS00010Dokumen24 halaman03N 0201 TS00010Santi PadmasariBelum ada peringkat
- Determinants of Community Health: Power SearchingDokumen40 halamanDeterminants of Community Health: Power SearchingSanti PadmasariBelum ada peringkat
- ACOEM Practice Guidelines: Perspectives On Their Use in Guiding Clinical Care and Utilization ManagementDokumen37 halamanACOEM Practice Guidelines: Perspectives On Their Use in Guiding Clinical Care and Utilization ManagementSanti PadmasariBelum ada peringkat
- CDC: Obesity Approaching Tobacco As Top Preventable Cause of DeathDokumen2 halamanCDC: Obesity Approaching Tobacco As Top Preventable Cause of DeathSanti PadmasariBelum ada peringkat
- From Clinical Observations To Research: Dr. Dick Menzies June 10, 2005Dokumen36 halamanFrom Clinical Observations To Research: Dr. Dick Menzies June 10, 2005Santi PadmasariBelum ada peringkat
- Introduction To Clinical Epidemiology: Spring 1999 ElectiveDokumen29 halamanIntroduction To Clinical Epidemiology: Spring 1999 ElectiveSanti PadmasariBelum ada peringkat
- SpeechDokumen2 halamanSpeechSanti PadmasariBelum ada peringkat
- Pedoman Nasional TBC AnakDokumen32 halamanPedoman Nasional TBC AnakSanti PadmasariBelum ada peringkat
- Ari 2003 PDFDokumen30 halamanAri 2003 PDFSanti PadmasariBelum ada peringkat
- Cell Cycle and ApoptosisDokumen31 halamanCell Cycle and ApoptosisSanti PadmasariBelum ada peringkat
- Redefining ObesityDokumen56 halamanRedefining ObesityAntonio PonceBelum ada peringkat
- Corticosteroid Conversion ChartDokumen1 halamanCorticosteroid Conversion ChartSanti PadmasariBelum ada peringkat
- Pediatric ATLS2008Dokumen20 halamanPediatric ATLS2008Santi PadmasariBelum ada peringkat
- Balance System: by M K SastryDokumen33 halamanBalance System: by M K SastryEdison halim100% (3)
- City & Guilds Unit 116: Support The Use of Medication in Social Care SettingsDokumen85 halamanCity & Guilds Unit 116: Support The Use of Medication in Social Care SettingsBex FerridayBelum ada peringkat
- Memoir Reflection PaperDokumen4 halamanMemoir Reflection Paperapi-301417439Belum ada peringkat
- Tetracycline Drug Reporting-2Dokumen21 halamanTetracycline Drug Reporting-2Shynne RPhBelum ada peringkat
- DAB 30102 Environmental Topics ProjectDokumen6 halamanDAB 30102 Environmental Topics ProjectNazsyazana YusofBelum ada peringkat
- Pre TestDokumen3 halamanPre TestBobet Reña100% (1)
- En ModulTechnik Moduflex 2500 2600Dokumen12 halamanEn ModulTechnik Moduflex 2500 2600Razvan PredaBelum ada peringkat
- Club FootDokumen47 halamanClub FootSujanaBelum ada peringkat
- Diabetes BrochureDokumen3 halamanDiabetes Brochureapi-348372254Belum ada peringkat
- Doctor-Patient Communication A ReviewDokumen6 halamanDoctor-Patient Communication A ReviewWagiono SuparanBelum ada peringkat
- Psychology Chapter SevenDokumen25 halamanPsychology Chapter Sevenmelaku zegeyeBelum ada peringkat
- Parenteral Nutrition in NICUDokumen16 halamanParenteral Nutrition in NICUPaulina Kristiani BangunBelum ada peringkat
- Case Conference 011017 (Appendicitis)Dokumen36 halamanCase Conference 011017 (Appendicitis)Lilik NatasubrataBelum ada peringkat
- Raphex Answers 2010 PDFDokumen15 halamanRaphex Answers 2010 PDFcarlosqueiroz7669100% (4)
- Counselling Module EDU3107 by IDRUL HISHAMDokumen209 halamanCounselling Module EDU3107 by IDRUL HISHAMThia SolveBelum ada peringkat
- Mason 2021 Feasibility and Acceptability of ADokumen9 halamanMason 2021 Feasibility and Acceptability of AjorgeBelum ada peringkat
- Scandinavian Guidelines For Initial Management of Minimal, Mild and Moderate Head Injuries in Adults: An Evidence and Consensus-Based UpdateDokumen14 halamanScandinavian Guidelines For Initial Management of Minimal, Mild and Moderate Head Injuries in Adults: An Evidence and Consensus-Based UpdateDesy RusianaBelum ada peringkat
- NCP OsteoarthritisDokumen4 halamanNCP OsteoarthritisKyle Margaret Flores100% (1)
- The Healing Power of Rainforest Herbs PDFDokumen532 halamanThe Healing Power of Rainforest Herbs PDFRaluca Huzum100% (10)
- Uses of Clobetasol Cream, Gel, and OintmentDokumen15 halamanUses of Clobetasol Cream, Gel, and OintmentIntsik LimBelum ada peringkat
- Principles and Practice of Gynecologic Oncology: Handbook ForDokumen288 halamanPrinciples and Practice of Gynecologic Oncology: Handbook ForPeter Osundwa KitekiBelum ada peringkat
- Research Paper: Coaching and Counseling - What Can We Learn From Each Other?Dokumen11 halamanResearch Paper: Coaching and Counseling - What Can We Learn From Each Other?International Coach AcademyBelum ada peringkat
- Why Stomach Acid Is Essential For Our HealthDokumen6 halamanWhy Stomach Acid Is Essential For Our HealthGabriel Turlac100% (1)
- MSDS Chemical InjectionDokumen12 halamanMSDS Chemical InjectionJohnson Lopes100% (1)
- Case StudyDokumen3 halamanCase StudyAvni DhingraBelum ada peringkat
- The Royal Children HospitalDokumen8 halamanThe Royal Children HospitalrenystrawberryBelum ada peringkat
- Hip Fracture Case Study: 39-Year-Old Male with EpilepsyDokumen9 halamanHip Fracture Case Study: 39-Year-Old Male with EpilepsyufuBelum ada peringkat
- Bhs Inggris ElsaDokumen11 halamanBhs Inggris ElsaElsa karuniatiBelum ada peringkat
- Cholesterol Lowering Secrets ReportDokumen12 halamanCholesterol Lowering Secrets ReportSantoshKumarBelum ada peringkat
- Unfinished Agenda - Indian Molecule Going Global - Business Line PDFDokumen2 halamanUnfinished Agenda - Indian Molecule Going Global - Business Line PDFhappinessalways38Belum ada peringkat