Anda mungkin juga menyukai
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- ACFormDokumen5 halamanACFormcommanderkeen100% (1)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (400)
- Assistance Animal Policy and AgreementDokumen5 halamanAssistance Animal Policy and AgreementcommanderkeenBelum ada peringkat
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- Animal Policy Final 012717 PDFDokumen13 halamanAnimal Policy Final 012717 PDFcommanderkeenBelum ada peringkat
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- Service, Assistance, and Other Animals at Northwestern Policy StatementDokumen13 halamanService, Assistance, and Other Animals at Northwestern Policy StatementcommanderkeenBelum ada peringkat
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Service-Assistance Animal Policy in University HousingDokumen6 halamanService-Assistance Animal Policy in University HousingcommanderkeenBelum ada peringkat
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- Goat Medications 2015Dokumen3 halamanGoat Medications 2015commanderkeenBelum ada peringkat
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Service-Assistance Animal Policy in University Housing PDFDokumen6 halamanService-Assistance Animal Policy in University Housing PDFcommanderkeenBelum ada peringkat
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Service and Assistance Animal PolicyDokumen9 halamanService and Assistance Animal PolicycommanderkeenBelum ada peringkat
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- Analyzing Political Cartoons PDFDokumen1 halamanAnalyzing Political Cartoons PDFcommanderkeenBelum ada peringkat
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (73)
- 036 CDokumen12 halaman036 CcommanderkeenBelum ada peringkat
- Animal RequestDokumen5 halamanAnimal RequestcommanderkeenBelum ada peringkat
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- Disability AnimalPolicyDokumen10 halamanDisability AnimalPolicycommanderkeenBelum ada peringkat
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- Physical Activity and Exercise Recent Advances and Current ChallengesDokumen11 halamanPhysical Activity and Exercise Recent Advances and Current ChallengescommanderkeenBelum ada peringkat
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- Analyzing Political CartoonsDokumen1 halamanAnalyzing Political CartoonscommanderkeenBelum ada peringkat
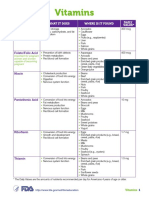
- Special Report: Vitamins and MineralsDokumen8 halamanSpecial Report: Vitamins and MineralscommanderkeenBelum ada peringkat
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Edrv0521 PDFDokumen27 halamanEdrv0521 PDFcommanderkeenBelum ada peringkat
- Vitamin D Sip43 June14 PDFDokumen11 halamanVitamin D Sip43 June14 PDFcommanderkeenBelum ada peringkat
- Ddsig Fact Sheet Exercise and Post Polio Syndrome PDFDokumen3 halamanDdsig Fact Sheet Exercise and Post Polio Syndrome PDFcommanderkeenBelum ada peringkat
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- Eds 21 ManualDokumen9 halamanEds 21 ManualcommanderkeenBelum ada peringkat
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- 147 12 1175 PDFDokumen2 halaman147 12 1175 PDFcommanderkeenBelum ada peringkat
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- ARGFocus 201008 VitaminsDAK WebDokumen16 halamanARGFocus 201008 VitaminsDAK WebcommanderkeenBelum ada peringkat
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- Special Report: Vitamins and MineralsDokumen8 halamanSpecial Report: Vitamins and MineralscommanderkeenBelum ada peringkat
- Foods With Vitamin K PDFDokumen2 halamanFoods With Vitamin K PDFcommanderkeenBelum ada peringkat
- Vitamin D Brochure FINALDokumen3 halamanVitamin D Brochure FINALcommanderkeenBelum ada peringkat
- Edrv 0521Dokumen27 halamanEdrv 0521commanderkeenBelum ada peringkat
- Vitamin and Mineral Chart PDFDokumen5 halamanVitamin and Mineral Chart PDFcommanderkeenBelum ada peringkat
- Vitamin A Deficiency: Health, Survival and Vision: by Alfred Sommer and Keith P. WestDokumen2 halamanVitamin A Deficiency: Health, Survival and Vision: by Alfred Sommer and Keith P. WestcommanderkeenBelum ada peringkat
- Efsa - Tolerable Upper Intake LevelsDokumen482 halamanEfsa - Tolerable Upper Intake LevelsdrantistBelum ada peringkat
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- FINAL VERSION National Guidelines VAS3 PDFDokumen2 halamanFINAL VERSION National Guidelines VAS3 PDFcommanderkeenBelum ada peringkat
- Conduct of Physical Examination: I. General SurveyDokumen10 halamanConduct of Physical Examination: I. General SurveyWeng RamojalBelum ada peringkat
- A&P - 7. Shoulder Girdle & Upper Limb Detailed Anatomy (42p)Dokumen42 halamanA&P - 7. Shoulder Girdle & Upper Limb Detailed Anatomy (42p)andreeaBelum ada peringkat
- Anesthesia For LiposuctionDokumen26 halamanAnesthesia For Liposuctionjulissand10Belum ada peringkat
- 11 Biology Notes ch18 Body Fluids and Circulation PDFDokumen8 halaman11 Biology Notes ch18 Body Fluids and Circulation PDFSumit SinghalBelum ada peringkat
- Approach To Acid BaseDokumen4 halamanApproach To Acid BaseJose Carlos Guerrero AcostaBelum ada peringkat
- In Focus Periodic Paralysis PDFDokumen8 halamanIn Focus Periodic Paralysis PDFLisa Pratiwi RBelum ada peringkat
- CiticolineDokumen8 halamanCiticolineadityaBelum ada peringkat
- Cardiac Rehabilitation ProtocolDokumen5 halamanCardiac Rehabilitation Protocolmarkhabm100% (1)
- General Review Questions in AnimalsDokumen9 halamanGeneral Review Questions in AnimalsAnonymous VkI5xDuBelum ada peringkat
- A Ciência Da Esgrima: Implicações Da Performance e Prevenção de LesõesDokumen18 halamanA Ciência Da Esgrima: Implicações Da Performance e Prevenção de LesõesDaniel GonçalvesBelum ada peringkat
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- Nursing Care Plan For A Patient With Pleural EffusionDokumen5 halamanNursing Care Plan For A Patient With Pleural Effusionmac042250% (4)
- Accepted Manuscript: Ageing Research ReviewsDokumen49 halamanAccepted Manuscript: Ageing Research ReviewsCarolina LucínBelum ada peringkat
- Chronic GlomerulonephritisDokumen6 halamanChronic GlomerulonephritisIsak ShatikaBelum ada peringkat
- Science 9th Chapter 5 Cell Biology NotesDokumen4 halamanScience 9th Chapter 5 Cell Biology NotesavanishBelum ada peringkat
- Airway: Nursing Care PlanDokumen3 halamanAirway: Nursing Care PlanPhoebe Kyles CammaBelum ada peringkat
- ScrotumDokumen17 halamanScrotumcynic mercerBelum ada peringkat
- MeiosisDokumen20 halamanMeiosisRosalina ColetoBelum ada peringkat
- Muscles of MasticationDokumen50 halamanMuscles of MasticationKaran AroraBelum ada peringkat
- Overview of Cell Cycle by Javali.GDokumen15 halamanOverview of Cell Cycle by Javali.GJavali.GBelum ada peringkat
- Information For You: An Ectopic PregnancyDokumen25 halamanInformation For You: An Ectopic PregnancyAnonymous layszXmsBelum ada peringkat
- Sensate FocusDokumen13 halamanSensate FocusMari Forgach100% (1)
- ThreePointer's Guide To Histology Steeple Chase For 022 ClassDokumen54 halamanThreePointer's Guide To Histology Steeple Chase For 022 ClassNnaemeka Neboh100% (1)
- Jurnal 11Dokumen14 halamanJurnal 11Zulvi RiriBelum ada peringkat
- Chapter 9 - Transport in AnimalsDokumen6 halamanChapter 9 - Transport in AnimalsLeann LeeBelum ada peringkat
- Grade 12 Biology Caffeine LabDokumen11 halamanGrade 12 Biology Caffeine Labpokesurfer85% (13)
- Principles of Vegetative PropagationDokumen5 halamanPrinciples of Vegetative PropagationJensenBelum ada peringkat
- IyotDokumen7 halamanIyotMonaimLaraMacabangonIVBelum ada peringkat
- (Julie K. Briggs, Valerie G.A. Grossman BSN CEN Emergency Nursing 5 Tier Triage ProtocolDokumen272 halaman(Julie K. Briggs, Valerie G.A. Grossman BSN CEN Emergency Nursing 5 Tier Triage ProtocolWulan Rahmadani FauziBelum ada peringkat
- Flight PhysiologyDokumen5 halamanFlight PhysiologyRicardo MarmolBelum ada peringkat
- Brilinta (Ticagrelor) Tablets, For Oral UseDokumen2 halamanBrilinta (Ticagrelor) Tablets, For Oral UsePonpimol Odee BongkeawBelum ada peringkat
- Chair Yoga: Sit, Stretch, and Strengthen Your Way to a Happier, Healthier YouDari EverandChair Yoga: Sit, Stretch, and Strengthen Your Way to a Happier, Healthier YouPenilaian: 3.5 dari 5 bintang3.5/5 (5)
- Aging Backwards: Reverse the Aging Process and Look 10 Years Younger in 30 Minutes a DayDari EverandAging Backwards: Reverse the Aging Process and Look 10 Years Younger in 30 Minutes a DayBelum ada peringkat
- Power of 10: The Once-A-Week Slow Motion Fitness RevolutionDari EverandPower of 10: The Once-A-Week Slow Motion Fitness RevolutionPenilaian: 3.5 dari 5 bintang3.5/5 (11)
- The Yogi Code: Seven Universal Laws of Infinite SuccessDari EverandThe Yogi Code: Seven Universal Laws of Infinite SuccessPenilaian: 4.5 dari 5 bintang4.5/5 (104)
- Boundless: Upgrade Your Brain, Optimize Your Body & Defy AgingDari EverandBoundless: Upgrade Your Brain, Optimize Your Body & Defy AgingPenilaian: 4.5 dari 5 bintang4.5/5 (66)
- Functional Training and Beyond: Building the Ultimate Superfunctional Body and MindDari EverandFunctional Training and Beyond: Building the Ultimate Superfunctional Body and MindPenilaian: 4.5 dari 5 bintang4.5/5 (1)
- Peak: The New Science of Athletic Performance That is Revolutionizing SportsDari EverandPeak: The New Science of Athletic Performance That is Revolutionizing SportsPenilaian: 5 dari 5 bintang5/5 (96)