Anda mungkin juga menyukai
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5795)
- Al-Masum ArticleDokumen23 halamanAl-Masum ArticleChhaibi AbderrahimBelum ada peringkat
- How To Read Academic Texts CriticallyDokumen2 halamanHow To Read Academic Texts CriticallyChhaibi AbderrahimBelum ada peringkat
- How To Provide An Artistic ServiceDokumen6 halamanHow To Provide An Artistic ServiceChhaibi AbderrahimBelum ada peringkat
- How To Write A Research Paper ProposalDokumen4 halamanHow To Write A Research Paper ProposalChhaibi AbderrahimBelum ada peringkat
- How To Be An Effective MentorDokumen2 halamanHow To Be An Effective MentorChhaibi AbderrahimBelum ada peringkat
- How To Annotate in Your English ClassDokumen5 halamanHow To Annotate in Your English ClassChhaibi AbderrahimBelum ada peringkat
- PubMed Database Interface ExercisesDokumen6 halamanPubMed Database Interface ExercisesChhaibi AbderrahimBelum ada peringkat
- Access Full Text at NLMDokumen24 halamanAccess Full Text at NLMChhaibi AbderrahimBelum ada peringkat
- CritiqueDokumen2 halamanCritiqueChhaibi AbderrahimBelum ada peringkat
- Adapt Security To Enable Macros in Excel: Step 1Dokumen5 halamanAdapt Security To Enable Macros in Excel: Step 1Chhaibi AbderrahimBelum ada peringkat
- (The Terry Lectures) Carl Gustav Jung-Psychology and Religion - Yale University Press (1960)Dokumen135 halaman(The Terry Lectures) Carl Gustav Jung-Psychology and Religion - Yale University Press (1960)Chhaibi AbderrahimBelum ada peringkat
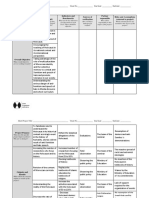
- Intervention Logic Indicators and Benchmarks Sources of Verification Partner Responsible Risks and Assumptions (External To Project)Dokumen3 halamanIntervention Logic Indicators and Benchmarks Sources of Verification Partner Responsible Risks and Assumptions (External To Project)Chhaibi AbderrahimBelum ada peringkat
- Curriculum Mapping HandbookDokumen20 halamanCurriculum Mapping HandbookChhaibi Abderrahim100% (1)
- Dialog Among CivilisationsDokumen199 halamanDialog Among CivilisationsChhaibi AbderrahimBelum ada peringkat
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (74)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (400)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- Definisi: Chong BS. 2017. Harty's Endodontics in Clinical Practice 7 Ed. Elsevier LTDDokumen61 halamanDefinisi: Chong BS. 2017. Harty's Endodontics in Clinical Practice 7 Ed. Elsevier LTDtillahBelum ada peringkat
- Innovative Endodontics Using Sweeps TechnologyDokumen6 halamanInnovative Endodontics Using Sweeps TechnologysoumyaBelum ada peringkat
- Efektifitas Ekstrak Propolis 8% Dan Sodium Hypochlorite (Naocl) 2,5% Terhadap Kebersihan Saluran AkarDokumen7 halamanEfektifitas Ekstrak Propolis 8% Dan Sodium Hypochlorite (Naocl) 2,5% Terhadap Kebersihan Saluran Akarrizal ardiBelum ada peringkat
- Smear LayerDokumen13 halamanSmear LayerDental Spa100% (2)
- A Study On Provisional Cements, Cementation Techniques, and Their Effects On Bonding of Porcelain Laminate VeneersDokumen8 halamanA Study On Provisional Cements, Cementation Techniques, and Their Effects On Bonding of Porcelain Laminate Veneerssnehal jaiswalBelum ada peringkat
- Aiims 2010 November 2010 DentalDokumen62 halamanAiims 2010 November 2010 DentalMrunal Doiphode100% (1)
- Liquid & Paste EdtaDokumen7 halamanLiquid & Paste EdtaLAKSHMI ARORABelum ada peringkat
- Manual Dynamic Activation MDA TechniqueDokumen7 halamanManual Dynamic Activation MDA Techniquesanaemi321Belum ada peringkat
- Root BiomodificationDokumen56 halamanRoot BiomodificationDr Jinal Desai50% (2)
- Aipg 2007 PDFDokumen26 halamanAipg 2007 PDFteju patneediBelum ada peringkat
- Recent Advances in Irrigation Devices: Dr. Bikramjeet Singh Mds 3 YearDokumen84 halamanRecent Advances in Irrigation Devices: Dr. Bikramjeet Singh Mds 3 YearParul ChauhanBelum ada peringkat
- Principles of AdhesionDokumen44 halamanPrinciples of AdhesionOmar Hesham SalahBelum ada peringkat
- Dentin Bonding Agents - An OverviewDokumen4 halamanDentin Bonding Agents - An OverviewIOSRjournalBelum ada peringkat
- Bryce2017 FALTA CITAR Y PONER PARRAFODokumen20 halamanBryce2017 FALTA CITAR Y PONER PARRAFOSTEPHANY MENESES REYESBelum ada peringkat
- Irrigation in EndodonticsDokumen7 halamanIrrigation in EndodonticsAasim YousufBelum ada peringkat
- Irrigating Solutions in Endodontics: A Brief ReviewDokumen9 halamanIrrigating Solutions in Endodontics: A Brief ReviewScienceVolksBelum ada peringkat
- Pulp-Dentin Biology2Dokumen16 halamanPulp-Dentin Biology2Hector Flores SotoBelum ada peringkat
- 120 - Modern Perspectives in RC ObturationDokumen14 halaman120 - Modern Perspectives in RC ObturationLarissa ClipaciucBelum ada peringkat
- Irrigants in EndodonticsDokumen46 halamanIrrigants in EndodonticstomdienyaBelum ada peringkat
- Comparative Evaluation of Efficacy of Three Different Irrigation Activation Systems in Debridement of Root Canal Isthmus: An in Vitro StudyDokumen4 halamanComparative Evaluation of Efficacy of Three Different Irrigation Activation Systems in Debridement of Root Canal Isthmus: An in Vitro StudyHema lathaBelum ada peringkat
- Coronal Leakage As A Cause of Failure in Root-Canal Therapy - A ReviewDokumen5 halamanCoronal Leakage As A Cause of Failure in Root-Canal Therapy - A ReviewFlorin IonescuBelum ada peringkat
- Dentin and Its Clinical ConsiderationDokumen97 halamanDentin and Its Clinical ConsiderationKrithikaBelum ada peringkat
- SynopsisDokumen13 halamanSynopsisharivijay ranmaleBelum ada peringkat
- CerkamedDokumen4 halamanCerkamedDragana CurcicBelum ada peringkat
- Intracanal Medicaments and IrrigantsDokumen85 halamanIntracanal Medicaments and IrrigantsAmit Abbey100% (1)
- Bonding Performance of Universal Adhesives in Different Etching ModesDokumen9 halamanBonding Performance of Universal Adhesives in Different Etching ModesRitter Adolfo OlivaresBelum ada peringkat
- Endo Lec 6 With AudioDokumen44 halamanEndo Lec 6 With AudioمحمدBelum ada peringkat
- Effect of Irrigation Protocol During Post Space Preparation On The Dentin Adhesive Interface - An in Vitro StudyDokumen9 halamanEffect of Irrigation Protocol During Post Space Preparation On The Dentin Adhesive Interface - An in Vitro StudyMayra Ortiz HerreraBelum ada peringkat
- Assessment of Apical Sealing Ability of Retrograde Filling Materials With Gic, Mta, Biodentine and Bioaggregate: An in Vitro StudyDokumen93 halamanAssessment of Apical Sealing Ability of Retrograde Filling Materials With Gic, Mta, Biodentine and Bioaggregate: An in Vitro StudypoojaBelum ada peringkat
- IrigasiDokumen21 halamanIrigasiFatimah DewiBelum ada peringkat