Anda mungkin juga menyukai
- Endo Vs Implant SeminarDokumen25 halamanEndo Vs Implant Seminarsweetminu99100% (1)
- Restorative Management of Dental Implants: 5.1 Basic Implant TerminologyDokumen19 halamanRestorative Management of Dental Implants: 5.1 Basic Implant TerminologyleeminhoangrybirdBelum ada peringkat
- Wound Ostomy Continence Skills ChecklistDokumen4 halamanWound Ostomy Continence Skills ChecklistnorthweststaffingBelum ada peringkat
- Prosthetic SurgeryDokumen14 halamanProsthetic SurgeryCristina CArrera100% (1)
- Medical ImagingDokumen8 halamanMedical ImagingMansourBelum ada peringkat
- Restorative and OcclusionDokumen13 halamanRestorative and OcclusionEhsan Ullah100% (1)
- The Debut Olympia DietDokumen13 halamanThe Debut Olympia DietFrank Black90% (10)
- 3.good Occlusal Practice in Simple Restorative Dentistry PDFDokumen13 halaman3.good Occlusal Practice in Simple Restorative Dentistry PDFaleeza sanaBelum ada peringkat
- Surgery - General SurgeryDokumen58 halamanSurgery - General Surgeryteena6506763100% (1)
- Treatment Planning Single Maxillary Anterior Implants for DentistsDari EverandTreatment Planning Single Maxillary Anterior Implants for DentistsBelum ada peringkat
- Immediate Loading Implants - A Paradigm Shift - A ReviewDokumen4 halamanImmediate Loading Implants - A Paradigm Shift - A ReviewDr. Abdulsalam Awas Dental CenterBelum ada peringkat
- The Chronic Miasms: Chapter SeventeenDokumen17 halamanThe Chronic Miasms: Chapter Seventeenmihaipopescu0100% (2)
- A Review of Selected Dental Literature On Contemporary Provisional FPD S Treatment - Report of The Commmitee On Research in FPD S of The Academy of Fixed ProsthodonticsDokumen24 halamanA Review of Selected Dental Literature On Contemporary Provisional FPD S Treatment - Report of The Commmitee On Research in FPD S of The Academy of Fixed ProsthodonticsLynda M. NaranjoBelum ada peringkat
- ORTHO - Treatment Planning and Management of Class I MalocclusionDokumen31 halamanORTHO - Treatment Planning and Management of Class I MalocclusionLailathul Bathur Kalikul Jaman50% (2)
- Planetary ThreadsDokumen2 halamanPlanetary ThreadsViviana PueblaBelum ada peringkat
- Endodontics or Implants. A Review of Decisive Criteria and GuidelinesDokumen19 halamanEndodontics or Implants. A Review of Decisive Criteria and GuidelinesJuan David Torres CanoBelum ada peringkat
- Dental Implant Treatment Planning for New Dentists Starting Implant TherapyDari EverandDental Implant Treatment Planning for New Dentists Starting Implant TherapyPenilaian: 4 dari 5 bintang4/5 (1)
- Depresion PostpartoDokumen6 halamanDepresion PostpartoOscar Alejandro Cardenas QuinteroBelum ada peringkat
- Contekan KodeDokumen4 halamanContekan KodeTessa Safitri KotoBelum ada peringkat
- TuberculosisDokumen16 halamanTuberculosisjojolim18100% (1)
- Pini Prato and Chambrone 2019-Journal - of - Periodontology PDFDokumen5 halamanPini Prato and Chambrone 2019-Journal - of - Periodontology PDFJayra Elieth Mendoza GomezBelum ada peringkat
- Retention Maintainenece - Conclusion PDFDokumen4 halamanRetention Maintainenece - Conclusion PDFDR HEGDE DENTAL CLINICBelum ada peringkat
- The Retention Protocol 2017 Seminars in OrthodonticsDokumen12 halamanThe Retention Protocol 2017 Seminars in Orthodonticsdruzair007Belum ada peringkat
- 1retention and RelapseDokumen12 halaman1retention and RelapseTara TeraBelum ada peringkat
- Orthodontic Relapse Versus Natural DevelopmentDokumen2 halamanOrthodontic Relapse Versus Natural DevelopmentCatherine NocuaBelum ada peringkat
- Evidence Based Retention Where Are We Now 2017 Seminars in OrthodonticsDokumen8 halamanEvidence Based Retention Where Are We Now 2017 Seminars in Orthodonticsdruzair007Belum ada peringkat
- Retention and Relapse 3Dokumen13 halamanRetention and Relapse 3Tara TeraBelum ada peringkat
- Terminology Semantics of Postorthodontictreatment Cha - 1999 - Seminars in OrthDokumen4 halamanTerminology Semantics of Postorthodontictreatment Cha - 1999 - Seminars in OrthNIKHITABelum ada peringkat
- Occlusal Stability and Mandibular Stability The Major Part of Dentistry We Are Still NeglectingDokumen4 halamanOcclusal Stability and Mandibular Stability The Major Part of Dentistry We Are Still NeglectingdanielaBelum ada peringkat
- Retention Management Decisions A Review of Current Evidence and Emerging Trends 2017 Seminars in OrthodonticsDokumen8 halamanRetention Management Decisions A Review of Current Evidence and Emerging Trends 2017 Seminars in Orthodonticsdruzair007Belum ada peringkat
- Diagnostic Elements For Tooth Extraction in OrthodonticsDokumen24 halamanDiagnostic Elements For Tooth Extraction in OrthodonticsLanaBelum ada peringkat
- Greene 2015Dokumen10 halamanGreene 2015Gabriela TorinoBelum ada peringkat
- Advanced Restorative DentistryDokumen10 halamanAdvanced Restorative DentistrySimona DobreBelum ada peringkat
- 1331-Texto Del Artículo-5697-1-10-20221002 PDFDokumen8 halaman1331-Texto Del Artículo-5697-1-10-20221002 PDFTasha FarahBelum ada peringkat
- Annalsash-Kmdc, 09Dokumen10 halamanAnnalsash-Kmdc, 09Alejandro Arias ErazoBelum ada peringkat
- Oral Diagnosis and Treatment Planning: Part 8. Reviews and Maintenance of RestorationsDokumen8 halamanOral Diagnosis and Treatment Planning: Part 8. Reviews and Maintenance of RestorationsBibek RajBelum ada peringkat
- Tooth WearDokumen7 halamanTooth WearKish BBelum ada peringkat
- Ld-Anoop Full Moth Rehab / Orthodontic Courses by Indian Dental AcademyDokumen279 halamanLd-Anoop Full Moth Rehab / Orthodontic Courses by Indian Dental Academyindian dental academyBelum ada peringkat
- Author's Accepted ManuscriptDokumen24 halamanAuthor's Accepted ManuscriptMargarita Lopez MartinezBelum ada peringkat
- Santosa-2007-Australian Dental JournalDokumen10 halamanSantosa-2007-Australian Dental JournalWidyawati HestiBelum ada peringkat
- Repraising Thoughts On Orthodontic Treatment StabilityDokumen2 halamanRepraising Thoughts On Orthodontic Treatment StabilityMaria Fernanda Garcia PucheBelum ada peringkat
- Retention and Relapse 2Dokumen13 halamanRetention and Relapse 2Tara TeraBelum ada peringkat
- Pini Prato and Chambrone 2019-Journal - of - PeriodontologyDokumen5 halamanPini Prato and Chambrone 2019-Journal - of - PeriodontologyJayra Elieth Mendoza GomezBelum ada peringkat
- LD Anoop Full Moth Rehab Orthodontic Courses by Indian Dental AcademyDokumen279 halamanLD Anoop Full Moth Rehab Orthodontic Courses by Indian Dental AcademyPhanQuangHuyBelum ada peringkat
- Planificación Del Tratamiento de Ortodoncia - ¿Podemos Planificar La Estabilidad?Dokumen5 halamanPlanificación Del Tratamiento de Ortodoncia - ¿Podemos Planificar La Estabilidad?patricio fierroBelum ada peringkat
- Good Occlusal Practice in The Provision of Implant Borne ProsthesesDokumen10 halamanGood Occlusal Practice in The Provision of Implant Borne ProsthesesNoland NaidooBelum ada peringkat
- Articol 1 PDFDokumen9 halamanArticol 1 PDFAna CernaianuBelum ada peringkat
- AAP Parameters of Care Periodontics 9Dokumen3 halamanAAP Parameters of Care Periodontics 9Tanmay JhulkaBelum ada peringkat
- The Following Resources Related To This Article Are Available Online atDokumen10 halamanThe Following Resources Related To This Article Are Available Online atOana DimaBelum ada peringkat
- Premium Day Poster COIR 2013Dokumen28 halamanPremium Day Poster COIR 2013juanBelum ada peringkat
- Risk Factors in Bone Augmentation Procedures: Peter K. Moy - Tara AghalooDokumen15 halamanRisk Factors in Bone Augmentation Procedures: Peter K. Moy - Tara Aghalooxiaoxin zhangBelum ada peringkat
- Timing Orthodontic Treatment Early or LateDokumen9 halamanTiming Orthodontic Treatment Early or LateAnaMariaCastroBelum ada peringkat
- Periodontology 2000 - 2022 - BarootchiDokumen28 halamanPeriodontology 2000 - 2022 - BarootchitzulinBelum ada peringkat
- 4.goals of Full Mouth RehabilitationDokumen8 halaman4.goals of Full Mouth RehabilitationVikas AggarwalBelum ada peringkat
- Growth Considerations in Stability of Orthodontic Treatment: Chapter OutlineDokumen4 halamanGrowth Considerations in Stability of Orthodontic Treatment: Chapter OutlineHabeeb HatemBelum ada peringkat
- The Application of OcclusionDokumen11 halamanThe Application of OcclusionM. ADIL ZaheerBelum ada peringkat
- Australian Dental Journal - 2008 - Santosa - Provisional Restoration Options in Implant DentistrDokumen9 halamanAustralian Dental Journal - 2008 - Santosa - Provisional Restoration Options in Implant DentistrNamratha UmeshBelum ada peringkat
- Clinical Considerations For Increasing Occlusal Vertical Dimension A ReviewDokumen9 halamanClinical Considerations For Increasing Occlusal Vertical Dimension A Reviewinibuatdaftar101Belum ada peringkat
- Ret and RelapseDokumen78 halamanRet and RelapseDeepshikha MandalBelum ada peringkat
- Retention and Stability: A Review of The LiteratureDokumen8 halamanRetention and Stability: A Review of The LiteratureLanaBelum ada peringkat
- 1 s2.0 S0300571205001417 MainDokumen11 halaman1 s2.0 S0300571205001417 MaintangroBelum ada peringkat
- E PerioTherapyDokumen5 halamanE PerioTherapyIova Elena-corinaBelum ada peringkat
- E PerioTherapyDokumen5 halamanE PerioTherapyDoni Aldi L. TobingBelum ada peringkat
- FMR OcclusionDokumen10 halamanFMR OcclusionSkAliHassanBelum ada peringkat
- Long-Term Stability After Orthodontic Treatment Remains InconclusiveDokumen2 halamanLong-Term Stability After Orthodontic Treatment Remains InconclusiveHabeeb AL-AbsiBelum ada peringkat
- Opciones de Prótesis Provisionales para Implantes Dentales Siadat2015Dokumen8 halamanOpciones de Prótesis Provisionales para Implantes Dentales Siadat2015solangeBelum ada peringkat
- Ghafari1987 Morees MeshDokumen8 halamanGhafari1987 Morees MeshSAM PRASANTH100% (1)
- Effects Of' Ret Ycling O/y1 Hmetallic - Direct-Bond Orth'odontie BracketsDokumen15 halamanEffects Of' Ret Ycling O/y1 Hmetallic - Direct-Bond Orth'odontie BracketsSAM PRASANTHBelum ada peringkat
- Janson2007 PDFDokumen9 halamanJanson2007 PDFSAM PRASANTHBelum ada peringkat
- Effects Of' Ret Ycling O/y1 Hmetallic - Direct-Bond Orth'odontie BracketsDokumen15 halamanEffects Of' Ret Ycling O/y1 Hmetallic - Direct-Bond Orth'odontie BracketsSAM PRASANTHBelum ada peringkat
- Bimaxillary Dentoalveolar Protrusion Traits andDokumen7 halamanBimaxillary Dentoalveolar Protrusion Traits andSAM PRASANTHBelum ada peringkat
- Rogelio P. Nogales Et Al vs. CMC, Dr. Oscar Estrada Et Al - gr142625Dokumen5 halamanRogelio P. Nogales Et Al vs. CMC, Dr. Oscar Estrada Et Al - gr142625Dani EsequeBelum ada peringkat
- 1955 Ball LauraDokumen55 halaman1955 Ball LauraBene BeanBelum ada peringkat
- Fetal EchocardiographyDokumen3 halamanFetal EchocardiographypolygoneBelum ada peringkat
- Clinton Valerio Informative Full-Sentence Speech OutlineDokumen4 halamanClinton Valerio Informative Full-Sentence Speech Outlineapi-325211358Belum ada peringkat
- E-Learning,, ,: Key WordsDokumen8 halamanE-Learning,, ,: Key WordsMaria MariaBelum ada peringkat
- Water Quality at Residential and Industrial AreaDokumen11 halamanWater Quality at Residential and Industrial AreaMohamad AizanBelum ada peringkat
- LEEDEN Basic 사용재료 - 23-10-30Dokumen28 halamanLEEDEN Basic 사용재료 - 23-10-30이상민Belum ada peringkat
- Advance Directive FormDokumen21 halamanAdvance Directive FormCommunityBridgesBelum ada peringkat
- ContentsDokumen19 halamanContentsdurairaj1977Belum ada peringkat
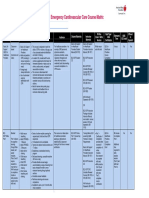
- Emergency Cardiovascular Care Course MatrixDokumen15 halamanEmergency Cardiovascular Care Course MatrixJesus M. Espinosa EchavarriaBelum ada peringkat
- HSS 1101 - FINAL NotesDokumen40 halamanHSS 1101 - FINAL NotesDARCY HAYDENBelum ada peringkat
- What To Know About General AnesthesiaDokumen8 halamanWhat To Know About General AnesthesiaPADAYON MEDISINABelum ada peringkat
- Necrotic Enteritis in ChickensDokumen3 halamanNecrotic Enteritis in ChickensHendra PranotogomoBelum ada peringkat
- Rehydration, Hangover and Vitamin TherapyDokumen2 halamanRehydration, Hangover and Vitamin TherapyKadek SeptiawanBelum ada peringkat
- Lecture 9 Reading Assignment 2Dokumen9 halamanLecture 9 Reading Assignment 2Dennis KorirBelum ada peringkat
- Therapeutic Interventions Part I Rubberbands NowDokumen8 halamanTherapeutic Interventions Part I Rubberbands NowAnna Purna100% (1)
- Fin e 171 2014 PDFDokumen66 halamanFin e 171 2014 PDFRenugopalBelum ada peringkat
- SKINNER: Behavioral Analysis: Characteristics of ScienceDokumen5 halamanSKINNER: Behavioral Analysis: Characteristics of ScienceRustumme Mirelle ReyesBelum ada peringkat
- Herpes Simplex Oral: EpidemiologyDokumen5 halamanHerpes Simplex Oral: EpidemiologyFariz RamadhanBelum ada peringkat
- Presentation of DR Archana Trivedi, One of Co-Authors of Study On Mhealth and TBDokumen11 halamanPresentation of DR Archana Trivedi, One of Co-Authors of Study On Mhealth and TBbobbyramakantBelum ada peringkat
- Clinical Rehabilitation: Goal Attainment Scaling (GAS) in Rehabilitation: A Practical GuideDokumen12 halamanClinical Rehabilitation: Goal Attainment Scaling (GAS) in Rehabilitation: A Practical GuideMarla Constanza Martinez RoseroBelum ada peringkat