Anda mungkin juga menyukai
- Exam For Real Estate in CaliforniaDokumen230 halamanExam For Real Estate in Californiaharpay100% (9)
- What 21st Century LearningDokumen30 halamanWhat 21st Century LearningMarselinus LombeBelum ada peringkat
- DESIGNING A RESEARCH PROJECT TitleDokumen26 halamanDESIGNING A RESEARCH PROJECT TitleShannen GestiadaBelum ada peringkat
- Research Main Aspects: Usama Bin Iqbal Lecture # 4 Qualitative Research TechniquesDokumen41 halamanResearch Main Aspects: Usama Bin Iqbal Lecture # 4 Qualitative Research TechniquesFaisal RazaBelum ada peringkat
- The Philippine Professional Standards For School Heads (PPSSH) IndicatorsDokumen11 halamanThe Philippine Professional Standards For School Heads (PPSSH) Indicatorsjahasiel capulongBelum ada peringkat
- ScientificWriting Jaka WidadDokumen48 halamanScientificWriting Jaka WidadrofiBelum ada peringkat
- Senior Project OutlineDokumen14 halamanSenior Project OutlineAkatew Haile MebrahtuBelum ada peringkat
- Concept MappingDokumen39 halamanConcept MappingRaquel M. Mendoza100% (2)
- Clinical Reasoning FormDokumen4 halamanClinical Reasoning FormgursangeetBelum ada peringkat
- Science Fair Final Report TemplateDokumen2 halamanScience Fair Final Report Templateapi-110202130Belum ada peringkat
- PRactical-Research-2 LM1 NuñezaDokumen18 halamanPRactical-Research-2 LM1 NuñezaJhel Sabatin100% (1)
- SeminarDokumen2 halamanSeminarYedu KrishnaBelum ada peringkat
- Progress Test Files 1-6 Answer Key A Grammar, Vocabulary, and PronunciationDokumen8 halamanProgress Test Files 1-6 Answer Key A Grammar, Vocabulary, and PronunciationEva Barrales0% (1)
- Fhum Ug 2023Dokumen405 halamanFhum Ug 2023Lusanda MbathaBelum ada peringkat
- Nursing Judgment CapstoneDokumen6 halamanNursing Judgment Capstoneapi-591870673Belum ada peringkat
- Nurs 605 Learning Contract Final Copy For Submission April 21Dokumen10 halamanNurs 605 Learning Contract Final Copy For Submission April 21api-323169345Belum ada peringkat
- Reference How To Do The Critical ReviewDokumen5 halamanReference How To Do The Critical ReviewSevi Zakiyyah PutriBelum ada peringkat
- Centre For Air and Space Law Nalsar University of Law, Hyderabad Purpose of Project WritingDokumen7 halamanCentre For Air and Space Law Nalsar University of Law, Hyderabad Purpose of Project WritingSanketBelum ada peringkat
- Nurs 605 Journal Entry 2 Final For SubmissionDokumen6 halamanNurs 605 Journal Entry 2 Final For Submissionapi-323169345Belum ada peringkat
- How To Write A Scientific Literature Review - Publishing in The Sciences - Research Guides at University of Michigan LibraryDokumen3 halamanHow To Write A Scientific Literature Review - Publishing in The Sciences - Research Guides at University of Michigan LibraryKusumitha S 16BBT0188100% (1)
- Charles H. Kahn (Auth.), Simo Knuuttila, Jaakko Hintikka (Eds.) The Logic of Being - Historical StudiesDokumen310 halamanCharles H. Kahn (Auth.), Simo Knuuttila, Jaakko Hintikka (Eds.) The Logic of Being - Historical StudiesAnonymous btcgV68sDP100% (2)
- PHI105.T6 - Persuasive Essay Peer Review WorksheetDokumen4 halamanPHI105.T6 - Persuasive Essay Peer Review WorksheetMark An Christin HaleBelum ada peringkat
- Alternative Capstone ProposalDokumen1 halamanAlternative Capstone ProposaldpanteBelum ada peringkat
- Chapter III - Sampling For ResearchDokumen24 halamanChapter III - Sampling For ResearchSrinadh NaikBelum ada peringkat
- Hewitt Nurs3020 MidtermevalDokumen6 halamanHewitt Nurs3020 Midtermevalapi-301240348Belum ada peringkat
- How To Write A Review of A Scholarly ArticleDokumen1 halamanHow To Write A Review of A Scholarly Articleapi-463969879Belum ada peringkat
- Research MethodsDokumen54 halamanResearch MethodsEyasu Desta100% (1)
- Educ761 Istc685 Syllabus082615Dokumen6 halamanEduc761 Istc685 Syllabus082615api-320617015Belum ada peringkat
- Writing Lab Reports and Scientific Papers: by Warren D. Dolphin Iowa State UniversityDokumen5 halamanWriting Lab Reports and Scientific Papers: by Warren D. Dolphin Iowa State UniversityMariana Muguerza100% (1)
- How To Review A Scientific PaperDokumen4 halamanHow To Review A Scientific PapermunierBelum ada peringkat
- Educ761 Istc685 Syllabus012919Dokumen6 halamanEduc761 Istc685 Syllabus012919api-320617015Belum ada peringkat
- PHI 445 Week 5 Final Project Argumentative EssayDokumen2 halamanPHI 445 Week 5 Final Project Argumentative Essayrollinsandrew0% (1)
- Genre AnalysisDokumen3 halamanGenre Analysisjrgoris9Belum ada peringkat
- To Explain What Is Meant by "Playing God" in This Case.)Dokumen3 halamanTo Explain What Is Meant by "Playing God" in This Case.)Hieu NguyenBelum ada peringkat
- Mco 03 em PDFDokumen8 halamanMco 03 em PDFFirdosh Khan80% (5)
- Symposium ConferenceDokumen8 halamanSymposium Conferencerydham BhatiaBelum ada peringkat
- The Structure of Academic TextsDokumen7 halamanThe Structure of Academic TextsMark Púgnit BonábonBelum ada peringkat
- Fluids Mechanics Lab PrefaceDokumen29 halamanFluids Mechanics Lab PrefaceYesar Bin Mustafa Almaleki50% (2)
- AMJ Publishing CriteriaDokumen24 halamanAMJ Publishing CriteriaLogistics teamBelum ada peringkat
- Framework Adapted From Writing Today, 4th EditionDokumen2 halamanFramework Adapted From Writing Today, 4th EditionKim LaceyBelum ada peringkat
- Common Gotchas in HEP Thesis WritingDokumen11 halamanCommon Gotchas in HEP Thesis WritingAndy Buckley100% (8)
- Challenges of ReadingDokumen52 halamanChallenges of Readingestefany TorresBelum ada peringkat
- Research QuestionDokumen6 halamanResearch QuestionAlfian Ardhiyana PutraBelum ada peringkat
- Develop A Research ProposalDokumen11 halamanDevelop A Research ProposalMonic Romero100% (1)
- Chapter 1: The Uses of Social Research Methods: Learning ObjectivesDokumen5 halamanChapter 1: The Uses of Social Research Methods: Learning Objectiveskamran shafaqatBelum ada peringkat
- PHYb56 F12Dokumen5 halamanPHYb56 F12Apoorva RajBelum ada peringkat
- RES320 - Preisinger, Carrie FINAL EXAMDokumen5 halamanRES320 - Preisinger, Carrie FINAL EXAMCarrie Preisinger100% (1)
- Methods 169 Syllabus Fall 2014Dokumen8 halamanMethods 169 Syllabus Fall 2014buddhaBelum ada peringkat
- Critical Appraisal of JournalDokumen25 halamanCritical Appraisal of JournalPrabhu AypaBelum ada peringkat
- UT Dallas Syllabus For Mas6v02.001.09s Taught by Orlando Richard (Pretty)Dokumen28 halamanUT Dallas Syllabus For Mas6v02.001.09s Taught by Orlando Richard (Pretty)UT Dallas Provost's Technology GroupBelum ada peringkat
- SQUIREdownloadabletemplateDokumen4 halamanSQUIREdownloadabletemplateAmisha Vastani100% (1)
- Checklist For Controlled TrialsDokumen3 halamanChecklist For Controlled TrialsFreddy Dinata100% (1)
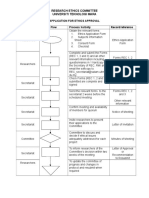
- Research Ethics Committee Universiti Teknologi MaraDokumen2 halamanResearch Ethics Committee Universiti Teknologi Maraamber ariaBelum ada peringkat
- What Is An Expository Essay?Dokumen3 halamanWhat Is An Expository Essay?mmendizabal100% (1)
- UT Dallas Syllabus For Psy3331.5u1.08u Taught by Karen Huxtable-Jester (kxh014900)Dokumen14 halamanUT Dallas Syllabus For Psy3331.5u1.08u Taught by Karen Huxtable-Jester (kxh014900)UT Dallas Provost's Technology GroupBelum ada peringkat
- ENG2DE Outline 2012-2013Dokumen5 halamanENG2DE Outline 2012-2013Danika BarkerBelum ada peringkat
- Description of The Patient & Instructions To SimulatorDokumen9 halamanDescription of The Patient & Instructions To SimulatorsarfirazBelum ada peringkat
- Embraced by The NeedleDokumen2 halamanEmbraced by The NeedleAdv Sandeep SinghBelum ada peringkat
- Steps in Writing Literature ReviewDokumen9 halamanSteps in Writing Literature Reviewm0d1p1fuwub2100% (1)
- ENG 4C OutlineDokumen4 halamanENG 4C OutlineDanika BarkerBelum ada peringkat
- Research Methods Course Article ReviewDokumen3 halamanResearch Methods Course Article Reviewsamia100% (1)
- Q1. What Is Emotional Intelligence? Explain Goleman's Model of Emotional IntelligenceDokumen22 halamanQ1. What Is Emotional Intelligence? Explain Goleman's Model of Emotional IntelligenceRaven MikhailBelum ada peringkat
- Guidelines For DPT Case StudyDokumen7 halamanGuidelines For DPT Case StudyHello RainbowBelum ada peringkat
- Reviewing An AppraisalDokumen9 halamanReviewing An AppraisalroshansamarawickremaBelum ada peringkat
- Commentary: Dr. Brian BudgellDokumen6 halamanCommentary: Dr. Brian Budgellsolstar1008Belum ada peringkat
- Mas For SarahDokumen3 halamanMas For Sarahapi-224606598100% (2)
- First Term Exam ms1Dokumen2 halamanFirst Term Exam ms1Aryam HannachiBelum ada peringkat
- Effects of Violent Online Games To Adolescent AggressivenessDokumen20 halamanEffects of Violent Online Games To Adolescent AggressivenesssorceressvampireBelum ada peringkat
- Motivation LTRDokumen1 halamanMotivation LTREhtesham UddinBelum ada peringkat
- Writing Lesson PlanDokumen3 halamanWriting Lesson Planapi-252918385Belum ada peringkat
- Module 8-4 Legacy of The RenaissanceDokumen3 halamanModule 8-4 Legacy of The RenaissanceClayton BlaylockBelum ada peringkat
- Interview Different TypesDokumen2 halamanInterview Different Typesআলটাফ হুছেইনBelum ada peringkat
- Tutorial Letter FMM3701-2022-S2Dokumen11 halamanTutorial Letter FMM3701-2022-S2leleBelum ada peringkat
- Chap 1 5 Descartes A 1Dokumen72 halamanChap 1 5 Descartes A 1jeric ballezaBelum ada peringkat
- Annual Report 2010Dokumen72 halamanAnnual Report 2010Yan-Lin Jubi LeeBelum ada peringkat
- Liver Disease Management & TransplantDokumen4 halamanLiver Disease Management & TransplantMusike TeckneBelum ada peringkat
- Esm2e Chapter 14 171939Dokumen47 halamanEsm2e Chapter 14 171939Jean HoBelum ada peringkat
- B. Ed Final Prospectus Autumn 2019 (16-8-2019) PDFDokumen41 halamanB. Ed Final Prospectus Autumn 2019 (16-8-2019) PDFbilal1294150% (4)
- Case Study - Kettering UniversityDokumen2 halamanCase Study - Kettering UniversitymajortayBelum ada peringkat
- B.ed NotesDokumen17 halamanB.ed Notesanees kakarBelum ada peringkat
- Level 5 Management and Leadership Qualification GuideDokumen2 halamanLevel 5 Management and Leadership Qualification Guidekim.taylor57430% (1)
- MapehDokumen8 halamanMapehBilly Jane MadrigalBelum ada peringkat
- Modern Labor Economics: Inequality in EarningsDokumen37 halamanModern Labor Economics: Inequality in EarningssamuelBelum ada peringkat
- Reyes Tag Ppt-PrefinalsDokumen11 halamanReyes Tag Ppt-PrefinalsRaphaella Mae Alegre ReyesBelum ada peringkat
- Felipe Padilla de LeonDokumen4 halamanFelipe Padilla de LeonJingky SallicopBelum ada peringkat
- 2022 Book PrimaryAndSecondaryEducationDuDokumen467 halaman2022 Book PrimaryAndSecondaryEducationDuFRANCISCA INDIRA CABRERA ARAYABelum ada peringkat
- SJG - DAE - Questioning Design - Preview PDFDokumen25 halamanSJG - DAE - Questioning Design - Preview PDFJulián JaramilloBelum ada peringkat
- Description: Tags: 1101FederalSchoolCodeListDokumen152 halamanDescription: Tags: 1101FederalSchoolCodeListanon-992356Belum ada peringkat
- PDF Hope 4 Module 3 - CompressDokumen9 halamanPDF Hope 4 Module 3 - CompressJaymark LigcubanBelum ada peringkat