H2288 Full
Diunggah oleh
csrpirataJudul Asli
Hak Cipta
Format Tersedia
Bagikan dokumen Ini
Apakah menurut Anda dokumen ini bermanfaat?
Apakah konten ini tidak pantas?
Laporkan Dokumen IniHak Cipta:
Format Tersedia
H2288 Full
Diunggah oleh
csrpirataHak Cipta:
Format Tersedia
Am J Physiol Heart Circ Physiol 300: H2288H2299, 2011.
First published April 1, 2011; doi:10.1152/ajpheart.00140.2011.
Effect of dietary omega-3 fatty acids on the heart rate and the heart rate
variability responses to myocardial ischemia or submaximal exercise
George E. Billman1,2 and William S. Harris3
1
Department of Physiology and Cell Biology, 2Davis Heart and Lung Research Institute, Ohio State University, Columbus,
Ohio, and 3Sanford Research Institute, University of South Dakota, Sioux Falls, South Dakota
Submitted 9 February 2011; accepted in final form 24 March 2011
Billman GE, Harris WS. Effect of dietary omega-3 fatty acids nists could improve cardiac vagal regulation and, as a conse-
on the heart rate and the heart rate variability responses to myo- quence, would also reduce the incidence of sudden cardiac
cardial ischemia or submaximal exercise. Am J Physiol Heart Circ death in myocardial infarction patients (14, 19). However,
Physiol 300: H2288 H2299, 2011. First published April 1, 2011;
Downloaded from http://ajpheart.physiology.org/ by 10.220.33.6 on August 18, 2017
doi:10.1152/ajpheart.00140.2011.The consumption of omega-3
these interventions failed to prevent ventricular fibrillation
polyunsaturated fatty acids (n-3 PUFAs) has been reported to decrease induced by myocardial ischemia (23, 29) despite significant
resting heart rate (HR) and increase heart rate variability (HRV). increases in resting time and frequency domain markers of
However, the effects of n-3 PUFAs on these variables in response to heart rate variability (HRV; indexes of cardiac parasympathetic
a physiological stress (e.g., exercise or acute myocardial ischemia), regulation; Refs. 2, 48). It was subsequently shown that low
particularly in postmyocardial infarction (MI) patients, are unknown. doses of atropine did not alter the cardiac autonomic response
Therefore, HR and HRV (high frequency and total R-R interval elicited by either submaximal exercise or acute myocardial
variability) were evaluated at rest, during submaximal exercise, and
during a 2-min coronary artery occlusion at rest and before and 3 mo ischemia (23). Thus the search for effective interventions that
after n-3 PUFA treatment in dogs with healed MI (n 59). The dogs improve autonomic balance both at rest and during stress
were randomly assigned to either placebo (1 g/day corn oil, n 19) condition remains elusive.
or n-3 PUFA supplement (docosahexaenoic acid eicosapentaenoic A number of experimental and clinical studies report that
acid ethyl esters; 1 g/day, n 6; 2 g/day, n 12; or 4 g/day, n 22) dietary omega-3 polyunsaturated fatty acids (n-3 PUFAs; Ref.
groups. The treatment elicited significant (P 0.01) dose-dependent 16) or the acute intravenous administration (9) of these lipids
increases in right atrial n-3 PUFA levels but dose-independent reduc- can both lower resting heart rate (HR) and increase resting
tions in resting HR and increases in resting HRV. In contrast, n-3
PUFAs did not attenuate the large changes in HR or HRV induced by HRV, data consistent with an enhanced baseline cardiac para-
either the coronary occlusion or submaximal exercise. These data sympathetic tone. It has been proposed that the cardiovascular
demonstrate that dietary n-3 PUFA decreased resting (i.e., preexercise benefits ascribed to dietary n-3 PUFAs could result, at least in
or preocclusion) HR and increased resting HRV but did not alter the part, from these reductions in HR and the corresponding
cardiac response to physiologic challenges. putative improvements in cardiac autonomic balance (16).
parasympathetic nervous system; exercise; fish oil; docosahexaenoic However, this concept has been challenged (11, 22, 24) and, to
acid; eicosapentaenoic acid date, the effects of dietary n-3 PUFA on HR and HRV during
physiological stress have received little attention. In a similar
manner, several lines of evidence suggest that the modulation
ALTERATIONS IN CARDIAC AUTONOMIC regulation have been impli-
of cardiac autonomic function may not be solely responsible
cated in an increased risk for sudden cardiac death (5). In for the n-3 PUFA-induced reductions in HR. For example, the
particular, reduced cardiac parasympathetic activity coupled acute application of n-3 PUFA reduced the contraction rate of
with an enhanced sympathetic activation in both patients and neonatal rat myocyte cultures (31) while dietary n-3 PUFA
animals following myocardial infarction is associated with an
supplements decreased HR of isolated rat atria (33) and cardiac
increased incidence of malignant ventricular tachyarrhythmias
transplant patients (25). A reduced pacemaker current (If)
and sudden cardiac death (5). Therefore, considerable effort
has been expended in the search for therapeutic interventions density has also been recorded in sinus nodal myocytes from
that improve cardiac balance and could thereby protect against rabbits fed n-3 PUFAs compared with cells from the hearts of
sudden death in high-risk patient populations. animals given similar amounts of sunflower oil (50). However,
To be effective, these interventions must not only improve whether these changes in intrinsic pacemaker rate are main-
baseline or resting cardiac autonomic balance but also maintain tained during physiological stress also remains to be deter-
these changes when the heart is challenged by a physiologic mined.
stress such as acute myocardial ischemia or exercise. For It was, therefore, the purpose of the present study to
example, low doses of cholinergic muscarinic antagonists (at- evaluate the effects of dietary n-3 PUFAs (1 4 g/day for 3
ropine or scopolamine) have, paradoxically, been shown to mo) on the HR and the HRV responses to physiological
enhance resting cardiac vagal regulation in both humans (14, stressors [exercise (submaximal exercise, assessed at its
19, 32) and animals (23, 29). It was therefore proposed that the onset and at its termination) and acute myocardial ischemia
continuous administration of low doses of muscarinic antago- (2-min coronary artery occlusion)] in dogs with healed
myocardial infarctions. In particular, the hypothesis that the
Address for reprint requests and other correspondence: G. E. Billman, Dept.
dietary n-3 PUFA-mediated reductions in HR and increases
of Physiology and Cell Biology, Ohio State Univ., 304 Hamilton Hall, 1645 in HRV would be maintained during a physiologic challenge
Neil Ave., Columbus, OH 43210-1218 (e-mail: billman.1@osu.edu). was tested.
H2288 0363-6135/11 Copyright 2011 the American Physiological Society http://www.ajpheart.org
n-3 FATTY ACIDS INCREASE HRV AT REST BUT NOT DURING METABOLIC STRESS H2289
METHODS 4.8 kph at 0% grade. The speed was then increased to 6.4 kph, and the
grade was increased every 3 min (0, 4, 8, 12, and 16%). The
All the animal procedures were approved by the Ohio State Uni- submaximal exercise test was repeated three times (1/day). On a
versity Institutional Animal Care and Use Committee and conformed subsequent day, with the dogs lying quietly unrestrained on a table, a
to the Guide for the Care and Use of Laboratory Animals published 2-min left circumflex coronary occlusion was made. Left circumflex
by the US National Institutes of Health (NIH publication no. 85-23, blood flow, HR, and HRV were monitored continuously throughout
revised 1996). the exercise or occlusion studies. The submaximal exercise and the
Surgical Preparation coronary occlusion at rest studies were performed both before and
after 3 mo of treatment with either placebo (1 g/day corn oil) or daily
A timeline for the studies may be found in Fig. 1. Eighty heart- n-3 PUFA capsules (1 4 g/day).
worm free mixed breed dogs (2- to 3-yr-old male, n 21, and female,
n 59) weighing 19.3 0.2 kg (range: 13.6 25.9 kg) that were part Dietary Omega-3 Polyunsaturated Fatty Acid Protocol
of an ongoing investigation of the cardiovascular effects of dietary n-3
PUFA (11) were used in this study. The animals were anesthetized The dogs were place on a diet that did not contain any n-3 PUFAs
and instrumented to measure a ventricular electrogram (from which (Harlan Teklad; Harlan Laboratories, Indianapolis, IN) beginning 1
HR and HRV were subsequently determined) and left circumflex wk before the instrumentation surgery and were maintained on this
Downloaded from http://ajpheart.physiology.org/ by 10.220.33.6 on August 18, 2017
coronary artery blood flow as previously described (3, 11). A hydrau- diet until the end of the study (4 mo). After the pretreatment data
lic vascular occluder (model OC3; In Vivo Metric, Healdsburg, collection (3 4 wk after the surgery) had been collected, the dogs
CA) was placed around the left circumflex coronary artery and were then randomly assigned to the following groups: placebo (n
used to induce acute myocardial ischemia for the coronary occlu- 19, 3 male and 16 female); 1 g/day n-3 PUFA (n 6, all female); 2
sion experiments described below (see HRV Protocols). The left g/day n-3 PUFA (n 12, 7 male and 5 female); 4 g/day n-3 PUFA
anterior descending coronary artery was also isolated during the (n 22, 4 male and 18 female); and sham 4 g/day sham (n 6, 1
instrumentation surgery, and a two-stage occlusion of this artery male and 5 females). The dogs were given supplements similar to
was then performed approximately one-third the distance from its those used in the GISSI-Prevenzione study (20). The n-3 PUFA group
origin to produce an anterior wall myocardial infarction (16% of received 465 mg ethyl eicosapentaenoate (EPA) 375 mg ethyl
left ventricular mass; Ref. 3). This vessel was partially occluded docosahexaenoate (DHA) (375 per capsule; Lovaza; GlaxoSmithK-
for 20 min and then tied off. Similar instrumentation surgery was line, Research Triangle Park, NC). The placebo was corn oil (1 g, 58%
performed on six additional sham infarction dogs (i.e., the left linoleic acid 28% oleic acid). The capsules were given per os before
anterior descending artery was isolated but not ligated). The dogs the daily feeding (between 8:00 and 10:00 AM each day, 7 days per
were given analgesic, antibiotic, and anti-arrhythmic therapy to wk for 3 mo).
alleviate postoperative pain, to prevent postoperative infection, and
to reduce acute arrhythmias associated with the myocardial infarc- Red Blood Cell and Cardiac Tissue Fatty Acid Analysis
tion as has been previously described (3, 11). Fasting blood samples (5 ml) were drawn into EDTA tubes from a
HRV Protocols cephalic vein between 8:00 and 9:00 AM 1 day before the initiation of
the treatment (placebo or n-3 PUFA) and when tissue was harvested
HRV was calculated using a Delta-Biometrics vagal tone monitor at the end of the study (14 wk after the treatment began). Right atrial
triggering off the ECG R-R interval (Urbana, Champaign, IL). This and left ventricular tissues were obtained when the hearts were
device employs the time-series signal processing techniques as devel- harvested; the tissue and red blood cells (RBC) were flash frozen in
oped by Porges to estimate the amplitude of respiratory sinus arrhyth- liquid nitrogen and stored at 80C for future analysis.
mia [the high frequency (HF) component of R-R interval variability; RBC and phospholipids from cardiac tissue were analyzed for fatty
Ref. 42]. Details of this analysis have been described previously (6, acid composition using previously described techniques (12, 35). The
28). Data were averaged over 30-s intervals either during exercise or samples were analyzed by gas chromatography using a GC2010-FID
the coronary occlusion. The following indexes of HRV were deter- (Shimadzu, Columbia, MD) equipped with a 100-mm capillary col-
mined: vagal tone index, the HF (0.24 to 1.04 Hz) component of R-R umn (SP-2560; Supelco, Bellefonte, PA). Fatty acids of interest were
interval variability, and standard deviation (SD) of the R-R intervals identified by comparison with known standards and expressed as a
(a marker of total variability) for the same 30-s time periods. percentage of total fatty acids. The coefficient of variation for the
The studies began 3 4 wk after the production of the myocardial RBC EPA DHA assays was 5%.
infarction. Fifteen (18.8%, 6 males, 9 females) died within 72 h of the
myocardial infarction, and reliable ECG recordings could not be Data Analysis
obtained in six dogs (1 male and 5 females). Thus HRV studies were
completed on 59 (14 male and 45 female) dogs following the myo- All data are reported as means SE. The data were digitized (1
cardial infarction and all six sham-operated dogs. First, over the kHz) and recorded using a Biopac MP-100 data acquisition system
period of 35 days, the dogs learned to run on a motor-driven (Biopac Systems, Goleta, CA). The HR and HRV data were averaged
treadmill. The cardiac response to submaximal (i.e., 60 70% of over 30-s intervals either during exercise or the coronary occlusion.
maximal HR) exercise was then evaluated as follows: exercise lasted The following time points were evaluated for the exercise trials: the
a total of 18 min with workload increasing every 3 min. The protocol last 30 s before the onset of exercise, from 0 to 30 s, from 30 to 60 s,
began with a 3-min warm-up period, during which the dogs ran at and from 90 to 120 s after exercise onset; and for recovery from
exercise: the last 30 s of exercise, from 0 to 30 s, from 30 to 60 s, and
from 90 to 120 s after the termination of exercise. The values averaged
over these time periods are reported as time 0, 30, 60, and 120 s,
respectively. ECG variables were averaged over the last five beats
before and 60 s after the onset of the coronary occlusion. QT interval
was corrected for changes in HR using Van de Waters correction
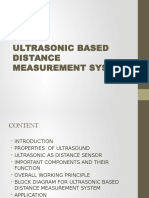
Fig. 1. Study timeline. Pre- and posttreatment data collection studies consist of formula [QTc QT-87(60/HR-1)] (49).
the following: three submaximal exercise studies and one 2-min coronary The data were compared using ANOVA for repeated measures
artery occlusion at rest. Studies were performed at least 24 h apart. MI, (NCSS Statistical Software, Kaysville, UT). For example, the effects
myocardial infarction. the n-3 PUFAs on resting HR and HRV were analyzed using a
AJP-Heart Circ Physiol VOL 300 JUNE 2011 www.ajpheart.org
H2290 n-3 FATTY ACIDS INCREASE HRV AT REST BUT NOT DURING METABOLIC STRESS
Table 1. Red blood cell omega-3 polyunsaturated fatty acid content
EPA DHA Omega-3 Index
Pre Post Pre Post Pre Post
Placebo (n 12) 0.16 0.01 0.25 0.04 0.28 0.07 0.32 0.06 0.43 0.08 0.54 0.08
1 g/day (n 6) 0.19 0.02 1.20 0.13* 0.17 0.02 2.15 0.22* 0.36 0.03 3.34 0.26*
2 g/day (n 12) 0.16 0.01 1.71 0.11* 0.29 0.08 2.01 0.13* 0.56 0.13 3.72 0.22*
4 g/day (n 22) 0.20 0.02 3.92 0.21* 0.21 0.03 3.02 0.17* 0.41 0.05 7.11 0.27*
Sham (n 5) 0.24 0.03 4.41 0.48* 0.17 0.02 3.421 0.33* 0.40 0.05 7.49 0.45*
All values are means SE and are expressed as %total lipid content. Sham (i.e., no myocardial infarction) received 4 g/day; EPA eicosapentaenoic acid;
DHA docasahexaenoic acid; omega-3 index EPA DHA. *P 0.01, pre vs. post.
two-way ANOVA [pre-post (2 levels) dose (4 levels)] with re- PUFA doses elicited similar reductions in HR, and increases
peated measures on one factor (pre-post) measures. In a similar HRV such that there were no significant differences noted
Downloaded from http://ajpheart.physiology.org/ by 10.220.33.6 on August 18, 2017
fashion, the effects of n-3 PUFAs on the HR and HRV response to between these treatments (i.e., no significant dose effect: HR,
either submaximal exercise or the coronary artery occlusion at rest P 0.51; HRV: HF, P 0.66, SD, P 0.80 or dose
were analyzed using a three-factor ANOVA [pre-post (2 levels)
dose (placebo vs. n-3 PUFA) time (exercise 7 levels or occlusion
pre-post interaction: HR, P 0.28; HRV: HF, P 0.42, SD,
6 levels) with repeated measures on two factors (pre-post and time)]. P 0.10 ).
The effect of n-3 PUFA on ECG variables before and 60 s after Sham (no infarction) dogs: n-3 PUFA treatment (4 g/day)
coronary occlusion were evaluated using a three factor [pre-post (2 elicited reductions in HR (pre 124.8 6.3 vs. post 103.2
levels), dose (2 levels), and occlusion time (2 levels)] ANOVA with 10.8 beats/min) and increases in HRV (HF: pre 5.2 0.3 vs.
repeated measures on two (pre-post and occlusion time) factors. post 7.2 0.7 ln ms2; SD: pre 40.2 7.2 vs. post 78.4 20.8
Homogeneity of covariance (sphericity assumption, equal correlates ms) that were similar to those induced in the infarcted dogs.
between the treatments) was tested using Mauchleys test and, if Thus n-3 PUFA provoked changes in resting HR and HRV that
appropriate, adjusted using Huynh-Feldt correction. RBC and cardiac were consistent with an enhanced cardiac vagal regulation (2,
tissue lipid compositions were compared using a two-factor ANOVA 48) in both infarcted and noninfarcted animals.
with repeated measures on one factor (pre-post) or a one-factor
ANOVA, respectively. If the F value exceeded a critical value (P
Effect of n-3 PUFA on the ECG Variables, HR, and HRV
0.05), post hoc comparisons of the data were then made using
Tukey-Kramer multiple comparison test. Response to Acute Myocardial Ischemia
As with resting values, each dose of n-3 PUFA elicited
RESULTS
similar changes in the HR and HRV responses to the 2-min
Effect of n-3 PUFA on RBC and Cardiac Tissue Fatty Acid coronary artery occlusion (no significant dose effect: HR, P
Content 0.63; HRV: HF, P 0.54, SD, P 0.10). Therefore, the n-3
PUFA data for all three doses have been combined in the
In agreement with our previous study (11), n-3 PUFA subsequent analyses. The effects of placebo and the n-3 PUFA
supplements elicited a dose-dependent (dose effect, pre-post, treatment on the HR and HRV (HF only) response to the acute
and dose pre-post interaction all; P 106) increases in myocardial ischemia are displayed in Fig. 3, while the effects
RBC membrane EPA, DHA, and the omega-3 index (EPA of the coronary occlusion on ECG variables are listed in
DHA) compared with the placebo-treated animals (Table 1). Table 3. The coronary occlusion provoked significant increases
Thus n-3 PUFA treatment (all 3 doses) increased RBC n-3 in HR (P 106) and the descending portion of the T wave
PUFA content while lipid composition did not change during
the 3-mo study in the placebo-treated dogs. In a similar
manner, cardiac tissue n-3 PUFA content was significantly Table 2. Cardiac tissue omega-3 polyunsaturated fatty acid
higher (P 106, all 3 doses) in n-3 PUFA compared with the content
placebo-treated animals (Table 2).
Omega-3
EPA DHA Index
Effect of n-3 PUFA on Resting HR and HRV
Right atrium
As n-3 PUFA have been reported to elicit different responses placebo (n 12) 0.32 0.11 0.56 0.14 0.85 0.22
in males than in females (17), the effect of gender was first 1 g/day (n 6) 1.24 0.11* 3.38 0.20* 4.63 0.18*
2 g/day (n 12) 1.45 0.23* 2.89 0.41* 4.34 0.64*
evaluated. There were no significant gender differences in HR 4 g/day (n 22) 2.76 0.44* 3.54 0.50* 6.31 0.88*
(P 0.69) or HRV (HF, P 0.91; SD, P 0.30) before or Sham (n 5) 2.80 0.43* 3.83 0.23* 6.63 0.31*
after the 3-mo treatment period. Therefore, these data have Left ventricle
been combined in all subsequent analyses. The effects of placebo (n 12) 0.31 0.06 0.49 0.08 0.80 0.11
placebo and the n-3 PUFA treatment on resting (i.e., obtained 1 g/day (n 6) 1.25 0.09* 3.08 0.17* 4.33 0.21*
2 g/day (n 12) 1.69 0.20* 2.67 0.21* 4.35 0.64*
while the animals were standing waiting for the onset of 4 g/day (n 22) 3.81 0.30* 3.43 0.20* 7.24 0.45*
exercise) HR and HRV are displayed in Fig. 2. HR decreased Sham (n 5) 3.71 0.43* 3.65 0.28* 7.07 0.70*
(pre-post effect, P 0.006) and HRV [either HF, P 0.008,
All values are means SE and are expressed as %total lipid content. Sham
or SD, P 0.0006] increased after 3 mo of treatment while (i.e., no myocardial infarction) received 4 g/day; EPA eicosapentaenoic
these variables did not change during the 3-mo duration of the acid; DHA docasahexaenoic acid; omega-3 index EPA DHA. *P
study in the placebo (P 0.98) treated group. All three n-3 0.01, omega-3 treated vs. placebo.
AJP-Heart Circ Physiol VOL 300 JUNE 2011 www.ajpheart.org
n-3 FATTY ACIDS INCREASE HRV AT REST BUT NOT DURING METABOLIC STRESS H2291
effect, P 106) in the placebo and in the n-3 PUFA-treated
animals. HR was significantly lower (pre-post, P 0.0005),
and both HF (pre-post, P 0.00004) and SD (data not shown
pre-post, P 0.0008) were higher during the coronary occlu-
sion after n-3 PUFA treatment compared with values obtained
before the treatment. However, the absolute change in these
variables induced by myocardial ischemia (HR pretreatment
31.8 4.1 vs. posttreatment 28.1 4.5 beats/min; HF pre
3.6 0.4 vs. post 2.9 0.4 ln ms2; SD pre 43.8 5.1
vs. post 30.3 4.8 ms) was not altered by the n-3 PUFA
treatment (pre-post time interaction: HR, P 0.70; HF, P
0.11; SD, P 0.15). Thus n-3 PUFA treatment elicited a
downward shift in resting HR and an upward shift in the resting
HRV but did not alter the magnitude of the change in these
Downloaded from http://ajpheart.physiology.org/ by 10.220.33.6 on August 18, 2017
variables that was induced by the coronary artery occlusion
(i.e., the response to the coronary occlusion per se was not
affected by the treatment). Similar results were obtained for the
sham n-3 PUFA-treated dogs (data not shown).
In contrast to the results from the n-3 PUFA treatment,
neither HR (pre-post, P 0.83), nor the HF component of R-R
interval variability (pre-post, P 0.20), nor the SD of R-R
interval (pre-post, P 0.14) was different before and at the
end the placebo treatment period. The change in these variables
was also similar before and at the end of the placebo treatment
(pre-post time interaction: HR, P 0.98; HF, P 0.57; SD,
P 0.67).
Effect of n-3 PUFA on the HR and HRV Response to
Submaximal Exercise
As with resting values, each dose of n-3 PUFA elicited
similar changes in the HR and HRV responses to exercise
(no significant dose effect: HR, P 0.88; HRV: HF, P
0.75, SD, P 0.83). Therefore, the n-3 PUFA data for all
three doses have been combined in all subsequent analyses.
As one would predict, exercise provoked large increases in
HR (exercise level effect, P 106) that were accompanied
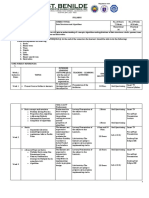
Fig. 2. Effect of increasing doses of dietary omega-3 polyunsaturated fatty by large reductions in HRV (exercise level effect, P
acids (n-3 PUFAs) on baseline heart rate and heart rate variability. Data were
obtained at rest and the last 30 s before the onset of a submaximal exercise test. 106). As these results confirm previous studies (3), these
Vagal tone index is the high frequency component of the R-R interval data are not presented. Rather, the major focus in the sub-
variability (0.24 to 1.04 Hz). SD, standard deviation of the R-R interval; pre, sequent sections has been placed on the analysis of the effects
before placebo or n-3 PUFA treatment began; post, after 3 mo of treatment. of n-3 PUFA treatment on the HR and HRV response to
Placebo (n 19), 1 g/day n-3 PUFA (n 6), 2 g/day n-3 PUFA (n 12), and
4 g/day n-3 PUFA (n 22) are shown. Each 1-g capsule of n-3 PUFA
exercise.
contained 465 mg ethyl eicosapentaenoate (EPA) ethyl docosahexaenoate Submaximal exercise. The HR and HRV response to sub-
(DHA) 375 mg while the placebo contained corn oil (1 g, 58% linoleic acid maximal exercise before and after 3 mo of placebo or n-3
28% oleic acid). *P 0.01, posttreatment vs. the corresponding pretreatment PUFA treatment are displayed in Fig. 4. HR was significantly
values.
lower (HR, pre-post effect P 0.03), and both HF (pre-post
P 0.02) and SD (data not shown pre-post P 0.00004) were
(P 105), a marker of the dispersion of repolarization (41, higher during exercise after n-3 PUFA treatment compared
51) while eliciting decreases in PR interval (P 106). No with values obtained before the treatment. In contrast, neither
other ECG variable was affected by the ischemia. The n-3 HR (pre-post HR, P 0.41) nor the SD of R-R interval
PUFA treatment (but not placebo) elicited significant reduc- (pre-post SD, P 0.62) was altered while HF increased at the
tions in HR (P 0.004) and increases in the PR interval (P end the placebo treatment period (pre-post, P 0.02). The HF
0.0005), changes that were maintained during the coronary increase noted in the placebo-treated animals was similar to
occlusion. Interestingly, preocclusion QTc interval increased in that noted in the n-3 PUFA-treated dogs (i.e., HF were not
both the placebo and n-3 PUFA treatment (P 105) at the significantly different in placebo and n-3 PUFA-treated ani-
end of the 3-mo treatment period compared with values ob- mals, P 0.66) while HR was significantly lower in the n-3
tained before the treatment began. PUFA-treated as compared in the placebo-treated dogs (P
In agreement with previous studies (3, 18), the coronary 0.03). The changes in HR (pre 64.1 4.1 vs. post 63.3 45
occlusion significantly increased HR (occlusion time effect, beats/min) and HF (pre 5.1 0.2 vs. post 5.0 0.2 ln ms2)
P 106) and decreased both indexes of HRV (occlusion time provoked by exercise were not affected by the n-3 PUFA
AJP-Heart Circ Physiol VOL 300 JUNE 2011 www.ajpheart.org
H2292 n-3 FATTY ACIDS INCREASE HRV AT REST BUT NOT DURING METABOLIC STRESS
Downloaded from http://ajpheart.physiology.org/ by 10.220.33.6 on August 18, 2017
Fig. 3. Effect of n-3 PUFAs on the heart rate and heart rate variability response to acute myocardial ischemia (2-min left circumflex coronary artery
occlusion). As there were no significant differences noted between the various n-3 PUFA doses, these data have been combined. Dietary n-3 PUFA, but
not the placebo, produced a significant downward shift of the heart rate response that was accompanied by an upward shift in the high frequency
component of the R-R interval variability (vagal tone index: 0.24 1.04 Hz; i.e., significant pre-post treatment effect). Despite the shifts in the curves, the
absolute change in these variables induced by the occlusion was not altered before or after the treatment (i.e., there was no significant pre-post treatment
ischemia interaction). Placebo (n 15) and n-3 PUFA (1 4 g/day, n 39) are shown. Pre, before treatment began; post, after 3 mo of treatment; C,
control preocclusion; R, recovery postocclusion.
treatment (no significant pre-post exercise level interaction: Exercise onset. The changes (from preexercise levels) in HR
HR, P 0.72; HF, P 0.97). In contrast, exercise elicited a and HRV (HF component) provoked by onset of exercise
significantly (pre-post exercise level interaction P 0.02) before and after 3 mo treatment with either the placebo or n-3
greater reduction in SD; following n-3 PUFA treatment resting PUFA are displayed in Fig. 5. HR was significantly lower (HR,
SD increased (pre 54.4 3.6 vs. post 72.9 5.4 ms) but pre-post effect P 0.04), and both HF (pre-post, P 0.02)
declined to a similar value at the final stage of exercise both and SD (data not shown pre-post, P 0.0002) were higher
before and after the n-3 PUFA treatment (pre 13.2 1.1 vs. during the onset of exercise after n-3 PUFA treatment com-
post 15.6 1.3 ms). Thus n-3 PUFA produced a shift in the pared with values obtained before the initiation of the treat-
preexercise values of HR, HF, and SD that was maintained ment. In contrast, neither HR (pre-post, P 0.27), HF (pre-
throughout the exercise period. This treatment either did not post, P 0.77), nor the SD of R-R interval (pre-post, P
alter (HR and HF) or actually increased (greater change in SD, 0.74) was different before and at the end of the placebo
pre 41.2 3.5 vs. post 57.3 5.0 ms) the magnitude of treatment period. In a similar manner, the change in HR, HF,
the change in these variables that was induced by exercise. In and SD provoked by exercise were not affected by either the
other words, the response to exercise per se was not affected by n-3 PUFA treatment (no significant pre-post exercise level
the treatment. These data suggest that the HR reductions interaction: HR, P 0.39; HF, P 0.16; SD, P 0.10) or the
induced by n-3 PUFA did not result solely from changes in placebo treatment (no significant pre-post exercise: HR, P
cardiac parasympathetic regulation. Similar results were ob- 0.28; HF, P 0.70; and SD, P 0.78). Thus, although n-3
tained for the sham n-3 PUFA-treated dogs. HR was decreased PUFA produced a shift in the baseline (preexercise onset)
and both HF and SD were increased at rest and during exercise values of HR, HF, and SD, this treatment did not alter the
by n-3 PUFA treatment (data not shown). change in these variables induced by the onset of exercise.
AJP-Heart Circ Physiol VOL 300 JUNE 2011 www.ajpheart.org
n-3 FATTY ACIDS INCREASE HRV AT REST BUT NOT DURING METABOLIC STRESS H2293
Table 3. Effect of dietary omega-3 fatty acid on ECG reached before the treatment began). However, the absolute
parameters at rest and during coronary artery occlusion magnitude of the change in HR and HRV provoked by either
exercise or acute myocardial ischemia was not altered by
Pretreatment Posttreatment
n-3 PUFA treatment and was similar to that recorded for the
Control Occlusion Control Occlusion placebo. In other words, the n-3 PUFA treatment produced
Heart rate, beats/ parallel shifts in the response to either exercise or the
min coronary occlusion due to changes in resting (prechallenge)
Placebo 114.8 4.9 154.4 9.7* 115.0 6.0 152.8 11.1* HR and HRV. These data suggest that reductions in intrinsic
n-3 PUFA 122.0 3.5 153.8 5.0* 109.3 3.2 137.3 5.1* pacemaker rate rather than enhanced cardiac parasympa-
PR interval, ms
Placebo 95.1 3.2 83.6 4.1* 100.4 3.4 91.1 3.3* thetic activity may be responsible for the n-3 PUFA-induced
n-3 PUFA 97.2 2.4 87.8 2.5* 104.2 2.3 96.1 2.7* changes in HR. Fourth, a more rapid HR recovery following
QRS duration, ms the termination of exercise was noted after n-3 PUFA
Placebo 80.1 2.7 79.6 2.8 83.7 2.4 82.4 1.7 treatment compared with placebo-treated animals. However,
n-3 PUFA 81.4 1.3 79.2 1.5 82.2 0.9 81.5 1.1
QTc interval, ms
this faster HR recovery was not accompanied by corre-
Downloaded from http://ajpheart.physiology.org/ by 10.220.33.6 on August 18, 2017
Placebo 248.1 4.3 251.3 3.8 270.4 3.7 258.9 3.7 sponding increases in the HF component of R-R interval
n-3 PUFA 254.6 2.4 253.8 2.6 271.3 2.6 265.5 3.0 variability, data that would also suggest that cardiac vagal
Tpeak-Tend regulation was not affected by the n-3 PUFA treatment.
(corrected), ms
Placebo 88.0 3.8 95.4 4.0 88.8 2.9 101.4 5.5*
Finally, similar HR and HRV changes were noted in sham
n-3 PUFA 93.1 2.3 105.4 2.6* 89.2 2.6 105.6 3.2* (noninfarcted animals), and as such, the n-3 PUFA changes
are not restricted to individuals with preexisting cardiac
Values are means SE. Heart rate correction: QTc, QT-87(60/HR-1); damage.
Tpeak-Tend(corrected), Tpeak-Tend-87(60/HR-1) (Ref. 49). *P 0.01, con-
trol vs. coronary artery occlusion (60 s after occlusion onset). P 0.01,
pretreatment vs. posttreatment. Effect of n-3 PUFA on Resting HR and HRV
In agreement with the present study, a number of clinical
Similar results were obtained for the sham n-3 PUFA-treated (1517) and experimental studies (11, 31, 33, 34) report that
dogs (data not shown). n-3 PUFA ingestion or acute intravenous administration (9)
Exercise recovery. The changes in HR and HRV (HF) lower HR and increase HRV, suggestive of an increase in
recovery following the termination of exercise before and after cardiac parasympathetic regulation. The PR interval also in-
3-mo treatment with either the placebo or n-3 PUFA are creased following n-3 PUFA treatment in the present study,
displayed in Fig. 6. Placebo treatment did not affect the data also consistent with a parasympathetically mediated re-
recovery of HR (pre-post, P 0.89), HF (P 0.11), or SD duction in atrioventricular nodal conduction. However, there
(P 0.74) following the termination of exercise. In contrast, are also studies in which n-3 PUFA failed to alter either HRV
HR declined more rapidly (i.e., a faster recovery, HR pre-post or other measures of autonomic function (22, 24, 45), such as
P 0.001) after n-3 PUFA treatment compared with values baroreceptor sensitivity (22). Furthermore, even in the studies
obtained before the initiation of the treatment. The faster HR that reported a positive action of n-3 PUFAs on HR or HRV,
recovery from exercise after n-3 PUFA treatment was accom- the effect was often quite small (36 38). For example, a
panied by a greater increase in SD (pre-post, P 0.001) but meta-analysis of 30 trials found that fish oil supplements (3.5
not HF (pre-post, P 0.10). In a similar manner, absolute g/day of EPA DHA) reduced baseline HR by 2.5 beats/min
change in HR (pre-post time interaction P 0.05) and in SD (38), while Mozaffarian et al. (37) reported that individuals
(pre-post time interaction, P 0.03) following the termi- with the highest fish consumption (5 meals per weak) only
nation of exercise were greater, while HF (no significant exhibited 1.5-ms greater HRV compared with those with the
pre-post time interaction, P 0.99) was not altered by n-3 lowest fish consumption. Although this difference was statis-
PUFA treatment compared with values obtained before n-3 tically significant, such a small change in resting HRV is not
PUFA treatment. Similar results were obtained for the sham likely to be physiologically relevant. Indeed, these investiga-
n-3 PUFA-treated dogs (data not shown). tors calculated that only a 1.1% reduction in the relative risk
DISCUSSION
for sudden cardiac death could be associated with this very
modest increase in HRV (37). However, these small changes
The present study investigated the effects of dietary n-3 could have important consequences if they are maintained
PUFA (1 4 g/day for 3 mo) on HR and HRV both at rest during a physiological stressor such as exercise or acute myo-
(baseline conditions) and during physiological stress (exer- cardial ischemia. Reductions in HR would reduce metabolic
cise or acute myocardial ischemia). The major findings of demand placed on the heart particularly when oxygen supply is
the study are as follows: first, and in agreement with compromised by coronary artery lesions/obstructions. The re-
previous studies (11, 26), the n-3 PUFA treatment elicited sulting better match between oxygen supply and oxygen de-
dose-dependent increases in both RBC and cardiac (right mand would, indirectly, decrease the risk for adverse cardiac
atrial and left ventricular) tissue DHA and EPA content. events associated with myocardial ischemia. In fact, individu-
Second, n-3 PUFA treatment induced reductions in resting als with the lowest resting HRs also exhibited the lowest
HR that were accompanied by increases in HRV. Third, long-term (20 yr) mortality rate (30). Furthermore, the ben-
these changes were maintained during a physiological chal- eficial effects of -adrenergic receptor antagonists, the most
lenge (the peak values obtained during the stimulus were effective anti-arrhythmic medication, have been attributed to
lower after n-3 PUFA treatment compared with values the negative chronotropic actions of these drugs (27).
AJP-Heart Circ Physiol VOL 300 JUNE 2011 www.ajpheart.org
H2294 n-3 FATTY ACIDS INCREASE HRV AT REST BUT NOT DURING METABOLIC STRESS
Downloaded from http://ajpheart.physiology.org/ by 10.220.33.6 on August 18, 2017
Fig. 4. Effect of n-3 PUFAs on the heart rate and heart rate variability response to submaximal exercise. As there were no significant differences noted between
the various n-3 PUFA doses, these data have been combined. Dietary n-3 PUFA, but not the placebo, produced a significant downward shift of the heart rate
response curve that was accompanied by an upward shift in the high frequency component of the R-R interval variability (vagal tone index: 0.24 to 1.04 Hz;
i.e., significant pre-post effect). Despite the shifts in the curves, the absolute change in these variables induced by the exercise was not altered before or after
the treatment (i.e., there was no significant pre-post treatment exercise interaction). Data were averaged over the last 30 s of given exercise level. Exercise
levels were as follows: 1 0 kph and 0% grade; 2 4.8 kph and 0% grade; 3 6.4 kph and 0% grade; 4 6.4 kph and 4% grade; 5 6.4 kph and 8% grade;
6 6.4 kph and 12% grade; 7 6.4 kph and 16% grade. Pre, before placebo (n 16) or n-3 PUFA (1 4 g/day, n 35) treatment began; post, after 3 mo
of treatment.
Effect of n-3 PUFA on HR and Heart Variability Response (due to changes in the preocclusion HR and HRV), but the
to Myocardial Ischemia magnitude of the change in these variables was not altered
by the n-3 PUFA treatment. As the robust autonomic re-
As far as we are aware, the present study provides the first
sponse to the coronary occlusion was not altered, the
description of the effects of dietary n-3 PUFAs on the HR
changes in preischemic HR and HRV induced by the n-3
and HRV response to acute myocardial ischemia in intact
unanesthetized preparations. As expected from previous PUFA may be insufficient to prevent malignant changes in
studies (3, 18), the coronary artery occlusion elicited a the cardiac rhythm. Indeed, the results from the present
robust HR increase that was accompanied by a rapid with- study are analogous to those obtained following treatment
drawal in parasympathetic regulation as indicated by the with low doses of the cholinergic antagonist atropine (23).
decline in both total R-R interval variability (SD) and the With the use of the same canine model of myocardial
HF component of R-R interval variability. However, despite infarction, low-dose atropine decreased baseline HR and
alterations in preocclusion HR and HRV, the cardiac re- increased HRV but, as in the present study, did not alter the
sponse to coronary artery occlusion was not altered by the response to myocardial ischemia (23). This intervention also
n-3 PUFA treatment. The n-3 PUFA treatment produced failed to prevent the induction of ventricular fibrillation
parallel shifts in the coronary occlusion response curves (23). In marked contrast, however, exercise training not only
AJP-Heart Circ Physiol VOL 300 JUNE 2011 www.ajpheart.org
n-3 FATTY ACIDS INCREASE HRV AT REST BUT NOT DURING METABOLIC STRESS H2295
Downloaded from http://ajpheart.physiology.org/ by 10.220.33.6 on August 18, 2017
Fig. 5. Effect of n-3 PUFAs on the change in heart rate and heart rate variability in response to the onset of submaximal exercise. As there were no significant
differences noted between the various n-3 PUFA doses, these data have been combined. As indicated in Fig. 4, dietary n-3 PUFA, but not the placebo, produced
a significant downward shift of the heart rate response that was accompanied by an upward shift in the high frequency component of the R-R interval variability
(vagal tone index: 0.24 1.04 Hz; i.e., significant pre-post treatment effect). Despite the shifts in the curves, the absolute change in these variables induced by
the exercise was not altered before or after the treatment (i.e., there was no significant pre-post treatment exercise onset interaction). Placebo (n 16) and
n-3 PUFA (1 4 g/day, n 35) are shown. Pre, before treatment began; post, after 3 mo of treatment.
improved resting HR and HRV but also dramatically re- the final stage of exercise both before and after the n-3 PUFA
duced the response to coronary occlusion and completely treatment. Interestingly, the HF component of R-R interval
suppressed the formation of malignant ventricular tachyar- variability exhibited a small but significant increase at the end
rhythmias (7). When considered together, these results of the 3-mo placebo period, an increase similar to that noted
strongly suggest that, to be effective, an intervention must after n-3 PUFA treatment. Despite these similar changes in HF,
enhance cardiac parasympathetic regulation during myocar- the HR response to exercise was reduced in n-3 PUFA com-
dial ischemia; resting changes alone may be insufficient to pared with placebo-treated dogs. These data suggest that the
protect against malignant arrhythmias. HR reductions induced by n-3 PUFA did not result solely from
changes in cardiac parasympathetic regulation. In contrast to
Effect of n-3 PUFA on HR and Heart Variability Response these n-3 PUFA findings, an endurance exercise training pro-
to Exercise
gram (10-wk treadmill running) both improved resting HR and
In the present study, dietary n-3 PUFA treatment also HRV and attenuated the cardiac response to submaximal ex-
elicited similar parallel shifts in the HR and HRV in the ercise in the same canine model as was used in the present
exercise HR and HF response curves as was noted during the study (7, 8) .
coronary occlusion. However, exercise elicited a greater reduc- There are relatively few studies that evaluated the effects of
tion in the SD in R-R interval following n-3 PUFA treatment, n-3 PUFA on the response to exercise in humans (13, 39, 40,
and preexercise SD increased but declined to a similar value at 43). In agreement with the present study, dietary fish oil
AJP-Heart Circ Physiol VOL 300 JUNE 2011 www.ajpheart.org
H2296 n-3 FATTY ACIDS INCREASE HRV AT REST BUT NOT DURING METABOLIC STRESS
Downloaded from http://ajpheart.physiology.org/ by 10.220.33.6 on August 18, 2017
Fig. 6. Effect of n-3 PUFAs on the change in heart rate and heart rate variability following the termination of submaximal exercise. As there were no significant
differences noted between the various n-3 PUFA doses, these data have been combined. Heart rate more rapidly declined following the termination of exercise
after the n-3 PUFA but not in the placebo-treated dogs. In contrast to what was noted during exercise onset, the absolute changes in heart rate following the
termination of exercise were greater after dietary n-3 PUFA treatment (i.e., significant pre-post treatment exercise recovery interaction). However, the more
rapid decline in heart rate was not accompanied by an upward shift in the high frequency component of the R-R interval variability (vagal tone index: 0.24 1.04
Hz; i.e., no significant pre-post treatment exercise recovery interaction). Placebo (n 16) and n-3 PUFA (1 4 g/day, n 35) are shown. Pre, before treatment
began; post, after 3 mo of treatment. *Posttreatment vs. the corresponding pretreatment time interval.
supplements (8-wk, 8 g/day) produced HR reductions both at sponses to exercise. Species (dog vs. human) may account for
rest and at peak workload in well-trained men (bicyclists) the seemingly disparate results.
during submaximal exercise (43). In a similar manner, fish oil Analysis of the HR and HRV response to the onset and
(5-wks, 6 g/day) reduced HR during exercise in a group of recovery from exercise can also provide insight into cardiac
Australian rule football players (13). Finally, fish oil supple- autonomic regulation (4, 47). Although preexercise onset HR
ments (12 wk, 6 g/day DHA-rich tuna oil) produced small decreased and HRV increased at the end of the 3-mo n-3 PUFA
reductions in baseline HR and larger reductions in HR with treatment, the changes in these variables that were induced by
increasing workload in sedentary overweight adults (39). Un- exercise onset were similar both before and after treatment. As
like the previous clinical studies (13, 40, 43), these investiga- far as we are aware, no other studies (either in humans or
tors also evaluated the effects of the interventions on HRV animals) have evaluated the effects of n-3 PUFA on the cardiac
(39). The fish oil supplement also increased the HF component response to the onset of exercise. Once again, the findings
of HRV both at rest and during exercise. The changes in HR reported in the present study contrast with the results obtained
and HRV induced by the fish oil supplements were similar to following a 10-wk exercise training program (8). Exercise
those recorded in a group of exercise-trained subjects (39). The training significantly attenuated the increase in HR but did not
authors concluded that fish oil supplements reduced HR and alter the reductions in HRV, elicited by the onset of exercise,
modulated HRV in keeping with an improved parasympathetic- data that suggest that cardiac sympathetic rather than cardiac
sympathetic balance in overweight adults (39). These latter parasympathetic response to exercise onset was reduced fol-
results contrast somewhat with the present study, in that the lowing exercise training (8).
tuna oil supplements induced modest changes in baseline HRV In contrast to the response to exercise onset, n-3 PUFA
and HR but also attenuated both the HR and the HRV re- treatment altered both the HR and SD of R-R interval recovery
AJP-Heart Circ Physiol VOL 300 JUNE 2011 www.ajpheart.org
n-3 FATTY ACIDS INCREASE HRV AT REST BUT NOT DURING METABOLIC STRESS H2297
following termination of exercise. In agreement with human Limitations of the Study
studies (40), HR declined more rapidly (i.e., a faster recovery),
which was accompanied by a greater increase in total R-R In the present study, cardiac vagal nerve activity was not
directly recorded. Cardiac parasympathetic regulation was only
interval variability but not the HF component of this variability
indirectly evaluated using noninvasive markers of HRV. Al-
(an index of cardiac parasympathetic activity) after n-3 PUFA
though a number of studies provide strong evidence that
treatment compared with values obtained before the initiation beat-to-beat fluctuation in HR reflect corresponding changes in
of the treatment. Thus the absolute changes in HR and the SD cardiac parasympathetic regulation (2, 48), an accurate assess-
of R-R interval following the termination of exercise were ment of nerve activity can only be obtained from direct nerve
greater, while the HF component of HRV was not altered by recordings. As such, HRV data should always be interpreted
n-3 PUFA treatment compared with values obtained before n-3 with care. Second, previous studies (10, 11) demonstrate that
PUFA treatment. Since the HF component of R-R interval ventricular function is not altered by myocardial infarction in
variability was not altered by n-3 PUFA treatment, the faster the canine model used in the present study. As such, one might
return to baseline after termination of exercise in the n-3 speculate that the potential benefits of dietary n-3 PUFA on
PUFA-treated animals probably did not result as a consequence cardiac autonomic regulation could be more obvious in indi-
Downloaded from http://ajpheart.physiology.org/ by 10.220.33.6 on August 18, 2017
of a faster reactivation of cardiac parasympathetic activity but viduals with more severe cardiac impairment. To the best of
rather may reflect either changes in the intrinsic pacemaker rate our knowledge, there have not been any studies that have
or cardiac sympathetic activity. evaluated the effects of dietary n-3 PUFA on the HRV re-
sponse to exercise or acute myocardial ischemia in patients
Possible Mechanism of Action with impaired cardiac function. Future investigation will be
required to determine if n-3 PUFA exhibit greater effects in
The mechanisms responsible for the n-3 PUFA-induced these patient populations. Third, selecting an appropriate dose
decreases in HR and increases in HRV were not investigated in can prove to be problematic when comparing across species of
the present study and remain to be determined. However, there different sizes. In the present study, if one adjusts dose by body
are at least two possible explanations for these observations: surface area, then the 1, 2, and 4 g/day dose would be
HR reductions could result from changes in cardiac autonomic equivalent to 1.5, 4.9, and 9.4 g/day in human subjects. As
regulation (enhanced parasympathetic and/or reduced sympa- such, these doses are somewhat higher than the dose (1 g/day)
thetic activity) and/or from alterations in intrinsic pacemaker most commonly used in secondary prevention trials. However,
rate. In the present study, the prechallenge (exercise or coro- doses up to 8 g/day n-3 PUFA have been used to evaluate the
nary occlusion) HF component of the R-R interval variability effect of n-3 PUFA on HRV in human subjects (43). In
increased following 3 mo of n-3 PUFA treatment. Although addition, n-3 PUFA treatment in the present study yielded RBC
there are limitations with this index (2, 28, 42), it is now membrane concentrations within the range that were associated
generally accepted that it can provide an indirect and qualita- with a significant reduction in the risk for sudden cardiac death
tive assessment of cardiac parasympathetic regulation (2, 48). in epidemiological studies (1). Specifically, Albert et al. (1)
As such, the reduction in HR that accompanies n-3 PUFA found that a mean RBC concentration of 6.9% was associated
treatment could reflect an enhanced parasympathetic efferent with a 90% reduction in the risk for sudden death, a value that
compares favorably to that obtained in the present study (after
(either of central or peripheral origin) regulation of the heart.
3 mo, the 4 g/day treatment RBC concentration was 7.1%).
However, as has been noted, both exercise and coronary artery
Finally, although dogs and humans exhibit a similar cardiac
occlusion elicited similar changes in HRV before and after n-3 autonomic regulation (46), species difference could also con-
PUFA treatment. The parallel shifts in the HRV response tribute to responses differences. One must always use caution
curves after n-3 PUFA treatment are more consistent with when extrapolating results between species.
reductions in the intrinsic pacemaker rate than with alterations
in autonomic neural regulation. If parasympathetic activity had Conclusions and Future Directions
been enhanced or sympathetic activity reduced following n-3
PUFA treatment, then one would expect smaller changes in HR In the present study, dietary n-3 PUFA (DHA EPA ethyl
esters, 1 4 g/day for 3 mo) elicited dose-independent reduc-
and HRV during physiological interventions (as was the case
tions in baseline HR that were accompanied by increases in
following endurance exercise training; Refs. 7, 8) rather than
HRV in dogs with and without healed myocardial infarctions.
similar changes as noted in the present study. Furthermore, an
However, n-3 PUFA treatment did not alter the robust auto-
accelerated HR recovery was noted after n-3 PUFA without nomic response (identical increases in HR and decreases in
corresponding changes in HF power. Finally, despite similar HRV before and after treatment) induced by either exercise or,
changes in HRV, the peak HR response to exercise was more importantly, by myocardial ischemia. Furthermore, HR
attenuated in the n-3 PUFA treated but not in the placebo- recovery following exercise was faster after n-3 PUFA without
treated dogs. When considered together, these data suggest that corresponding changes HF power and the peak HR obtained
intrinsic changes in pacemaker rate may play a more important during exercise was lower in n-3 PUFA-treated dogs compared
role in n-3 PUFA-induced HR reductions than do changes in with placebo-treated animals despite similar HRV changes.
cardiac autonomic regulation. Indeed, n-3 PUFA have been When considered together, these data suggest that changes in
recently reported to reduce the pacemaker current (If) in sino- cardiac autonomic regulation are not solely responsible for n-3
atrial node cells obtained from rabbits fed diets enriched with PUFA-induced changes in HR; alterations in the intrinsic
fish oil but not in cells isolated from the hearts of animals fed pacemaker rate also contribute to the chronotropic actions of
sunflower oil (50). these fatty acids.
AJP-Heart Circ Physiol VOL 300 JUNE 2011 www.ajpheart.org
H2298 n-3 FATTY ACIDS INCREASE HRV AT REST BUT NOT DURING METABOLIC STRESS
If n-3 PUFA-induced changes in intrinsic pacemaker rate are 6. Billman GE, Dujardin J. Dynamic changes in cardiac vagal tone as
responsible for (or at least contribute to) the HR reductions measured by time-series analysis. Am J Physiol Heart Circ Physiol 258:
H896 H902, 1990.
associated with this treatment, then one can make several 7. Billman GE, Kukielka M. Effects of endurance exercise training on heart
predictions. In vivo: 1) One would predict that selective an- rate variability and susceptibility to sudden cardiac death: protection is not
tagonists of the pacemaker current (If) should elicit parallel due to enhanced cardiac vagal regulation. J Appl Physiol 100: 896 906,
shifts in the HR response to exercise or coronary occlusion 2006.
8. Billman GE, Kukielka M. Effect of endurance exercise training on the
similar to those noted in the present study. In fact, Zatebradine
heart rate onset and heart rate recovery responses to submaximal exercise
reduced both the resting HR and the HR at the end of each in animals susceptible to ventricular fibrillation. J Appl Physiol 102:
stage of an exercise stress test (21). 2) One would predict that 231240, 2007.
after complete cardiac autonomic neural blockade, HR would 9. Billman GE, Hallaq H, Leaf A. Prevention of ischemia-induced ventric-
be lower in n-3 PUFA treated than in placebo-treated subjects. ular fibrillation by omega-3 fatty acids. Proc Natl Acad Sci USA 91:
44274430, 1994.
If, however, intrinsic rate is not altered by this intervention, 10. Billman GE, Schwartz PJ, Gagnol JP, Stone HL. The cardiac response
then alterations in autonomic regulation could play an impor- to submaximal exercise in dogs susceptible to sudden cardiac death. J Appl
tant role in mediating the HR reduction following n-3 PUFA Physiol 59: 890 897, 1985.
Downloaded from http://ajpheart.physiology.org/ by 10.220.33.6 on August 18, 2017
treatment. In vitro: 3) One would predict a reduced If current 11. Billman GE, Nishijima Y, Belevych AE, Terentyev D, Xu Y, Haizlip
density in sinus nodal myocytes obtained from n-3 PUFA- KM, Monasky MM, Hiranandani N, Harris WS, Gyorke S, Carnes
CA, Janssen PML. Effects of dietary omega-3 fatty acids on ventricular
treated dogs similar to that which has been reported in rabbit function in dogs with healed myocardial infarctions. Am J Physiol Heart
preparations (50). 4) This reduced pacemaker current could Circ Physiol 298: H1219 H1228, 2010.
result from either reduced expression of the pacemaker channel 12. Bligh EG, Dyer WJ. A rapid method for total lipid extraction and
(i.e., reduced HCN protein content) or from the posttransla- purification. Can J Biochem Physiol 37: 911917, 1959.
tional modification of this protein (trafficking, phosphoryla- 13. Buckley JD, Burgess S, Murphy KJ, Howe PRC. DHA-rich fish oil
lowers heart rate during submaximal exercise in elite Australian Rules
tion, oxidation, etc). 5) In contrast, if the HR reduction resulted footballers. J Sci Med Sport 12: 503507, 2009.
from increased parasympathetic activity, then one would ex- 14. Casadei B, Pipillis A, Sessa F, Conway J, Sleight P. Low doses of
pect an increase in the acetylcholine-activated potassium cur- scopolamine increase cardiac vagal tone in the acute phase of myocardial
rent (IK-ach) accompanied by an increased expression of this infarction. Circulation 88: 353357, 1993.
15. Carney RM, Freedland KE, Stein PK, Steinmeyer BC, Harris WS,
channel protein and/or the muscarinic (M2) receptors (and Rubin EH, Krone RJ, Rich WW. Effect of omega-3 fatty acids on heart
associated signaling pathway proteins). The determination of rate variability in depressed patients with coronary heart disease. Psycho-
the relative contribution of putative changes in intrinsic pace- som Med 72: 748 754, 2010.
maker rate and cardiac autonomic regulation to n-3 PUFA- 16. Christensen JH, Schmidt EB. Autonomic nervous system, heart rate
mediated reductions in HR will require further investigation. variability and n-3 fatty acids. J Cardiovasc Med 8, Suppl 1: S19 S22,
2007.
17. Christensen JH, Christensen MS, Dyerberg J, Schmidt EB. Heart rate
ACKNOWLEDGMENTS
variability and fatty acid content in blood cell membranes: a dose-response
We thank Raven Morgan, Anita McKenzie, and Andrew Christianson for study with n-3 fatty acids. Am J Clin Nutr 70: 331337, 1999.
excellent technical assistance during the course of the studies. We also thank 18. Collins MN, Billman GE. Autonomic response to coronary occlusion in
GlaxoSmithKline for generously providing the n-3 PUFA ethyl ester and animals susceptible to ventricular fibrillation. Am J Physiol Heart Circ
placebo capsules for this study. Physiol 257: H1886 H1894, 1989.
19. De Ferrari GM, Mantica M, Vanoli E, Hull SS Jr, Schwartz PJ.
GRANTS Scopolamine increases vagal tone and vagal reflexes in patients after
myocardial infarction. J Am Coll Cardiol 22: 13271334, 1993.
This work was supported by National Heart, Lung, and Blood Institute 20. Di Stasi D, Bernasconi R, Marchioli R, Marfisi RM, Rossi G, Tognoni
Grant HL-086700 (to G. E. Billman). G, Tacconi MT. Early modifications of fatty acid composition in plasma
phospholipids, platelets and mononucleates of healthy volunteers after low
DISCLOSURES doses of n-3 polyunsaturated fatty acids. Eur J Clin Pharmacol 60:
William S. Harris is a scientific advisor to GlaxoSmithKline, Monsanto, and 183190, 2004.
Unilever; a speaker for GlaxoSmithKline; and the owner of OmegaQuant, a 21. Frishman WH, Pepine CJ, Weiss RJ, Baiker WM, for the Zatebradine
company offering blood omega-3 testing. There are no other conflicts to Study Group. Addition of Zatebradine, a direct sinus node inhibitor,
declare. provides no greater exercise tolerance benefit in patients with angina
taking extended-release nifedipine: results of multicenter, randomized
REFERENCES double-blind, placebo-controlled, parallel-group study. J Am Coll Cardiol
26: 305312, 1995.
1. Albert CM, Campos H, Stamfer MJ, Ridker PM, Mason JE, Willet 22. Geelen A, Zock PL, Swenne CA, Brouwer IA, Schouten EG, Katan
WC, Ma J. Blood levels of long-chin n-3 fatty acids and the risk of sudden MB. Effect of n-3 fatty acids on heart rate variability and baroreflex
death. N Engl J Med 346: 11131118, 2002. sensitivity in middle-aged subjects. Am Heart J 146: E4, 2003.
2. Berntson GG, Bigger JT, Eckberg DL, Grossman P, Kaufmann PG, 23. Halliwill JR, Billman GE, Eckberg DL. Effect of a vagomimetic
Malik M, Nagaraja HK, Proges SW, Saul JP, Stone PH, van der atropine dose on canine cardiac vagal tone and susceptibility to sudden
Molen MW. Heart rate variability: origins, methods, and interpretive cardiac death. Clin Auton Res 8: 155164, 1998.
caveats. Pyschophysiology 34: 623648, 1997. 24. Hamaad A, Lee WK, Lip GYH, MacFadyen RJ. Oral omega-3 PUFA
3. Billman GE. A comprehensive review and analysis of 25 years of data therapy (Omacor) has no impact on indices of heart rate variability in
from an in vivo canine model of sudden cardiac death: implications for stable post myocardial infarction patients. Cardiovasc Drug Ther 20:
future anti-arrhythmic drug development. Pharmacol Therap 111: 808 359 364, 2006.
835, 2006. 25. Harris WS, Gonzles M, Laney N, Sastre A, Borkon AM. Effects of
4. Billman GE. Heart rate response to the onset of exercise: evidence for omega-3 fatty acids on heart rate in cardiac transplant recipients. Am J
enhanced cardiac sympathetic activity in animals susceptible to ventricular Cardiol 98: 13931395, 2006.
fibrillation. Am J Physiol Heart Circ Physiol 291: H429 H435, 2006. 26. Harris WS, Sands SA, Windsor SL, Ali HA, Stevens TL, Magalski A,
5. Billman GE. Cardiac autonomic neural remodeling and susceptibility to Porter CB, Borkon AM. Omega-3 fatty acids in cardiac biopsies from
sudden cardiac death: effect of endurance exercise training. Am J Physiol heart transplantation patients: correlation with erythrocytes and response
Heart Circ Physiol 297: H1171H1193, 2009. to supplementation. Circulation 110: 16451649, 2004.
AJP-Heart Circ Physiol VOL 300 JUNE 2011 www.ajpheart.org
n-3 FATTY ACIDS INCREASE HRV AT REST BUT NOT DURING METABOLIC STRESS H2299
27. Held PH, Yusuf S. Effects of beta-blockers and Ca2 channel blockers in responses to exercise in overweight adults. Br J Nutr 100: 10971103,
acute myocardial infarction. Eur Heart J 14, Suppl F: 18 25, 1993. 2008.
28. Houle MS, Billman GE. Low-frequency component of the heart rate 40. OKeefe JH Jr, Abuissa H, Sastre A, Steinhaus DM, Harris WS.
variability spectrum: a poor marker of sympathetic activity. Am J Physiol Effects of omega-3 fatty acids on resting heart rate, heart rate recovery
Heart Circ Physiol 276: H215H223, 1999. after exercise, and heart rate variability in men with healed myocardial
29. Hull SS Jr, Vanoli E, Adamson PB, De Ferrari GM, Foreman RD, infarctions and depressed ejection fraction. Am J Cardiol 97: 11271130,
Schwartz PJ. Do increases in markers of vagal activity imply protection 2006.
from sudden death? The case of scopolamine. Circulation 91: 2516 2519, 41. Opthof T, Coronel R, Wilms-Schopman FJG, Plotnikov AN, Shlapa-
1995. kova IN, Danilo P Jr, Rosen MR, Janse MJ. Dispersion of repolariza-
30. Jouven X, Empana JP, Escolano S, Buyck JF, Tafflet M, Desnos M, tion in canine ventricle and electrocardiographic T wav: Tp-e interval does
Ducimetiere P. Relation of heart rate at rest and long-term (20 years) not reflect transmural dispersion. Heart Rhythm 4: 341348, 2007.
death rate in initially healthy middle-aged men. Am J Cardiol 103: 42. Parati G, di Rienzo M, Castiglioni P, Mancia G, Taylor JA, Studinger
279 283, 2009. P. Point: cardiovascular variability is/is not an index of autonomic control
31. Kang Leaf A JX. Effects of long-chain polyunsaturated fatty acids on the of circulation. J Appl Physiol 101: 676 682, 2006.
contraction of neonatal rat cardiac myocytes. Proc Natl Acad Sci USA 91: 43. Peoples GE, McLennan PL, Howe PRC, Groeller H. Fish oil reduces
9886 9890, 1994. heart rate and oxygen consumption during exercise. J Cardiovasc Phar-
32. Kottmeier CA, Gravenstein JS. The parasympathomimetic activity of macol 52: 540 547, 2008.
44. Porges SW. Respiratory sinus arrhythmia: physiological basis, quantita-
Downloaded from http://ajpheart.physiology.org/ by 10.220.33.6 on August 18, 2017
atropine and atropine methylbromide. Anesthesiology 29: 11251133,
tive methods and clinical implications. In: Cardiac, Respiratory, and
1968.
Cardiosomatic Psychophysiology. New York: Plenum, 1986, p. 101115.
33. Laustiola K, Salo MK, Mets-Ketel T. Altered physiological responses
45. Russo C, Olivieri O, Girelli D, Azzini M, Stanzial AM, Guarini P,
and decreased cyclic AMP levels in rat atria after dietary cod liver oil
Friso S, De Franceschi L, Corrocher R. Omega-3 polyunsaturated fatty
supplementation and its possible association with n3/n6 fatty acid ratio.
acid supplements and ambulatory blood pressure monitoring parameters in
Biochim Biophys Acta 889: 59 79, 1986.
patients with mild hypertension. J Hypertens 13: 18231826, 1995.
34. Mayyas F, Sakurai S, Ram R, Rennison JH, Hwang ES, Castel L, 46. Scher AM, Ohm WW, Bumgarner K, Boynton R, Young AC. Sym-
Lovano B, Brennan ML, Bibus D, Lands B, Barnard J, Chung MK, pathetic and parasympathetic control of heart rate in the dog, baboon and
Van Wagoner DR. Dietary 3 fatty acids modulate the substrate for man. Fed Proc 31: 1219 1225, 1972.
post-operative atrial fibrillation in a canine cardiac surgery model. Car- 47. Smith LL, Kukielka M, Billman GE. Heart rate recovery after exercise:
diovasc Res 89: 852861, 2011. a predictor of ventricular fibrillation susceptibility after myocardial infarc-
35. Morrison WR, Smith LM. Preparation of fatty acid methyl esters and tion. Am J Physiol Heart Circ Physiol 288: H1763H1769, 2005.
dimethylacetals from lipids with boron fluoride-methanol. J Lipid Res 5: 48. Task Force of the European Society of Cardiology, and the North
600 608, 1964. American Society of Pacing and Electrophysiology. Heart rate variabil-
36. Mozaffarian D, Prineas RJ, Stein PK, Siscovick DS. Dietary fish and ity: standards of measurement, physiological interpretation, and clinical
n-3 fatty acid intake and cardiac electrocardiographic parameters in use. Circulation 93: 10431065, 1996.
humans. J Am Coll Cardiol 48: 478 484, 2006. 49. Van de Water A, Verheyen J, Xhonnex R, Reneman RS. An improved
37. Mozaffarian D, Stein PK, Prineas RJ, Siscovick DS. Dietary fish 3 method to correct QT intrerval of the electrocardiogram from changes in
fatty acid consumption and heart rate variability in US adults. Circulation heart rate. J Pharmacol Methods 22: 207217, 1989.
117: 1130 1137, 2008. 50. Verkerk AO, den Ruijter HM, Bourier J, Boukens BJ, Brouwer IA,
38. Mozaffarian D, Geelen A, Brouwer IA, Geleijnse JM, Zock PL, Katan Wilders R, Coronel R. Dietary fish oil reduces pacemaker current and
MB. Effect of fish oil on heart rate in humans: meta-analysis of random- heart rate in rabbit. Heart Rhythm 6: 14851492, 2009.
ized controlled trials. Circulation 112: 19451952, 2005. 51. Yan GX, Antzelevitch C. Cellular basis for the normal T wave and the
39. Ninio DM, Hill AM, Howe PR, Buckley JD, Saint DA. Docosa- electrocardiographic manifestations of the long-QT syndrome. Circulation
hexaenoic acid-rich fish oil improves heart variability and heart rate 98: 1928 1936, 1998.
AJP-Heart Circ Physiol VOL 300 JUNE 2011 www.ajpheart.org
Anda mungkin juga menyukai
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- Scandinavian Med Sci Sports - 2023 - Nuzzo - Overview of Muscle Fatigue Differences Between Maximal Eccentric andDokumen15 halamanScandinavian Med Sci Sports - 2023 - Nuzzo - Overview of Muscle Fatigue Differences Between Maximal Eccentric andcsrpirataBelum ada peringkat
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (400)
- Validity of Criteria For Establishing Maximal O2 UptakeDokumen9 halamanValidity of Criteria For Establishing Maximal O2 UptakecsrpirataBelum ada peringkat
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- Cdj-200 Owners ManualDokumen92 halamanCdj-200 Owners ManualNik100% (2)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- CDJ 200 Pro cdmp3 PlayerDokumen20 halamanCDJ 200 Pro cdmp3 PlayercsrpirataBelum ada peringkat
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- LCD 4 LinuxDokumen1 halamanLCD 4 LinuxcsrpirataBelum ada peringkat
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- MB Grueezi eDokumen1 halamanMB Grueezi ecsrpirataBelum ada peringkat
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Cdj-200 Owners ManualDokumen92 halamanCdj-200 Owners ManualNik100% (2)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Validity of The Favero Assioma Duo Power PedalDokumen14 halamanValidity of The Favero Assioma Duo Power PedalcsrpirataBelum ada peringkat
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- Feedback Reporting FormDokumen1 halamanFeedback Reporting FormcsrpirataBelum ada peringkat
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (73)
- Compressors in Energy Transition: Cornerstones Filtration ComponentsDokumen60 halamanCompressors in Energy Transition: Cornerstones Filtration ComponentscsrpirataBelum ada peringkat
- 22-1K-1 Test Configuration Velometer 2021-06-07Dokumen160 halaman22-1K-1 Test Configuration Velometer 2021-06-07csrpirataBelum ada peringkat
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- Validity and Reliability of The Leomo Motion-Tracking DeviceDokumen14 halamanValidity and Reliability of The Leomo Motion-Tracking DevicecsrpirataBelum ada peringkat
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- Dynamix 2500 Data Collector: User ManualDokumen218 halamanDynamix 2500 Data Collector: User ManualcsrpirataBelum ada peringkat
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- Feedback Reporting FormDokumen1 halamanFeedback Reporting FormcsrpirataBelum ada peringkat
- Polarized Training Has Greater Impact On Key Endurance Variables Than Threshold, High Intensity, or High Volume TrainingDokumen9 halamanPolarized Training Has Greater Impact On Key Endurance Variables Than Threshold, High Intensity, or High Volume TrainingsergiBelum ada peringkat
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- RMS o Peak To Peak Acceleration Enveloping AlarmDokumen1 halamanRMS o Peak To Peak Acceleration Enveloping AlarmcsrpirataBelum ada peringkat
- Bascula Nutrition Scales PDFDokumen101 halamanBascula Nutrition Scales PDFcsrpirataBelum ada peringkat
- Gearbox Vibration Analysis - Forcing Frequencies: 16 Things Many Vibration Analysts Don't Do (But They Should)Dokumen19 halamanGearbox Vibration Analysis - Forcing Frequencies: 16 Things Many Vibration Analysts Don't Do (But They Should)Pedro RosaBelum ada peringkat
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- Exploded View and Spare Part List: 12.1 ELSI-JKD009-N11Dokumen10 halamanExploded View and Spare Part List: 12.1 ELSI-JKD009-N11csrpirataBelum ada peringkat
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- Progress Tracker Site VersionDokumen9 halamanProgress Tracker Site VersioncsrpirataBelum ada peringkat
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- How To Powercrank Firmware UpdatesDokumen1 halamanHow To Powercrank Firmware UpdatescsrpirataBelum ada peringkat
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- A Season Review VeloDokumen10 halamanA Season Review VelocsrpirataBelum ada peringkat
- Building Aerobic FitnessDokumen9 halamanBuilding Aerobic FitnesscsrpirataBelum ada peringkat
- 2015-11-18 - Suplementos para Corredores de Fondo y TriatletasDokumen4 halaman2015-11-18 - Suplementos para Corredores de Fondo y TriatletascsrpirataBelum ada peringkat
- The Effect of Bicycle Seat-Tube Angle On Muscle Activation of Lower ExtremityDokumen5 halamanThe Effect of Bicycle Seat-Tube Angle On Muscle Activation of Lower ExtremitycsrpirataBelum ada peringkat
- An Introduction To TrainingPeaks MetricsDokumen1 halamanAn Introduction To TrainingPeaks MetricscsrpirataBelum ada peringkat
- Colector Analizador de Vibraciones Falcon PDF 2 MBDokumen6 halamanColector Analizador de Vibraciones Falcon PDF 2 MBGabriel Alexis MartínezBelum ada peringkat
- Ref Antena W211Dokumen1 halamanRef Antena W211csrpirataBelum ada peringkat
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- Vehicle ListDokumen44 halamanVehicle ListcsrpirataBelum ada peringkat
- PC's & Laptop Accessories PDFDokumen4 halamanPC's & Laptop Accessories PDFsundar chapagainBelum ada peringkat
- Instruction Manual Twin Lobe CompressorDokumen10 halamanInstruction Manual Twin Lobe Compressorvsaagar100% (1)
- Planning Effective Advertising and Promotion Strategies For A Target AudienceDokumen16 halamanPlanning Effective Advertising and Promotion Strategies For A Target Audiencebakhoo12Belum ada peringkat
- Wall Panel SystemsDokumen57 halamanWall Panel SystemsChrisel DyBelum ada peringkat
- T10 - PointersDokumen3 halamanT10 - PointersGlory of Billy's Empire Jorton KnightBelum ada peringkat
- Encapsulation of Objects and Methods in C++Dokumen46 halamanEncapsulation of Objects and Methods in C++Scott StanleyBelum ada peringkat
- COMMISSIONING COUPLE Aafidavit SANKET DOCTORDokumen2 halamanCOMMISSIONING COUPLE Aafidavit SANKET DOCTORYogesh ChaudhariBelum ada peringkat
- Johari WindowDokumen7 halamanJohari WindowSarthak Priyank VermaBelum ada peringkat
- Kamapehmilya: Fitness Through Traditional DancesDokumen21 halamanKamapehmilya: Fitness Through Traditional DancesValerieBelum ada peringkat
- Lab Report 2Dokumen5 halamanLab Report 2Md jubayer SiddiqueBelum ada peringkat
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- Lyka Kendall B. Adres: Personal Na ImpormasyonDokumen2 halamanLyka Kendall B. Adres: Personal Na ImpormasyonKendall BarbietoBelum ada peringkat
- Presentation No. 3 - Songs and ChantsDokumen44 halamanPresentation No. 3 - Songs and Chantsandie hinchBelum ada peringkat
- Eureka Math Grade 2 Module 3 Parent Tip Sheet 1Dokumen2 halamanEureka Math Grade 2 Module 3 Parent Tip Sheet 1api-324573119Belum ada peringkat
- EstoqueDokumen56 halamanEstoqueGustavo OliveiraBelum ada peringkat
- Advanced Methods For Complex Network AnalysisDokumen2 halamanAdvanced Methods For Complex Network AnalysisCS & ITBelum ada peringkat
- PDF Synopsis PDFDokumen9 halamanPDF Synopsis PDFAllan D GrtBelum ada peringkat
- Chanakya: For The Indian Television Series Based On His Life, SeeDokumen11 halamanChanakya: For The Indian Television Series Based On His Life, SeeTrinadh CrazyguyBelum ada peringkat
- Acronyms and AbbreviationsDokumen875 halamanAcronyms and AbbreviationsLacky KrishnanBelum ada peringkat
- Tylenol CrisisDokumen2 halamanTylenol CrisisNida SweetBelum ada peringkat
- BDRRM Sample Draft EoDokumen5 halamanBDRRM Sample Draft EoJezreelJhizelRamosMendozaBelum ada peringkat
- Letter of Acceptfor TDokumen3 halamanLetter of Acceptfor TCCSBelum ada peringkat
- Space Saving, Tight AccessibilityDokumen4 halamanSpace Saving, Tight AccessibilityTran HuyBelum ada peringkat
- Ultrasonic Based Distance Measurement SystemDokumen18 halamanUltrasonic Based Distance Measurement SystemAman100% (2)
- API IND DS2 en Excel v2 10081834Dokumen462 halamanAPI IND DS2 en Excel v2 10081834Suvam PatelBelum ada peringkat
- Gothic ArchitectureDokumen6 halamanGothic ArchitectureleeBelum ada peringkat
- Resolution: Owner/Operator, DocketedDokumen4 halamanResolution: Owner/Operator, DocketedDonna Grace Guyo100% (1)
- Data Structures and Algorithms SyllabusDokumen9 halamanData Structures and Algorithms SyllabusBongbong GalloBelum ada peringkat
- Book Review Fiction New HereDokumen7 halamanBook Review Fiction New HereFILZAH SYAUQINA BINTI SUBLY Pelajar KPTM IpohBelum ada peringkat
- Starbucks Progressive Web App: Case StudyDokumen2 halamanStarbucks Progressive Web App: Case StudyYesid SuárezBelum ada peringkat
- Sinamics g120 BrochureDokumen16 halamanSinamics g120 BrochuremihacraciunBelum ada peringkat
- Chair Yoga: Sit, Stretch, and Strengthen Your Way to a Happier, Healthier YouDari EverandChair Yoga: Sit, Stretch, and Strengthen Your Way to a Happier, Healthier YouPenilaian: 3.5 dari 5 bintang3.5/5 (5)
- Boundless: Upgrade Your Brain, Optimize Your Body & Defy AgingDari EverandBoundless: Upgrade Your Brain, Optimize Your Body & Defy AgingPenilaian: 4.5 dari 5 bintang4.5/5 (66)
- Aging Backwards: Reverse the Aging Process and Look 10 Years Younger in 30 Minutes a DayDari EverandAging Backwards: Reverse the Aging Process and Look 10 Years Younger in 30 Minutes a DayBelum ada peringkat
- Peak: The New Science of Athletic Performance That is Revolutionizing SportsDari EverandPeak: The New Science of Athletic Performance That is Revolutionizing SportsPenilaian: 5 dari 5 bintang5/5 (96)
- Relentless: From Good to Great to UnstoppableDari EverandRelentless: From Good to Great to UnstoppablePenilaian: 5 dari 5 bintang5/5 (785)
- The Yogi Code: Seven Universal Laws of Infinite SuccessDari EverandThe Yogi Code: Seven Universal Laws of Infinite SuccessPenilaian: 4.5 dari 5 bintang4.5/5 (104)
- Power of 10: The Once-A-Week Slow Motion Fitness RevolutionDari EverandPower of 10: The Once-A-Week Slow Motion Fitness RevolutionPenilaian: 3.5 dari 5 bintang3.5/5 (11)
- Not a Diet Book: Take Control. Gain Confidence. Change Your Life.Dari EverandNot a Diet Book: Take Control. Gain Confidence. Change Your Life.Penilaian: 4.5 dari 5 bintang4.5/5 (124)