Anda mungkin juga menyukai
- 110 211 1 SM PDFDokumen2 halaman110 211 1 SM PDFjohannaBelum ada peringkat
- Acute Coronary Syndrome Sindroma Koroner AkutDokumen50 halamanAcute Coronary Syndrome Sindroma Koroner AkutWinda Ayu PurnamasariBelum ada peringkat
- 2014 NSTE ACS Slide SetDokumen109 halaman2014 NSTE ACS Slide SetmikaBelum ada peringkat
- Weekly Ortophedi FiiiiiixDokumen51 halamanWeekly Ortophedi FiiiiiixWinda Ayu PurnamasariBelum ada peringkat
- PHC Community DiagnosisDokumen27 halamanPHC Community DiagnosisCassandra_Maca_6324Belum ada peringkat
- Weekly Ortophedi FiiiiiixDokumen51 halamanWeekly Ortophedi FiiiiiixWinda Ayu PurnamasariBelum ada peringkat
- EpidemiologyDokumen1 halamanEpidemiologyWinda Ayu PurnamasariBelum ada peringkat
- Undescended Testis - Current Trends and Guidelines: A Review of The LiteratureDokumen19 halamanUndescended Testis - Current Trends and Guidelines: A Review of The LiteratureWinda Ayu PurnamasariBelum ada peringkat
- 1446 7608 3 PBDokumen4 halaman1446 7608 3 PBWinda Ayu PurnamasariBelum ada peringkat
- Clinical & Experimental Dermatology Research: Pruritus of Healing Wounds: Why "Scabs" ItchDokumen5 halamanClinical & Experimental Dermatology Research: Pruritus of Healing Wounds: Why "Scabs" ItchWinda Ayu PurnamasariBelum ada peringkat
- Weekly OrthopedicDokumen28 halamanWeekly OrthopedicWinda Ayu PurnamasariBelum ada peringkat
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (74)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- Methadone - DrugBankDokumen13 halamanMethadone - DrugBankravaBelum ada peringkat
- Cdi MockboardDokumen61 halamanCdi MockboardButch Kyle GalvezBelum ada peringkat
- Analgesics Word DocumentDokumen18 halamanAnalgesics Word DocumentvisweswarkcBelum ada peringkat
- Dark Classics in Chemical Neuroscience Opium A Friend or FoeDokumen9 halamanDark Classics in Chemical Neuroscience Opium A Friend or FoeChristopher CookBelum ada peringkat
- Factors Affecting Drug ActionDokumen3 halamanFactors Affecting Drug ActionHempriya Tomar0% (1)
- 8 - Toxicants That Cause Central Nervous System DepressionDokumen22 halaman8 - Toxicants That Cause Central Nervous System DepressionCabinet VeterinarBelum ada peringkat
- Transdermal Analgesic Patch GuideDokumen3 halamanTransdermal Analgesic Patch GuideSeanBelum ada peringkat
- Psychotropic Drugs ReviewDokumen16 halamanPsychotropic Drugs ReviewVîñàý PãtêlBelum ada peringkat
- Desomorphine KrokodilDokumen20 halamanDesomorphine Krokodilapi-252934043Belum ada peringkat
- Health Psychology 8Th Edition Taylor Test Bank Full Chapter PDFDokumen47 halamanHealth Psychology 8Th Edition Taylor Test Bank Full Chapter PDFDeborahAndersonmkpy100% (12)
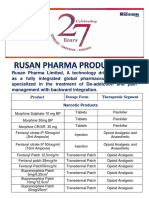
- Rusan Pharma Product ListDokumen4 halamanRusan Pharma Product ListSanjay SharmaBelum ada peringkat
- Opioid AnalgesicsDokumen41 halamanOpioid AnalgesicsSayan NagBelum ada peringkat
- Forensic Toxicology HDokumen18 halamanForensic Toxicology Hq_onda_fhonixBelum ada peringkat
- Preanesthetic Medication JasminaDokumen44 halamanPreanesthetic Medication Jasminaanjali s100% (1)
- OpiateConversionDoses (Final) Nov2010Dokumen1 halamanOpiateConversionDoses (Final) Nov2010NajihBelum ada peringkat
- Fundamentals of Pharmacology 8th Edition Bullock Test BankDokumen9 halamanFundamentals of Pharmacology 8th Edition Bullock Test Bankdorissamuelqpnrrz100% (27)
- Pharmacology 1 - Case Study 1Dokumen2 halamanPharmacology 1 - Case Study 1BaldogBelum ada peringkat
- Drug Study of OpioidDokumen3 halamanDrug Study of OpioidGerrahBelum ada peringkat
- Isoquinoline AlkaloidsDokumen83 halamanIsoquinoline AlkaloidsAlan K MhamadBelum ada peringkat
- Recall QuestionsDokumen2 halamanRecall QuestionsAymen BekirBelum ada peringkat
- NDPS Act 1985Dokumen27 halamanNDPS Act 1985Ashish DavessarBelum ada peringkat
- ASSIST-Y 10-14yo DRAFT Questionnaire 24Oct2011-DASSA-June2013Dokumen4 halamanASSIST-Y 10-14yo DRAFT Questionnaire 24Oct2011-DASSA-June2013Denina DeninaBelum ada peringkat
- NSTP 1 CWTS 1 Module For Health Care and Drug Education First Semester AY 2021-2022Dokumen40 halamanNSTP 1 CWTS 1 Module For Health Care and Drug Education First Semester AY 2021-2022Marialyn AnonuevoBelum ada peringkat
- Patient Controlled AnalgesiaDokumen5 halamanPatient Controlled AnalgesianxBelum ada peringkat
- Pain Management in Infants, Children, Adolescents, and Individuals With Special Health Care NeedsDokumen9 halamanPain Management in Infants, Children, Adolescents, and Individuals With Special Health Care Needsnona aryanBelum ada peringkat
- Opioid AnalgesicsDokumen29 halamanOpioid AnalgesicsamonlisaBelum ada peringkat
- Alkaloids 1 1Dokumen276 halamanAlkaloids 1 1عبدو عبدوBelum ada peringkat
- Chapter 5 Forensic ScienceDokumen52 halamanChapter 5 Forensic ScienceGABRIEL DIASBelum ada peringkat
- Kimia AnalisisDokumen75 halamanKimia AnalisisQonita NitaBelum ada peringkat
- Review of Organic Chemistry Functional Group Solutions ManualDokumen252 halamanReview of Organic Chemistry Functional Group Solutions ManualRaul Marquez0% (1)