Anda mungkin juga menyukai
- Learjet 45 Pilot Traning Manual Volumen 2Dokumen539 halamanLearjet 45 Pilot Traning Manual Volumen 2Agustin Bernales88% (8)
- PLAXIS Tutorial ManualDokumen124 halamanPLAXIS Tutorial ManualPeteris Skels100% (2)
- MDN 1508DSDokumen108 halamanMDN 1508DSdocazanBelum ada peringkat
- Feature Setup Description: Software Basic Data Mcs - TCBCDokumen77 halamanFeature Setup Description: Software Basic Data Mcs - TCBCAlexis MauricioBelum ada peringkat
- Din en 1561 - en - 1997-08Dokumen21 halamanDin en 1561 - en - 1997-08AlissonFernandes17Belum ada peringkat
- Gold Series Dust Collector: Installation, Operation and MaintenanceDokumen85 halamanGold Series Dust Collector: Installation, Operation and MaintenanceDAVID ALFONSO CARABALLO PATIÑOBelum ada peringkat
- Grade 9 ICT Network Configuration GuideDokumen15 halamanGrade 9 ICT Network Configuration GuideMark Anthony Nieva RafalloBelum ada peringkat
- Distinguishing MR ImagingDokumen6 halamanDistinguishing MR ImagingWinda HaeriyokoBelum ada peringkat
- Nasopharyngeal Carcinoma: Imaging Features of Unusual Cancer in ChildrenDokumen5 halamanNasopharyngeal Carcinoma: Imaging Features of Unusual Cancer in ChildrenDevanti EkaBelum ada peringkat
- Differentiating Pediatric Brain Tumor Grade Using Apparent Diffusion CoefficientsDokumen6 halamanDifferentiating Pediatric Brain Tumor Grade Using Apparent Diffusion CoefficientsadfirdaBelum ada peringkat
- ADC in MRI Determines Paediatric Brain Tumour GradesDokumen7 halamanADC in MRI Determines Paediatric Brain Tumour GradesKathia AguilarBelum ada peringkat
- Shi 2017Dokumen8 halamanShi 2017Claudia Ivette Villarreal OvalleBelum ada peringkat
- Accuracy of Computerised Tomography in Diagnosis of Brain Tumours in ChildrenDokumen3 halamanAccuracy of Computerised Tomography in Diagnosis of Brain Tumours in ChildrenVidinikusumaBelum ada peringkat
- Aziz Khan 1985Dokumen7 halamanAziz Khan 1985Eric MunBelum ada peringkat
- Mri Evaluation of Medulloblastoma With Histopahtological CorrelationDokumen5 halamanMri Evaluation of Medulloblastoma With Histopahtological CorrelationVidinikusumaBelum ada peringkat
- Hiperplasia Condilar3Dokumen5 halamanHiperplasia Condilar3Alejandra Oliveros VargasBelum ada peringkat
- Atypical Pituitary Adenoma: A Case ReportDokumen3 halamanAtypical Pituitary Adenoma: A Case ReportMuhammad Hafizh Islam SadidaBelum ada peringkat
- 1.masas en CuelloDokumen3 halaman1.masas en CuelloIsaac TellezBelum ada peringkat
- Acute Brain MRI Findings in Malawian Children with Cerebral MalariaDokumen7 halamanAcute Brain MRI Findings in Malawian Children with Cerebral MalariaRobin SianiparBelum ada peringkat
- Low and High Grade Gliom in MRSDokumen8 halamanLow and High Grade Gliom in MRSHuyen NguyenBelum ada peringkat
- Atypical Teratoid:Rhabdoid Tumors in Adult Patients: CT and MR Imaging FeaturesDokumen7 halamanAtypical Teratoid:Rhabdoid Tumors in Adult Patients: CT and MR Imaging FeaturesMauro CampelloBelum ada peringkat
- 2014-Metrics and Textural Features of MRI Diffusion To Improve Classification of Pediatric Posterior Fossa TumorsDokumen7 halaman2014-Metrics and Textural Features of MRI Diffusion To Improve Classification of Pediatric Posterior Fossa TumorsAhmet KaragozBelum ada peringkat
- 1 s2.0 S1083318820303703Dokumen6 halaman1 s2.0 S1083318820303703ashwiniBelum ada peringkat
- Koch 2009Dokumen9 halamanKoch 2009Intan Kartika NursyahbaniBelum ada peringkat
- Achondroplasia Natural History Study (CLARITY)Dokumen7 halamanAchondroplasia Natural History Study (CLARITY)jakelinelagoadvBelum ada peringkat
- Space Occupying Lesions of Central Nervous System: A Radiological and Histopathological CorrelationDokumen6 halamanSpace Occupying Lesions of Central Nervous System: A Radiological and Histopathological CorrelationRaja WartegBelum ada peringkat
- Angiosarcoma of The Spleen: Imaging Characteristics in 12 PatientsDokumen10 halamanAngiosarcoma of The Spleen: Imaging Characteristics in 12 PatientsHuyen NguyenBelum ada peringkat
- Maris 2007Dokumen15 halamanMaris 2007asialoren74Belum ada peringkat
- Endovaginal Ultrasound and Doppler Findings After First-Trimester Abortion (Journal of Diagnostic Medical Sonography, Vol. 9, Issue 2) (1993)Dokumen1 halamanEndovaginal Ultrasound and Doppler Findings After First-Trimester Abortion (Journal of Diagnostic Medical Sonography, Vol. 9, Issue 2) (1993)Orchid LandBelum ada peringkat
- Ijss Nov Oa28Dokumen5 halamanIjss Nov Oa28Irsanti sasmitaBelum ada peringkat
- Updatesinpediatric Cholesteatoma: Minimizing Intervention While Maximizing OutcomesDokumen11 halamanUpdatesinpediatric Cholesteatoma: Minimizing Intervention While Maximizing OutcomesenviBelum ada peringkat
- Brain Diffusion Tensor Imaging in Children With Tuberous SclerosisDokumen6 halamanBrain Diffusion Tensor Imaging in Children With Tuberous SclerosisNurul Huda KowitaBelum ada peringkat
- Radiographic Imaging of Mastoid in Chronic OtitisDokumen5 halamanRadiographic Imaging of Mastoid in Chronic OtitisEMIRZA NUR WICAKSONOBelum ada peringkat
- HydrocephalusDokumen8 halamanHydrocephaluscaliptra36Belum ada peringkat
- 10 1002@pbc 27697Dokumen8 halaman10 1002@pbc 27697Ravi JhaBelum ada peringkat
- Dysembryoplastic Neuroepithelial Tumors in Childhood: Long-Term Outcome and Prognostic FeaturesDokumen7 halamanDysembryoplastic Neuroepithelial Tumors in Childhood: Long-Term Outcome and Prognostic Featureslucasher35Belum ada peringkat
- Review Article: Recent Advances in Childhood Brain TumoursDokumen10 halamanReview Article: Recent Advances in Childhood Brain Tumoursjosue_wigBelum ada peringkat
- Abnormalities in RibsDokumen17 halamanAbnormalities in RibsMARIA ISABELA URREA CARDONABelum ada peringkat
- Rycan 2021210036Dokumen7 halamanRycan 2021210036Imagenologia Hospital de ClinicasBelum ada peringkat
- Non Small-Cell Lung Cancer in A 15-Year-Old NonsmokerDokumen2 halamanNon Small-Cell Lung Cancer in A 15-Year-Old Nonsmokertonirian99Belum ada peringkat
- Application of Cortical Bone Trajectory Instrumentation For Juvenile and Adolescent Idiopathic Scoliosis PDFDokumen2 halamanApplication of Cortical Bone Trajectory Instrumentation For Juvenile and Adolescent Idiopathic Scoliosis PDFJasonBelum ada peringkat
- 0959 80492995521 7Dokumen1 halaman0959 80492995521 7Sayda DhaouadiBelum ada peringkat
- Meta-Análise 2021 - ItáliaDokumen9 halamanMeta-Análise 2021 - ItáliaLeonardo Müller RodriguesBelum ada peringkat
- Wu Et Al 2020 Descending Necrotizing Mediastinitis Analysis of 9 Cases in Our HospitalDokumen4 halamanWu Et Al 2020 Descending Necrotizing Mediastinitis Analysis of 9 Cases in Our HospitalcharlaayasyafefiBelum ada peringkat
- SWAIMANDokumen18 halamanSWAIMANVan John MagallanesBelum ada peringkat
- Amiel Tison2012Dokumen7 halamanAmiel Tison2012Anonymous Xmb6QQvRBelum ada peringkat
- Mass-Like Extramedullary Hematopoiesis: Imaging Features: Scientific ArticleDokumen6 halamanMass-Like Extramedullary Hematopoiesis: Imaging Features: Scientific ArticleVo VũBelum ada peringkat
- Pathologic Quiz Case: Ovarian Mass in A 2-Year-Old Girl Presenting With Pleural EffusionsDokumen4 halamanPathologic Quiz Case: Ovarian Mass in A 2-Year-Old Girl Presenting With Pleural EffusionsMateen ShukriBelum ada peringkat
- Blunt Abdiminal TraumaDokumen6 halamanBlunt Abdiminal TraumaErdyBelum ada peringkat
- Supraclavicular Lymph NodeDokumen14 halamanSupraclavicular Lymph NodeNeva PadillaBelum ada peringkat
- 1 s2.0 S0378603X13001253 MainDokumen8 halaman1 s2.0 S0378603X13001253 MainMoh Hidayat ThahaBelum ada peringkat
- Research Article: ISSN: 2319-6505 ISSN: 2319 - 6475Dokumen6 halamanResearch Article: ISSN: 2319-6505 ISSN: 2319 - 6475Leonor TorresBelum ada peringkat
- Andreasen 2015Dokumen6 halamanAndreasen 2015stoia_sebiBelum ada peringkat
- ShearWave Elastography Thyroid NodulesDokumen8 halamanShearWave Elastography Thyroid Nodulesinfo8089Belum ada peringkat
- Brain Abscess in Uncorrected Tetralogy of Fallot Diagnosed During Preparationfor Computed Cardiac Angiotomography 2329 9517 1000193Dokumen2 halamanBrain Abscess in Uncorrected Tetralogy of Fallot Diagnosed During Preparationfor Computed Cardiac Angiotomography 2329 9517 1000193nisaBelum ada peringkat
- 1369 Full PDFDokumen9 halaman1369 Full PDFIqbal AbdillahBelum ada peringkat
- Perilongo 1997Dokumen7 halamanPerilongo 1997Gustav RSRBelum ada peringkat
- Ultrasonography Detects Large Mixed-Echo Masses in Immature Ovarian TeratomasDokumen8 halamanUltrasonography Detects Large Mixed-Echo Masses in Immature Ovarian TeratomasIlincaBelum ada peringkat
- Characteristics and Outcome of Patients With Ganglioneuroblastoma, Nodular Subtype: A Report From The INRG ProjectDokumen7 halamanCharacteristics and Outcome of Patients With Ganglioneuroblastoma, Nodular Subtype: A Report From The INRG ProjectWahyudhy SajaBelum ada peringkat
- Askin's TumorDokumen5 halamanAskin's Tumoranon_828221297Belum ada peringkat
- Pediatri RabdomyosarkomDokumen7 halamanPediatri RabdomyosarkomDogukan DemirBelum ada peringkat
- 2017 Article 141 Part9Dokumen5 halaman2017 Article 141 Part9Karina MonasaBelum ada peringkat
- Brain Abnormalities On MR Imaging in Patients With RetinoblastomaDokumen5 halamanBrain Abnormalities On MR Imaging in Patients With RetinoblastomaSabrina SanchezBelum ada peringkat
- LancetradiacionDokumen7 halamanLancetradiacionIbai ArregiBelum ada peringkat
- Down Leukemia JAMA 2023Dokumen8 halamanDown Leukemia JAMA 2023pedsoncoaiimsBelum ada peringkat
- Me Hanna 2016Dokumen11 halamanMe Hanna 2016eswarBelum ada peringkat
- Imaging in Pediatric OncologyDari EverandImaging in Pediatric OncologyStephan D. VossBelum ada peringkat
- Specificity and SensitivityDokumen18 halamanSpecificity and SensitivityKaran SharmaBelum ada peringkat
- Ajr 181 6 1811695Dokumen10 halamanAjr 181 6 1811695Danu BagoesBelum ada peringkat
- 12 GP Ruptured Corpus LuteumDokumen3 halaman12 GP Ruptured Corpus LuteumDanu BagoesBelum ada peringkat
- 574 FTPDokumen10 halaman574 FTPDanu BagoesBelum ada peringkat
- 2010 06 Articles AR - 06 10 - Gill AR - 06 10 - GillDokumen11 halaman2010 06 Articles AR - 06 10 - Gill AR - 06 10 - GillDanu BagoesBelum ada peringkat
- Pediatric TumorsDokumen25 halamanPediatric Tumorswiwit adeBelum ada peringkat
- Management of Nodal Recurrent of Endometrial Cancer With IMRTDokumen17 halamanManagement of Nodal Recurrent of Endometrial Cancer With IMRTDanu BagoesBelum ada peringkat
- Uk EpendymomaDokumen7 halamanUk EpendymomaDanu BagoesBelum ada peringkat
- 31 TerdimanDokumen24 halaman31 TerdimanDanu BagoesBelum ada peringkat
- 10.1177 2047981613515211Dokumen4 halaman10.1177 2047981613515211DianAndikaBelum ada peringkat
- 0218492311419164Dokumen9 halaman0218492311419164Danu BagoesBelum ada peringkat
- Assessment of Self Taken Swab Versus Clinican Taken Swab Culture For Diagnosing Gonorrhoea in WomenDokumen8 halamanAssessment of Self Taken Swab Versus Clinican Taken Swab Culture For Diagnosing Gonorrhoea in WomenDanu BagoesBelum ada peringkat
- Evaluacion Conducto Nasolagrimal 1000Dokumen4 halamanEvaluacion Conducto Nasolagrimal 1000Leonardo J. BarriaBelum ada peringkat
- Ecr2010 C-0850Dokumen28 halamanEcr2010 C-0850Danu BagoesBelum ada peringkat
- Case DKJ 18 December 2014Dokumen29 halamanCase DKJ 18 December 2014Danu BagoesBelum ada peringkat
- Breast Cancer Staging PDFDokumen12 halamanBreast Cancer Staging PDFDanu BagoesBelum ada peringkat
- Assessment of Self Taken Swab Versus Clinican Taken Swab Culture For Diagnosing Gonorrhoea in WomenDokumen8 halamanAssessment of Self Taken Swab Versus Clinican Taken Swab Culture For Diagnosing Gonorrhoea in WomenDanu BagoesBelum ada peringkat
- Anders K, 2012 PDFDokumen6 halamanAnders K, 2012 PDFmangiemrBelum ada peringkat
- Assessment of Self Taken Swab Versus Clinican Taken Swab Culture For Diagnosing Gonorrhoea in WomenDokumen8 halamanAssessment of Self Taken Swab Versus Clinican Taken Swab Culture For Diagnosing Gonorrhoea in WomenDanu BagoesBelum ada peringkat
- 8 Bit Invaders RulesDokumen4 halaman8 Bit Invaders RulesRollo MirfinoBelum ada peringkat
- VF1 Technicalspecifications 031997 EN PDFDokumen43 halamanVF1 Technicalspecifications 031997 EN PDFelectricistBelum ada peringkat
- Design of Miniature Maglev Using Hybrid MagnetsDokumen4 halamanDesign of Miniature Maglev Using Hybrid MagnetsErmin FazlicBelum ada peringkat
- Citrix Xen Desktop Interview Questions and Answers - Citrix Xen Desktop FAQsDokumen3 halamanCitrix Xen Desktop Interview Questions and Answers - Citrix Xen Desktop FAQsAnonymous rNmxZViYaBelum ada peringkat
- Djdusty VideolistDokumen302 halamanDjdusty VideolistgonduBelum ada peringkat
- Strategic Human Resource Management and The HR ScorecardDokumen20 halamanStrategic Human Resource Management and The HR ScorecardRajat JainBelum ada peringkat
- Bringing Industrial Automation Environment Into Classroom: A Didactic Three-Tank and Heat Exchanger ModuleDokumen5 halamanBringing Industrial Automation Environment Into Classroom: A Didactic Three-Tank and Heat Exchanger Modulenicacio_89507470Belum ada peringkat
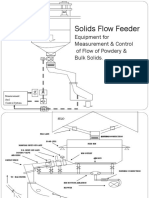
- Solids Flow Feeder Equipment for Precise Measurement & ControlDokumen7 halamanSolids Flow Feeder Equipment for Precise Measurement & ControlAbhishek DuttaBelum ada peringkat
- Ordinary Portland Cement, 33 Grade - Specification: Indian StandardDokumen12 halamanOrdinary Portland Cement, 33 Grade - Specification: Indian StandardAmbrishBelum ada peringkat
- Look at The Picture Carefully. Rearrange The Words To Form Correct SentencesDokumen6 halamanLook at The Picture Carefully. Rearrange The Words To Form Correct SentencesAdy PutraBelum ada peringkat
- Secure Email Transaction SystemDokumen32 halamanSecure Email Transaction SystemGautam Sharma100% (1)
- Assignment OracleDokumen4 halamanAssignment OracleKyle Austin PabustanBelum ada peringkat
- Net HSMDokumen4 halamanNet HSMJosé Tudela de la RosaBelum ada peringkat
- Instruction and Maintenance Manual: Silenced Screw Rotary Compressor UnitsDokumen34 halamanInstruction and Maintenance Manual: Silenced Screw Rotary Compressor UnitsJohnny Diaz VargasBelum ada peringkat
- Tapered Roller Bearings, RBC Tapered Thrust Bearings: Producing High-Quality Products Since 1929Dokumen16 halamanTapered Roller Bearings, RBC Tapered Thrust Bearings: Producing High-Quality Products Since 1929eblees100Belum ada peringkat
- How To Setup CM Notify SyncDokumen2 halamanHow To Setup CM Notify SyncascfsfBelum ada peringkat
- United States Patent (19) : HoferDokumen7 halamanUnited States Patent (19) : Hoferjoel marshallBelum ada peringkat
- B2B ApiDokumen350 halamanB2B ApiratnavelpBelum ada peringkat
- Process Management: Operating SystemsDokumen48 halamanProcess Management: Operating SystemsvidishsaBelum ada peringkat
- Project: Water Supply Layout Finals Drawn By: 20141142805 Date: 10/11/2018 Sheet No. 1 of 2Dokumen1 halamanProject: Water Supply Layout Finals Drawn By: 20141142805 Date: 10/11/2018 Sheet No. 1 of 2Jabber Reyes AmborBelum ada peringkat
- LCD panel and module replacement parts for saleDokumen1 halamanLCD panel and module replacement parts for saleValeria bolañosBelum ada peringkat
- Nokia 7368 ISAM ONT G-010G-A For Optical LAN Data Sheet enDokumen3 halamanNokia 7368 ISAM ONT G-010G-A For Optical LAN Data Sheet enMirado AndriamihasinoroBelum ada peringkat
- Block Out TimeDokumen3 halamanBlock Out TimeschumangelBelum ada peringkat