Anda mungkin juga menyukai
- Models For DC MotorsDokumen8 halamanModels For DC MotorsebrahimpanBelum ada peringkat
- Sensors: Adaptive PIF Control For Permanent Magnet Synchronous Motors Based On GPCDokumen18 halamanSensors: Adaptive PIF Control For Permanent Magnet Synchronous Motors Based On GPCebrahimpanBelum ada peringkat
- Solution 2Dokumen5 halamanSolution 2Paulina MarquezBelum ada peringkat
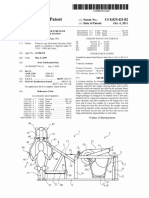
- United States Patent (10) Patent N6 US 8,029,424 B2: Thulin 45 Date of Patent: Oct. 4 2011Dokumen15 halamanUnited States Patent (10) Patent N6 US 8,029,424 B2: Thulin 45 Date of Patent: Oct. 4 2011ebrahimpanBelum ada peringkat
- Adaptation of Multijoint Coordination During Standing Balance in Healthy Young and Healthy Old IndividualsDokumen14 halamanAdaptation of Multijoint Coordination During Standing Balance in Healthy Young and Healthy Old IndividualsebrahimpanBelum ada peringkat
- DC motor dynamic modeling and control techniquesDokumen23 halamanDC motor dynamic modeling and control techniquesKaderBelum ada peringkat
- Open Sim Tutorial 1Dokumen10 halamanOpen Sim Tutorial 1Rayanne FlorianoBelum ada peringkat
- Mechatronics: Haoyong Yu, Sunan Huang, Gong Chen, Nitish ThakorDokumen12 halamanMechatronics: Haoyong Yu, Sunan Huang, Gong Chen, Nitish ThakorebrahimpanBelum ada peringkat
- Open Sim Tutorial 1Dokumen10 halamanOpen Sim Tutorial 1Rayanne FlorianoBelum ada peringkat
- c3d2OpenSim TutorialDokumen8 halamanc3d2OpenSim Tutorialebrahimpan100% (1)
- Yjmt 23 188Dokumen9 halamanYjmt 23 188ebrahimpanBelum ada peringkat
- Design and Implementation of A Distributed Variable Impedance Actuator Using Parallel Linear SpringsDokumen12 halamanDesign and Implementation of A Distributed Variable Impedance Actuator Using Parallel Linear SpringsebrahimpanBelum ada peringkat
- An Assisted Waist Supporter For Vertebral RehabilitationDokumen2 halamanAn Assisted Waist Supporter For Vertebral RehabilitationebrahimpanBelum ada peringkat
- Spring Over Muscle (SOM) Actuator For Rehabilitation DevicesDokumen4 halamanSpring Over Muscle (SOM) Actuator For Rehabilitation DevicesebrahimpanBelum ada peringkat
- I6 BrochureDokumen2 halamanI6 BrochureebrahimpanBelum ada peringkat
- Viscoelasticity - RheologicalDokumen10 halamanViscoelasticity - RheologicalsaltyBelum ada peringkat
- Adaptation of Multijoint Coordination During Standing Balance in Healthy Young and Healthy Old IndividualsDokumen14 halamanAdaptation of Multijoint Coordination During Standing Balance in Healthy Young and Healthy Old IndividualsebrahimpanBelum ada peringkat
- A Review of The Use of Electro-Motor Stimulation in Human MusclesDokumen13 halamanA Review of The Use of Electro-Motor Stimulation in Human MusclesebrahimpanBelum ada peringkat
- Hasegawa 1985Dokumen6 halamanHasegawa 1985ebrahimpanBelum ada peringkat
- Three-Dimensional Joint Reaction Forces and Moments at The Low Ba PDFDokumen9 halamanThree-Dimensional Joint Reaction Forces and Moments at The Low Ba PDFebrahimpanBelum ada peringkat
- 100720141556121410000Dokumen6 halaman100720141556121410000ebrahimpanBelum ada peringkat
- A Review of The Clinical Value of Isolated Lumbar Extension Resistance Training For Chronic Low Back PainDokumen19 halamanA Review of The Clinical Value of Isolated Lumbar Extension Resistance Training For Chronic Low Back PainebrahimpanBelum ada peringkat
- 100720141556121410000Dokumen6 halaman100720141556121410000ebrahimpanBelum ada peringkat
- Mca 21 00016 v2 PDFDokumen15 halamanMca 21 00016 v2 PDFebrahimpanBelum ada peringkat
- Watanabe 2010Dokumen4 halamanWatanabe 2010ebrahimpanBelum ada peringkat
- Elastic Constitutive EquationsDokumen46 halamanElastic Constitutive EquationsAmithkumar R AchariBelum ada peringkat
- Supported Contact Mechanics ModelsDokumen8 halamanSupported Contact Mechanics ModelsebrahimpanBelum ada peringkat
- Hasegawa 1985Dokumen6 halamanHasegawa 1985ebrahimpanBelum ada peringkat
- Strain CylindricalDokumen4 halamanStrain CylindricalebrahimpanBelum ada peringkat
- Plane Strain Problems of Transversely Isotropic Thermoelastic MediaDokumen15 halamanPlane Strain Problems of Transversely Isotropic Thermoelastic MediaebrahimpanBelum ada peringkat
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5784)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (72)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (119)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- Medical ReceptionistDokumen4 halamanMedical ReceptionistM LubisBelum ada peringkat
- Nurdiana. R PD-B/ 0810713031: Module TaskDokumen10 halamanNurdiana. R PD-B/ 0810713031: Module TaskNurdiana RahmadaniBelum ada peringkat
- Cirugia BariatricaDokumen9 halamanCirugia BariatricaedwardmenesesBelum ada peringkat
- ACCIDENT REPORTING AND INVESTIGATION PROCEDUREDokumen23 halamanACCIDENT REPORTING AND INVESTIGATION PROCEDUREkirandevi1981Belum ada peringkat
- WeeFIM Score Sheet (MS Word)Dokumen4 halamanWeeFIM Score Sheet (MS Word)Siti Maryam Rosyidah0% (2)
- UrinalysisDokumen16 halamanUrinalysisJestha Parayno De Vera100% (6)
- Shatavari (Asparagus Racemosus), Jivanti (Leptadenia Reticulata) and Methi (Trigonella Foenum-Graecum) : The Herbal Galactogogues For RuminantsDokumen7 halamanShatavari (Asparagus Racemosus), Jivanti (Leptadenia Reticulata) and Methi (Trigonella Foenum-Graecum) : The Herbal Galactogogues For RuminantsSanjay C. ParmarBelum ada peringkat
- Erasme Igitabo Cy' Imiti Ivura Abantu Yo Mu Ibyaremwe 2Dokumen105 halamanErasme Igitabo Cy' Imiti Ivura Abantu Yo Mu Ibyaremwe 2gashesabiBelum ada peringkat
- Spectrophotometric determination of total phenolic content in Gul-e-ZoofaDokumen4 halamanSpectrophotometric determination of total phenolic content in Gul-e-Zoofayulyansyah susantoBelum ada peringkat
- Ewert WCNDT Standards 2012 04 PDFDokumen38 halamanEwert WCNDT Standards 2012 04 PDFJorge Manuel GuillermoBelum ada peringkat
- Afifah FixedDokumen25 halamanAfifah FixedAfifah Nur KartikasariBelum ada peringkat
- MOU Between LA Net and CLINICDokumen3 halamanMOU Between LA Net and CLINICMaja AtanasovaBelum ada peringkat
- Hospital ICU Organization and TypesDokumen82 halamanHospital ICU Organization and TypesPaul Shan GoBelum ada peringkat
- Refacere Dinti Frontali Cu Cape de CeluloidDokumen5 halamanRefacere Dinti Frontali Cu Cape de CeluloidSorina NeamțuBelum ada peringkat
- 2021-2022 Sem 2 Lecture 2 Basic Tests in Vision Screenings - Student VersionDokumen123 halaman2021-2022 Sem 2 Lecture 2 Basic Tests in Vision Screenings - Student Versionpi55aBelum ada peringkat
- Correlation of Sound and Colour - Paul Foster CaseDokumen30 halamanCorrelation of Sound and Colour - Paul Foster Casesrk777100% (7)
- Tfios Mediastudyguide v4Dokumen7 halamanTfios Mediastudyguide v4api-308995770Belum ada peringkat
- Bioactive Compounds in Phytomedicine BookDokumen228 halamanBioactive Compounds in Phytomedicine BookAnil KumarBelum ada peringkat
- CIPHIDokumen256 halamanCIPHIसदानंद देशपांडेBelum ada peringkat
- Research Background: (Budget 2016: Chapter 5 - An Inclusive and Fair Canada, 2021)Dokumen4 halamanResearch Background: (Budget 2016: Chapter 5 - An Inclusive and Fair Canada, 2021)Talha NaseemBelum ada peringkat
- Ban Biblio NumberedDokumen23 halamanBan Biblio NumberedYayangAsanggaBelum ada peringkat
- 2 Months To LiveDokumen26 halaman2 Months To LivedtsimonaBelum ada peringkat
- Pharmacy Math CalculationsDokumen8 halamanPharmacy Math CalculationsRahmawati KuswandiBelum ada peringkat
- A Comparison of Muscle Strength and Flexibility Between The Preferred and Non Preferred Leg in English Soccer PlayersDokumen10 halamanA Comparison of Muscle Strength and Flexibility Between The Preferred and Non Preferred Leg in English Soccer PlayersMalikiBelum ada peringkat
- Case Study: Exercise 2: Triage 1Dokumen26 halamanCase Study: Exercise 2: Triage 1Chandra DewiBelum ada peringkat
- NTR OductionDokumen83 halamanNTR OductionmalathiBelum ada peringkat
- Maharashtra Government PGM Admissions 2015-2016 Round 2 Selection ListDokumen30 halamanMaharashtra Government PGM Admissions 2015-2016 Round 2 Selection ListAbhinav BhardwajBelum ada peringkat
- 01 - Chance - Fletcher, Clinical Epidemiology The Essentials, 5th EditionDokumen19 halaman01 - Chance - Fletcher, Clinical Epidemiology The Essentials, 5th EditionDaniel PalmaBelum ada peringkat
- IHBAS ProspectusDokumen31 halamanIHBAS Prospectusshahmed999Belum ada peringkat
- Antibacterial Agents, NitrofuransDokumen8 halamanAntibacterial Agents, NitrofuransEmmanuel ChangBelum ada peringkat