Anda mungkin juga menyukai
- Journal Pre-Proof: Best Practice & Research Clinical Obstetrics & GynaecologyDokumen19 halamanJournal Pre-Proof: Best Practice & Research Clinical Obstetrics & GynaecologyGabriel Ferreira MassonBelum ada peringkat
- Obesity and Lung Disease: A Guide to ManagementDari EverandObesity and Lung Disease: A Guide to ManagementAnne E. DixonBelum ada peringkat
- ACOG Management of Stillbirth PDFDokumen14 halamanACOG Management of Stillbirth PDFLêMinhĐứcBelum ada peringkat
- Reducing Racial/Ethnic Disparities in Reproductive and Perinatal Outcomes: The Evidence from Population-Based InterventionsDari EverandReducing Racial/Ethnic Disparities in Reproductive and Perinatal Outcomes: The Evidence from Population-Based InterventionsArden HandlerBelum ada peringkat
- High Risk WomenDokumen17 halamanHigh Risk WomenamitBelum ada peringkat
- ABORTIONS AND ITS MANAGEMENT - FinalDokumen73 halamanABORTIONS AND ITS MANAGEMENT - FinalSamuel AdefemiBelum ada peringkat
- Interrelation of Liver & Kidney Parameter Changes Association With Hematological Changes of Patients With Dengue FeverDokumen6 halamanInterrelation of Liver & Kidney Parameter Changes Association With Hematological Changes of Patients With Dengue FeverSALT Journal of Scientific Research in HealthcareBelum ada peringkat
- Postterm Pregnancy - UpToDateDokumen17 halamanPostterm Pregnancy - UpToDateJosé Abraham Amaya DuarteBelum ada peringkat
- Fetal DeathDokumen15 halamanFetal DeathYasmin AlqadriBelum ada peringkat
- Practice Bulletin No 144 Multifetal Gestations .40Dokumen15 halamanPractice Bulletin No 144 Multifetal Gestations .40Jose Luis Morales Bautista100% (1)
- Spontaneous Abortion - Risk Factors, Etiology, Clinical Manifestations, and Diagnostic Evaluation - UpToDate PDFDokumen23 halamanSpontaneous Abortion - Risk Factors, Etiology, Clinical Manifestations, and Diagnostic Evaluation - UpToDate PDFPaula Grtrs WstrmrBelum ada peringkat
- Spontaneous AbortionDokumen17 halamanSpontaneous Abortionanon_985338331Belum ada peringkat
- 09_chapter 2Dokumen43 halaman09_chapter 2Vishnu Pragash ABelum ada peringkat
- Induced Abortion and Risks That May Impact AdolescentsDokumen29 halamanInduced Abortion and Risks That May Impact AdolescentsMichael RezaBelum ada peringkat
- Embarazo MultipleDokumen15 halamanEmbarazo MultipleLina E. ArangoBelum ada peringkat
- ACOG Practice Bulletin Prevencion PPDokumen10 halamanACOG Practice Bulletin Prevencion PPFelipe LlanosBelum ada peringkat
- Miscarriage in India: A Population-Based Study: Tervals, Because It Was Not Possible From The Data Set ToDokumen3 halamanMiscarriage in India: A Population-Based Study: Tervals, Because It Was Not Possible From The Data Set ToMutianaUmminyaKhanzaBelum ada peringkat
- Clinical Risk Factor For Preterm BirthDokumen22 halamanClinical Risk Factor For Preterm BirthGabyBffBelum ada peringkat
- Jurnal Ilmiah Kohesi Vol. 1 No. 3 Oktober 2017 ISSN: 2579-5872Dokumen10 halamanJurnal Ilmiah Kohesi Vol. 1 No. 3 Oktober 2017 ISSN: 2579-5872EXODUSGENBelum ada peringkat
- 1 s2.0 S1521693420300961 MainDokumen8 halaman1 s2.0 S1521693420300961 MainFloida Rose KatterBelum ada peringkat
- Deep Vein Thrombosis in Pregnancy - Epidemiology, Pathogenesis, and Diagnosis - UpToDateDokumen26 halamanDeep Vein Thrombosis in Pregnancy - Epidemiology, Pathogenesis, and Diagnosis - UpToDateCristinaCaprosBelum ada peringkat
- Obstetrics V13 Obstetric Emergencies Chapter Epidemiology of Extreme Maternal Morbidity and Maternal Mortality 1710573094Dokumen11 halamanObstetrics V13 Obstetric Emergencies Chapter Epidemiology of Extreme Maternal Morbidity and Maternal Mortality 1710573094antidius johnBelum ada peringkat
- Review Article: Maternal Preeclampsia and Neonatal OutcomesDokumen8 halamanReview Article: Maternal Preeclampsia and Neonatal OutcomesMita RestuBelum ada peringkat
- Analytical Study of Intrauterine Fetal Death Cases and Associated Maternal ConditionsDokumen5 halamanAnalytical Study of Intrauterine Fetal Death Cases and Associated Maternal ConditionsNurvita WidyastutiBelum ada peringkat
- Obsgyn 5Dokumen8 halamanObsgyn 5Teguh SulistiyantoBelum ada peringkat
- Preventing non-medically indicated late preterm and early term birthsDokumen14 halamanPreventing non-medically indicated late preterm and early term birthsAnuradha DissanayakeBelum ada peringkat
- Original Research Paper Pregnancy-Related Deaths: A Three-Year Retrospective StudyDokumen4 halamanOriginal Research Paper Pregnancy-Related Deaths: A Three-Year Retrospective StudySiva PrasadBelum ada peringkat
- Jurnal 10 PDFDokumen8 halamanJurnal 10 PDFFirman MufidBelum ada peringkat
- Multiparity FinalDokumen4 halamanMultiparity FinalUkwuma Michael ChijiokeBelum ada peringkat
- Multiparity and Childbirth Complication in Rural Women of Northeastern NigeriaDokumen14 halamanMultiparity and Childbirth Complication in Rural Women of Northeastern NigeriaUkwuma Michael ChijiokeBelum ada peringkat
- Postterm Pregnancy - UpToDateDokumen16 halamanPostterm Pregnancy - UpToDateCarlos Jeiner Díaz SilvaBelum ada peringkat
- Factors That Contribute to Early Pregnancy LossDokumen22 halamanFactors That Contribute to Early Pregnancy LosscacaBelum ada peringkat
- Epidemiology of Infertility and Recurrent Pregnancy Loss in Society With Fewer ChildrenDokumen6 halamanEpidemiology of Infertility and Recurrent Pregnancy Loss in Society With Fewer ChildrenDavid AdityaBelum ada peringkat
- Chapter 3Dokumen32 halamanChapter 3Vaibhav JainBelum ada peringkat
- GestationDokumen2 halamanGestationMustaf MohamedBelum ada peringkat
- Diabetic-Associated Stillbirth: Incidence, Pathophysiology, and PreventionDokumen16 halamanDiabetic-Associated Stillbirth: Incidence, Pathophysiology, and PreventionInas TsurayyaBelum ada peringkat
- Evaluation of Fetal Death: Causes, Diagnosis and ManagementDokumen12 halamanEvaluation of Fetal Death: Causes, Diagnosis and ManagementQoniek Nuzulul FalakhiBelum ada peringkat
- Abortion, What Is ItDokumen3 halamanAbortion, What Is ItAssero EricBelum ada peringkat
- BBLRDokumen8 halamanBBLRSVENPRIBelum ada peringkat
- Inherited and Acquired Thrombophilia - Pregnancy Outcome and TreatmentDokumen22 halamanInherited and Acquired Thrombophilia - Pregnancy Outcome and TreatmentLuiza RadulescuBelum ada peringkat
- This Is From Web. Credits To The OwnerDokumen40 halamanThis Is From Web. Credits To The OwnerYanna Habib-MangotaraBelum ada peringkat
- Urinary Tract Infections and Asymptomatic Bacteriuria in Pregnancy - UpToDateDokumen20 halamanUrinary Tract Infections and Asymptomatic Bacteriuria in Pregnancy - UpToDateEdward MarteBelum ada peringkat
- Aging and Infertility in WomenDokumen5 halamanAging and Infertility in Womendoc.GBelum ada peringkat
- Medical Jurisprudence ProjectDokumen11 halamanMedical Jurisprudence ProjectUtkarshini VermaBelum ada peringkat
- Care in Pregnancies Subsequent To Stillbirthor Perinatal DeatDokumen12 halamanCare in Pregnancies Subsequent To Stillbirthor Perinatal DeatgalalBelum ada peringkat
- Incomplete AbortionDokumen18 halamanIncomplete AbortionAra DirganBelum ada peringkat
- JGWH - Ms.id.555623 1 KirimDokumen6 halamanJGWH - Ms.id.555623 1 KirimBaiq Bunga Citra PratiwiBelum ada peringkat
- Causes, Stages and Risk Factors of Spontaneous MiscarriageDokumen28 halamanCauses, Stages and Risk Factors of Spontaneous MiscarriagetamaBelum ada peringkat
- Advanced Maternal Age & PregnancyDokumen67 halamanAdvanced Maternal Age & PregnancyMa Pilar Peñaflor AñonuevoBelum ada peringkat
- In Vitro Fertilization For M6 Students: YL TsaiDokumen49 halamanIn Vitro Fertilization For M6 Students: YL TsaiLee BoborasBelum ada peringkat
- App 2021 AcogDokumen26 halamanApp 2021 AcogFernanda Copete Yolianis100% (1)
- Causes and Risks of Gestational Hypertensive Disorders: Student's Name Submission DateDokumen24 halamanCauses and Risks of Gestational Hypertensive Disorders: Student's Name Submission DateAbd HasanBelum ada peringkat
- Parity and Maternal Illness and The Incidence of IDokumen6 halamanParity and Maternal Illness and The Incidence of ICarelle Faith Serrano AsuncionBelum ada peringkat
- Pregnancy, ectopic: An endovaginal sonogram reveals key findingsDokumen15 halamanPregnancy, ectopic: An endovaginal sonogram reveals key findingsAjay SapkaleBelum ada peringkat
- Dafpus Abortus 3Dokumen16 halamanDafpus Abortus 3ShintungBelum ada peringkat
- Chapter 1 Reproductive Health EpidemiologyyDokumen13 halamanChapter 1 Reproductive Health EpidemiologyyAnnisa NurrachmawatiBelum ada peringkat
- Incidence and Mortality of The Preterm Infant - UpToDateDokumen29 halamanIncidence and Mortality of The Preterm Infant - UpToDateAyu Dyah PrimaningrumBelum ada peringkat
- Eklampsia JurnalDokumen10 halamanEklampsia JurnalmerryBelum ada peringkat
- Fetomaternal Outcome in Advanced Maternal Age Protocol PDFDokumen25 halamanFetomaternal Outcome in Advanced Maternal Age Protocol PDFGetlozzAwabaBelum ada peringkat
- 1472 6882 6 39Dokumen8 halaman1472 6882 6 39Endah RizkiiBelum ada peringkat
- 2018 Weekly Calendar - Starts With Monday: This Excel Calendar Is Blank & Designed For Easy Use As A PlannerDokumen3 halaman2018 Weekly Calendar - Starts With Monday: This Excel Calendar Is Blank & Designed For Easy Use As A PlannerrestuwidianaBelum ada peringkat
- Freepik Premium License TermsDokumen1 halamanFreepik Premium License TermsNguyen Viet Trung (FPL HCMK13.3)100% (1)
- DX STD and Classification of TBC in ATSDokumen20 halamanDX STD and Classification of TBC in ATSAeris YeapBelum ada peringkat
- Movement Disorder ApproachDokumen9 halamanMovement Disorder ApproachSurat TanprawateBelum ada peringkat
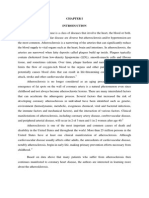
- AtherosclerosisDokumen11 halamanAtherosclerosisPande Indra PremanaBelum ada peringkat
- JurnalDokumen11 halamanJurnalrestuwidianaBelum ada peringkat
- Bleeding in Early PregnancyDokumen25 halamanBleeding in Early PregnancyAnnapurna DangetiBelum ada peringkat
- Mola Hidantidosa & Gestational Trophoblastic NeoplasmaDokumen23 halamanMola Hidantidosa & Gestational Trophoblastic NeoplasmanurkamilawatiBelum ada peringkat
- Maersk VN - Benefit Summary - Staff - 2020 (En)Dokumen36 halamanMaersk VN - Benefit Summary - Staff - 2020 (En)Thanh TraBelum ada peringkat
- Choriocarcinoma 11Dokumen23 halamanChoriocarcinoma 11Fakhir HasanBelum ada peringkat
- Management of Pregnancy Related BleedingDokumen75 halamanManagement of Pregnancy Related BleedingChuah Wei Hong100% (1)
- Cad Module 11 23 Unit1 Unit5 ReviewerDokumen47 halamanCad Module 11 23 Unit1 Unit5 ReviewerJelmar CastuloBelum ada peringkat
- Multiple Pregnancy - PPTX Md3Dokumen41 halamanMultiple Pregnancy - PPTX Md3Brother George100% (1)
- Great Medic Shield + Gms ExtenderDokumen16 halamanGreat Medic Shield + Gms ExtenderAthpotharaathi ManavalanBelum ada peringkat
- 2 PDFDokumen297 halaman2 PDFTaj KoyyodeBelum ada peringkat
- TEST II Community Health Nursing and Care of The Mother and Child XDDokumen11 halamanTEST II Community Health Nursing and Care of The Mother and Child XDraquel maniegoBelum ada peringkat
- UroginDokumen13 halamanUroginShandy Suwanto PutraBelum ada peringkat
- FinalDokumen45 halamanFinalRanvidsBelum ada peringkat
- Documents HUMSS C GROUP 3Dokumen10 halamanDocuments HUMSS C GROUP 3jerica joaquinBelum ada peringkat
- Preterm Birth - Risk Factors, Interventions For Risk Reduction, and Maternal Prognosis - UpToDateDokumen55 halamanPreterm Birth - Risk Factors, Interventions For Risk Reduction, and Maternal Prognosis - UpToDateArnold Yesid Rivas ZapataBelum ada peringkat
- High Risk PregnancyDokumen35 halamanHigh Risk PregnancykenBelum ada peringkat
- Prenatal Testing in Genetic Mutation Carrrier ParentsDokumen36 halamanPrenatal Testing in Genetic Mutation Carrrier ParentsJindal IVF ChandigarhBelum ada peringkat
- Krok 2 - 2023 (14 March) (General Medicine) - 1Dokumen19 halamanKrok 2 - 2023 (14 March) (General Medicine) - 1berdaderagaBelum ada peringkat
- Racheal Crane Babyloss Awareness Case Studies 20th March 2023Dokumen1 halamanRacheal Crane Babyloss Awareness Case Studies 20th March 2023api-286232866Belum ada peringkat
- Genetic Syndromes Associated With Isolated Fetal Growth Restriction PDFDokumen34 halamanGenetic Syndromes Associated With Isolated Fetal Growth Restriction PDFManuel GonzalezBelum ada peringkat
- BLA 761278 Lamzede PIDokumen15 halamanBLA 761278 Lamzede PINeethu Anna StephenBelum ada peringkat
- Killer Whales (Orcas) Unsuccessful Births by Mother's NameDokumen2 halamanKiller Whales (Orcas) Unsuccessful Births by Mother's NameThe Orca Project Corp100% (1)
- Incomplete Abortion Case StudyDokumen15 halamanIncomplete Abortion Case StudyJane Vi50% (6)
- PNLE II For Maternal and Child HealthDokumen13 halamanPNLE II For Maternal and Child HealthASDF ASDF100% (1)
- Obstetrics Gynecology Competencies e PDFDokumen22 halamanObstetrics Gynecology Competencies e PDFمركز ريلاكس للعلاج الطبيعيBelum ada peringkat
- OB/GYN For EMS ProvidersDokumen94 halamanOB/GYN For EMS ProvidersPaulhotvw67100% (6)
- Incompetent CervixDokumen29 halamanIncompetent CervixCyrelle Jen TorresBelum ada peringkat
- Maternity Benefit-Employer's ObligationsDokumen20 halamanMaternity Benefit-Employer's ObligationsSonika BhatiBelum ada peringkat
- Bedside Obstetrics and Gynecology 2010Dokumen564 halamanBedside Obstetrics and Gynecology 2010Nurul Wandasari S100% (2)
- NP2 Recalls 9Dokumen10 halamanNP2 Recalls 9AhrisJeannine EscuadroBelum ada peringkat
- Medyczny Słownik Angielsko-PolskiDokumen10 halamanMedyczny Słownik Angielsko-PolskiAnia JGBelum ada peringkat
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionDari EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionPenilaian: 4 dari 5 bintang4/5 (402)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessDari EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessPenilaian: 4.5 dari 5 bintang4.5/5 (327)
- The Age of Magical Overthinking: Notes on Modern IrrationalityDari EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityPenilaian: 4 dari 5 bintang4/5 (13)
- The Ultimate Guide To Memory Improvement TechniquesDari EverandThe Ultimate Guide To Memory Improvement TechniquesPenilaian: 5 dari 5 bintang5/5 (34)
- Techniques Exercises And Tricks For Memory ImprovementDari EverandTechniques Exercises And Tricks For Memory ImprovementPenilaian: 4.5 dari 5 bintang4.5/5 (40)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsDari EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsPenilaian: 3.5 dari 5 bintang3.5/5 (3)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeDari EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeBelum ada peringkat
- The Comfort of Crows: A Backyard YearDari EverandThe Comfort of Crows: A Backyard YearPenilaian: 4.5 dari 5 bintang4.5/5 (23)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedDari EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedPenilaian: 5 dari 5 bintang5/5 (78)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisDari EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisPenilaian: 4 dari 5 bintang4/5 (1)
- Why We Die: The New Science of Aging and the Quest for ImmortalityDari EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityPenilaian: 3.5 dari 5 bintang3.5/5 (2)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsDari EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsBelum ada peringkat
- The Obesity Code: Unlocking the Secrets of Weight LossDari EverandThe Obesity Code: Unlocking the Secrets of Weight LossPenilaian: 5 dari 5 bintang5/5 (3)
- The Happiness Trap: How to Stop Struggling and Start LivingDari EverandThe Happiness Trap: How to Stop Struggling and Start LivingPenilaian: 4 dari 5 bintang4/5 (1)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingDari EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingPenilaian: 5 dari 5 bintang5/5 (4)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingDari EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingPenilaian: 3.5 dari 5 bintang3.5/5 (31)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsDari EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsPenilaian: 4.5 dari 5 bintang4.5/5 (169)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaDari EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- The Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsDari EverandThe Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsBelum ada peringkat
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisDari EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisPenilaian: 4.5 dari 5 bintang4.5/5 (41)
- The Tennis Partner: A Doctor's Story of Friendship and LossDari EverandThe Tennis Partner: A Doctor's Story of Friendship and LossPenilaian: 4.5 dari 5 bintang4.5/5 (4)
- Summary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisDari EverandSummary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisPenilaian: 5 dari 5 bintang5/5 (3)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Dari EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Penilaian: 4.5 dari 5 bintang4.5/5 (110)
- Summary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisDari EverandSummary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisPenilaian: 5 dari 5 bintang5/5 (8)