Anda mungkin juga menyukai
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Ijerph 16 03937Dokumen14 halamanIjerph 16 03937anggaririnBelum ada peringkat
- The New Fifth-Generation Cephalosporins - A BalancDokumen7 halamanThe New Fifth-Generation Cephalosporins - A BalancanggaririnBelum ada peringkat
- Kumar 2017Dokumen31 halamanKumar 2017anggaririnBelum ada peringkat
- Cephalosporins Pharmacology and ChemistryDokumen5 halamanCephalosporins Pharmacology and ChemistryIrfan QaisarBelum ada peringkat
- Quino LoneDokumen28 halamanQuino LoneanggaririnBelum ada peringkat
- Harrison 2008Dokumen12 halamanHarrison 2008anggaririnBelum ada peringkat
- Nej Mo A 2118691Dokumen14 halamanNej Mo A 2118691anggaririnBelum ada peringkat
- Mechanisms Efflux Pumps of Acinetobacter To Antibiotics: Baumannii (MDR) : Increasing ResistanceDokumen23 halamanMechanisms Efflux Pumps of Acinetobacter To Antibiotics: Baumannii (MDR) : Increasing ResistanceanggaririnBelum ada peringkat
- Laboratory Procedure Manual: Cd4+ T-Lymphocytes and Cd8 T Cells Whole Blood Tricount MethodDokumen11 halamanLaboratory Procedure Manual: Cd4+ T-Lymphocytes and Cd8 T Cells Whole Blood Tricount MethodanggaririnBelum ada peringkat
- Jama Abbasi 2021 MN 210043 1627852635.57854Dokumen2 halamanJama Abbasi 2021 MN 210043 1627852635.57854anggaririnBelum ada peringkat
- Pi Is 1473309922002286Dokumen10 halamanPi Is 1473309922002286anggaririnBelum ada peringkat
- MonkeyfoxDokumen20 halamanMonkeyfoxanggaririnBelum ada peringkat
- BiomarkerDokumen18 halamanBiomarkeranggaririnBelum ada peringkat
- The Diagnostic Use of ADVIA 2120i Siemens and An "APL Criteria" CanDokumen9 halamanThe Diagnostic Use of ADVIA 2120i Siemens and An "APL Criteria" CananggaririnBelum ada peringkat
- A Simple Flow-Cytometry Method To Evaluate Peripheral Blood Contamination of BoneDokumen5 halamanA Simple Flow-Cytometry Method To Evaluate Peripheral Blood Contamination of BoneanggaririnBelum ada peringkat
- BD Trucount BeadsDokumen7 halamanBD Trucount BeadsanggaririnBelum ada peringkat
- A Copper Based Enzyme-Free Fluorescence ELISA For HER2 DetectionDokumen5 halamanA Copper Based Enzyme-Free Fluorescence ELISA For HER2 DetectionanggaririnBelum ada peringkat
- Art TerapiDokumen7 halamanArt TerapianggaririnBelum ada peringkat
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (74)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- DOCTO Consent FormDokumen6 halamanDOCTO Consent FormAnonymous 0vBpnRMpqVBelum ada peringkat
- Roland Berger - Pharmaceutical Industry Study 2009 - What Is NextDokumen40 halamanRoland Berger - Pharmaceutical Industry Study 2009 - What Is Nextapritul3539Belum ada peringkat
- John Wiley & SonsDokumen17 halamanJohn Wiley & SonsleretsantuBelum ada peringkat
- Drug Discovery and Drug DevelopmentDokumen20 halamanDrug Discovery and Drug DevelopmentsilviaBelum ada peringkat
- Biostatistics Classes Till 11.10.20Dokumen265 halamanBiostatistics Classes Till 11.10.20Md.Siddiqur RahmanBelum ada peringkat
- Director Clinical Operations in Philadelphia PA Resume Michelle AltonDokumen4 halamanDirector Clinical Operations in Philadelphia PA Resume Michelle AltonMichelleAltonBelum ada peringkat
- GCP 13 PrinciplesDokumen1 halamanGCP 13 Principlesshaik_firozBelum ada peringkat
- Wellcome News 71Dokumen36 halamanWellcome News 71Wellcome TrustBelum ada peringkat
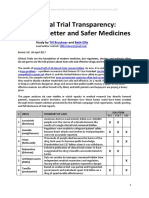
- Clinical Trial Transparency - A Key To Better and Safer Medicines (Till Bruckner and Beth Ellis 2017)Dokumen21 halamanClinical Trial Transparency - A Key To Better and Safer Medicines (Till Bruckner and Beth Ellis 2017)Till BrucknerBelum ada peringkat
- H5773e PDFDokumen83 halamanH5773e PDFPatrick PerezBelum ada peringkat
- Board Exam Compilation Book 2Dokumen163 halamanBoard Exam Compilation Book 2Aaron Cy Untalan100% (6)
- Off-Label Prescribing For Allergic Diseases in Pre-School ChildrenDokumen6 halamanOff-Label Prescribing For Allergic Diseases in Pre-School ChildrenrizkaBelum ada peringkat
- Wockhardt Annual Report 2022 2023Dokumen264 halamanWockhardt Annual Report 2022 2023ashwin moviesBelum ada peringkat
- 38 The Use of Meta-Analysis in Pharmacoepidemiology: Jesse A. BerlinDokumen27 halaman38 The Use of Meta-Analysis in Pharmacoepidemiology: Jesse A. BerlinFranklin garryBelum ada peringkat
- Mock Questions 2Dokumen40 halamanMock Questions 2Kamlesh KishorBelum ada peringkat
- Research Methods A Framework For Evidence-Based Clinical PracticeDokumen450 halamanResearch Methods A Framework For Evidence-Based Clinical PracticeAle Ramírez100% (1)
- Case Study On Royalty Pharma (109104)Dokumen25 halamanCase Study On Royalty Pharma (109104)gamerzgamerzBelum ada peringkat
- Miracle Check Point 1Dokumen60 halamanMiracle Check Point 1Henny Zahrany100% (2)
- Palin Parent Child Interaction and The Lidcombe Program: Clarifying Some IssuesDokumen8 halamanPalin Parent Child Interaction and The Lidcombe Program: Clarifying Some IssuesMinkushBelum ada peringkat
- Questions For Controlled TrialDokumen5 halamanQuestions For Controlled TrialTiaz Diniutami100% (1)
- 2021 DPharm - Clinical InkDokumen8 halaman2021 DPharm - Clinical InkEd SeguineBelum ada peringkat
- Autism Update Report 140929 PDFDokumen519 halamanAutism Update Report 140929 PDFBianca AngelescuBelum ada peringkat
- Animal Testing: Pros and ConsDokumen11 halamanAnimal Testing: Pros and ConsabhishekjainitBelum ada peringkat
- Opinion in Vanda Pharm. - Inc. v. FDA - 436 F. Supp. 3d 256Dokumen15 halamanOpinion in Vanda Pharm. - Inc. v. FDA - 436 F. Supp. 3d 256Kirk HartleyBelum ada peringkat
- NPC 10 12 2015Dokumen240 halamanNPC 10 12 2015SyaefudinBelum ada peringkat
- Early Childhood Edcation in PakistanDokumen95 halamanEarly Childhood Edcation in Pakistanmadihan00rBelum ada peringkat
- World Health Organization Study Concludes Risk of Suffering Serious Injury Due To COVID Vaccination IDokumen6 halamanWorld Health Organization Study Concludes Risk of Suffering Serious Injury Due To COVID Vaccination IZsolt Andras FerenczBelum ada peringkat
- Appi Books 9780890426807Dokumen218 halamanAppi Books 9780890426807Heidy Bravo RamosBelum ada peringkat
- Technical Update On Physiology Amniotic FluidDokumen7 halamanTechnical Update On Physiology Amniotic FluidIqra AnugerahBelum ada peringkat
- LB ClinTrialsDokumen23 halamanLB ClinTrialsmelissaisostdBelum ada peringkat