Anda mungkin juga menyukai
- Ultrasound in Acute Kidney InjuryDokumen70 halamanUltrasound in Acute Kidney InjuryaandakuBelum ada peringkat
- Understanding Chronic Kidney Disease: A guide for the non-specialistDari EverandUnderstanding Chronic Kidney Disease: A guide for the non-specialistPenilaian: 4 dari 5 bintang4/5 (3)
- 05 Smallpox and The First VaccineDokumen34 halaman05 Smallpox and The First VaccineRoman Bystrianyk100% (2)
- Chronic Kidney Disease - 2023Dokumen51 halamanChronic Kidney Disease - 2023ramadhanadlansyah7100% (1)
- Neinstein's Adolescent and Young Adult Health Care - A Practical Guide (6th Ed)Dokumen2.233 halamanNeinstein's Adolescent and Young Adult Health Care - A Practical Guide (6th Ed)angelashan100% (8)
- Health Management Contract Guidelines For Clients and ContractorsDokumen12 halamanHealth Management Contract Guidelines For Clients and ContractorsInternational Association of Oil and Gas ProducersBelum ada peringkat
- CKD UnsoedDokumen42 halamanCKD UnsoedSutan Malik IbrahimBelum ada peringkat
- Chronickidneydisease: Cornelia Charles,, Allison H. FerrisDokumen11 halamanChronickidneydisease: Cornelia Charles,, Allison H. FerrisDiahBelum ada peringkat
- Chronic Kidney Disease: The BasicsDokumen56 halamanChronic Kidney Disease: The BasicsAlmas Safina KauserBelum ada peringkat
- COPDs DR Moses KazevuDokumen30 halamanCOPDs DR Moses KazevuMoses Jr KazevuBelum ada peringkat
- Chronic Kidney DiseaseDokumen42 halamanChronic Kidney DiseaseLeta GemechuBelum ada peringkat
- PCP in A Box - Module 1Dokumen43 halamanPCP in A Box - Module 1Fate ChanBelum ada peringkat
- Renal FailureDokumen17 halamanRenal FailureNursidar Pascual MukattilBelum ada peringkat
- Reviews: Early Detection of CKD: The Benefits, Limitations and Effects On PrognosisDokumen12 halamanReviews: Early Detection of CKD: The Benefits, Limitations and Effects On Prognosisanderson roberto oliveira de sousaBelum ada peringkat
- Boala Cronica de Rinichi Adrian CovicDokumen85 halamanBoala Cronica de Rinichi Adrian CovicLorenaBelum ada peringkat
- PPT CKDDokumen35 halamanPPT CKDCandice LavigneBelum ada peringkat
- Pulsenotes - Chronic Kidney Disease NotesDokumen12 halamanPulsenotes - Chronic Kidney Disease NotesElay PedrosoBelum ada peringkat
- Chronic Kidney Disease Bhakti MuliaDokumen24 halamanChronic Kidney Disease Bhakti MuliaCOVID RSHJBelum ada peringkat
- Preventif CKD FinalDokumen43 halamanPreventif CKD Finaltika.dyahmustikaBelum ada peringkat
- Pathophysiology and Classification of Kidney DiseasesDokumen10 halamanPathophysiology and Classification of Kidney DiseasesmedicalBelum ada peringkat
- Diabetic Conference 2 (1) RenalDokumen20 halamanDiabetic Conference 2 (1) RenalWarren DonaldsonBelum ada peringkat
- Anesthesia For Kidney DiseaseDokumen6 halamanAnesthesia For Kidney DiseaseFrits Dede SinagaBelum ada peringkat
- Chronic Renal DiseaseDokumen7 halamanChronic Renal DiseaseDr-Dalya ShakirBelum ada peringkat
- Diagnostic Approach To Chronic Kidney DiseaseDokumen3 halamanDiagnostic Approach To Chronic Kidney DiseaseBlomblom Pow00Belum ada peringkat
- Jurnal Reading: Sit Dolor AmetDokumen20 halamanJurnal Reading: Sit Dolor AmetLiri AndiyaniBelum ada peringkat
- Buku CKD ManagementDokumen27 halamanBuku CKD ManagementPutri Atthariq IlmiBelum ada peringkat
- Management of Chronic Kidney Disease: Patient Population: ObjectivesDokumen27 halamanManagement of Chronic Kidney Disease: Patient Population: ObjectivesNadya SaptarinaBelum ada peringkat
- CKD 2016Dokumen39 halamanCKD 2016husnaBelum ada peringkat
- Jurding CKD Edit-1Dokumen20 halamanJurding CKD Edit-1Asmaul HabibiBelum ada peringkat
- Mayoclinproc 84 2 012 PDFDokumen7 halamanMayoclinproc 84 2 012 PDFVinceErwinTanBelum ada peringkat
- Chronic Kidney DiseaseDokumen14 halamanChronic Kidney DiseaseJoel CanenciaBelum ada peringkat
- Drug-Induced Kidney DiseasesDokumen10 halamanDrug-Induced Kidney DiseasesMubashar ShahidBelum ada peringkat
- AKI Vs CKD Lecture Latest 3rd Dec 2018Dokumen51 halamanAKI Vs CKD Lecture Latest 3rd Dec 2018mugilessBelum ada peringkat
- CKD SheetDokumen4 halamanCKD SheetMomy SutanBelum ada peringkat
- 22-12 - Chronic Kidney DiseaseDokumen19 halaman22-12 - Chronic Kidney DiseaseSergio VasquezBelum ada peringkat
- A Review On Dose Adjusment in Renal Failure Patients: European Journal of Pharmaceutical and Medical ResearchDokumen6 halamanA Review On Dose Adjusment in Renal Failure Patients: European Journal of Pharmaceutical and Medical Researchvyta100% (1)
- AKI Perioperatif 3Dokumen6 halamanAKI Perioperatif 3Kevin JohanesBelum ada peringkat
- Causes of Acute Deterioration in Chronic Kidney DiseaseDokumen3 halamanCauses of Acute Deterioration in Chronic Kidney DiseaseSitLus ChannelBelum ada peringkat
- CKD PresentationDokumen83 halamanCKD PresentationMoh'md NuohBelum ada peringkat
- CKD and Uti-2Dokumen9 halamanCKD and Uti-2Corazon Arellano RamosBelum ada peringkat
- Chronic Kidney DiseaseDokumen18 halamanChronic Kidney DiseaseAde Cahyo IslamiBelum ada peringkat
- CKD PDFDokumen6 halamanCKD PDFmkafabillahBelum ada peringkat
- Chronic Kidney DiseaseDokumen18 halamanChronic Kidney DiseaseAde Cahyo IslamiBelum ada peringkat
- Acute Kidney Injury: Current Concepts and New Insights: Key WordsDokumen5 halamanAcute Kidney Injury: Current Concepts and New Insights: Key WordsIHBelum ada peringkat
- DefisniDokumen41 halamanDefisniAzizah MBelum ada peringkat
- Gagal Ginjal Kronik FarmakoDokumen28 halamanGagal Ginjal Kronik FarmakoIkhza Yasyifa RusydaBelum ada peringkat
- Fluid and Electrolyte Problems in Renal DysfunctionDokumen5 halamanFluid and Electrolyte Problems in Renal Dysfunctionfachrudin arBelum ada peringkat
- Chronic Kidney Disease: Presented By, Mariya Antony 3 Year BSC Nursing ST - Thomas College of Nursing ChethipuzhaDokumen62 halamanChronic Kidney Disease: Presented By, Mariya Antony 3 Year BSC Nursing ST - Thomas College of Nursing ChethipuzhaSamuel LalBelum ada peringkat
- Insuficiencia Renal Aguda: Acute Kidney InjuryDokumen10 halamanInsuficiencia Renal Aguda: Acute Kidney InjuryVitor Hugo G CorreiaBelum ada peringkat
- Chronic Kidney Disease (CKD) : Provider's Guide To Diagnose and Code CKDDokumen2 halamanChronic Kidney Disease (CKD) : Provider's Guide To Diagnose and Code CKDAry Rio PambudiBelum ada peringkat
- Ijda 5 024 PDFDokumen5 halamanIjda 5 024 PDFKumarsai DurusojuBelum ada peringkat
- Chronic Kidney Disease: Rizki Aliana AgustinaDokumen85 halamanChronic Kidney Disease: Rizki Aliana AgustinaRofi IrmanBelum ada peringkat
- Onconephrology: Update in Anticancer Drug-Related NephrotoxicityDokumen13 halamanOnconephrology: Update in Anticancer Drug-Related NephrotoxicityFreddy Shanner Chávez VásquezBelum ada peringkat
- Joacp 28 386Dokumen11 halamanJoacp 28 386KrisztinaBelum ada peringkat
- Chronic Renal Disease: Data Supplement ReferencesDokumen7 halamanChronic Renal Disease: Data Supplement ReferencesmedcrgBelum ada peringkat
- Chapter 102 Medical Management of The Kidney Transplant Recipient Cardiovascular Disease and Other IssuesDokumen11 halamanChapter 102 Medical Management of The Kidney Transplant Recipient Cardiovascular Disease and Other Issuesadrian mendoza croesBelum ada peringkat
- CKD PDFDokumen20 halamanCKD PDFReyhan TarisBelum ada peringkat
- Actualizaciones Sobre La Enfermedad Renal PoliquísticaDokumen45 halamanActualizaciones Sobre La Enfermedad Renal PoliquísticaEvelyn CaveroBelum ada peringkat
- CHRONIC KIDNEY DISEASE Pelatihan Perawat HD 2021Dokumen33 halamanCHRONIC KIDNEY DISEASE Pelatihan Perawat HD 2021Yudha WirawanBelum ada peringkat
- How To Improve Outcomes in Hemodialysis PatientsDokumen24 halamanHow To Improve Outcomes in Hemodialysis PatientsSuardy CiayadiBelum ada peringkat
- Chronic Kidney Disease in Primary Care: Duaine D. Murphree, MD, and Sarah M. Thelen, MDDokumen11 halamanChronic Kidney Disease in Primary Care: Duaine D. Murphree, MD, and Sarah M. Thelen, MDMawarBelum ada peringkat
- L11 Renal Failure General Approach 230213 002819Dokumen16 halamanL11 Renal Failure General Approach 230213 002819S sBelum ada peringkat
- Restoring Chronic Kidney Disease : Restoring, Preserving, and Improving CKD to Avoid DialysisDari EverandRestoring Chronic Kidney Disease : Restoring, Preserving, and Improving CKD to Avoid DialysisBelum ada peringkat
- Tuberculosis Vih EthiopiaDokumen9 halamanTuberculosis Vih Ethiopiajulma1306Belum ada peringkat
- Keane Et Al-2012-HIV MedicineDokumen6 halamanKeane Et Al-2012-HIV Medicinejulma1306Belum ada peringkat
- Hepatitis E AustraliaDokumen3 halamanHepatitis E Australiajulma1306Belum ada peringkat
- Hepatitis E CaliforniaDokumen3 halamanHepatitis E Californiajulma1306Belum ada peringkat
- 12 10 4487 KBB ClinicalUpdateOnAlternateiveVADokumen4 halaman12 10 4487 KBB ClinicalUpdateOnAlternateiveVAjulma1306Belum ada peringkat
- Zoonotic and Foodborne Trnasmition of Hepatitis EDokumen9 halamanZoonotic and Foodborne Trnasmition of Hepatitis Ejulma1306Belum ada peringkat
- An Emerging Diseade Hepatitis EDokumen20 halamanAn Emerging Diseade Hepatitis Ejulma1306Belum ada peringkat
- Lymphoma HandoutDokumen5 halamanLymphoma Handoutapi-244850728Belum ada peringkat
- 44transboundary Environmental Issues Intra-ASEANZoonotic Diseases Affecting TDokumen4 halaman44transboundary Environmental Issues Intra-ASEANZoonotic Diseases Affecting Ttanmaya_purohitBelum ada peringkat
- In Memoriam Allan Cott, M.D. 1910-1993: Journal of Orthomolecular Medicine. He WasDokumen4 halamanIn Memoriam Allan Cott, M.D. 1910-1993: Journal of Orthomolecular Medicine. He WasSchwab RealHumanBelum ada peringkat
- Haematolgy MDT WebDokumen2 halamanHaematolgy MDT WebbfdboiiBelum ada peringkat
- Medical Excuse From Jury Duty TemplateDokumen2 halamanMedical Excuse From Jury Duty TemplateBalkiss TouzriBelum ada peringkat
- Tuberculosis Taking ControlDokumen9 halamanTuberculosis Taking Controlrkbhuvaneshwari32Belum ada peringkat
- Health-Care Workers' Occupational Exposures To Body Fluids in 21 Countries in Africa: Systematic Review and Meta-AnalysisDokumen17 halamanHealth-Care Workers' Occupational Exposures To Body Fluids in 21 Countries in Africa: Systematic Review and Meta-AnalysisgusdeBelum ada peringkat
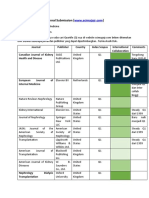
- Journal SubmissionDokumen3 halamanJournal SubmissionMaruhum Bonar MarbunBelum ada peringkat
- Mycoses - 2023 - Kato - A Systematic Review and Meta Analysis of Efficacy and Safety of Isavuconazole For The Treatment andDokumen10 halamanMycoses - 2023 - Kato - A Systematic Review and Meta Analysis of Efficacy and Safety of Isavuconazole For The Treatment andc gBelum ada peringkat
- Skills Assessment - Nursing-HomecareDokumen2 halamanSkills Assessment - Nursing-HomecareKatherine SamsBelum ada peringkat
- Weekly Epi Update 79Dokumen19 halamanWeekly Epi Update 79Lee Ji EunBelum ada peringkat
- CHN Post TestDokumen21 halamanCHN Post TestAngie RelosBelum ada peringkat
- A Simpler Prediction Rule For Rebound HyperbilirubinemiaDokumen7 halamanA Simpler Prediction Rule For Rebound HyperbilirubinemiaNoviaBelum ada peringkat
- Consumer Health EducationDokumen21 halamanConsumer Health Educationerwin espinosaBelum ada peringkat
- Nurs FPX 4020 Assessment 3 Improvement Plan in Service PresentationDokumen6 halamanNurs FPX 4020 Assessment 3 Improvement Plan in Service Presentationzadem5266Belum ada peringkat
- Abnormal NipplesDokumen1 halamanAbnormal NipplesdrpamiBelum ada peringkat
- Untitled Document - EditedDokumen2 halamanUntitled Document - EditedBenjamin MuriithiBelum ada peringkat
- The Effect of Relaxation Techniques and Distraction Techniques On Reducing Pain Scale in Postoperative Patients at UKI Hospital East Jakarta in 2020Dokumen10 halamanThe Effect of Relaxation Techniques and Distraction Techniques On Reducing Pain Scale in Postoperative Patients at UKI Hospital East Jakarta in 2020Lisa MaghfirahBelum ada peringkat
- Renal Psychology: Carolyn Evans, Sarah Cook, Joanne Taylor - Review Date Jan 2016Dokumen5 halamanRenal Psychology: Carolyn Evans, Sarah Cook, Joanne Taylor - Review Date Jan 2016oanacrisBelum ada peringkat
- Autism Spectrum Disorder (ASD) - Market Insights, Epidemiology & Market Forecast-2027 - Sample PagesDokumen25 halamanAutism Spectrum Disorder (ASD) - Market Insights, Epidemiology & Market Forecast-2027 - Sample PagesDelveInsight0% (1)
- Talcum Powder and CancerDokumen7 halamanTalcum Powder and CancerhasnizaBelum ada peringkat
- Manejo Del Choque Séptico: Jesús Nicolás Hidalgo DelgadoDokumen40 halamanManejo Del Choque Séptico: Jesús Nicolás Hidalgo DelgadoNicko HidalgoBelum ada peringkat
- Hafid M. Jabir 18710093Dokumen28 halamanHafid M. Jabir 18710093titin setya ningsihBelum ada peringkat
- Daftar Pustaka GlaukomaDokumen2 halamanDaftar Pustaka Glaukomakatherine rinovaBelum ada peringkat
- Afi Part 2Dokumen438 halamanAfi Part 2Dr AnandBelum ada peringkat
- Bcongress 2016Dokumen2 halamanBcongress 2016Christian RiveraBelum ada peringkat