Anda mungkin juga menyukai
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (345)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (74)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- New Health Care Clinical: Laboratory SrinagarDokumen1 halamanNew Health Care Clinical: Laboratory SrinagarRajaBelum ada peringkat
- Diabetes Jigsaw ActivitiesDokumen11 halamanDiabetes Jigsaw ActivitiesJacqueline CullieBelum ada peringkat
- Guide PDFDokumen84 halamanGuide PDFbiomeditechBelum ada peringkat
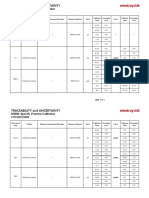
- Specific Proteins Calibrator-150721009-BS600Dokumen2 halamanSpecific Proteins Calibrator-150721009-BS600S6b2Belum ada peringkat
- Is Doa 10 Cup TestDokumen1 halamanIs Doa 10 Cup TestUqi.Belum ada peringkat
- Exercise PrescriptionDokumen53 halamanExercise PrescriptionEvangeline A. Alegre100% (1)
- NCPDokumen2 halamanNCPfierfizBelum ada peringkat
- Vesiculobullous LesionDokumen31 halamanVesiculobullous Lesionsara ibrahimBelum ada peringkat
- Myofascial Pain Dysfunction Syndrome - A RevisitDokumen9 halamanMyofascial Pain Dysfunction Syndrome - A RevisitRhea RejiBelum ada peringkat
- Icru 89 (229-260)Dokumen32 halamanIcru 89 (229-260)Christian Ordoñez100% (1)
- An Awareness Session On Blood Donation and Its ImportanceDokumen40 halamanAn Awareness Session On Blood Donation and Its Importancekushi krishnaBelum ada peringkat
- IDP 11.13.19 11.14.19 Metal Implants White Paper - 0 PDFDokumen152 halamanIDP 11.13.19 11.14.19 Metal Implants White Paper - 0 PDFVivek KhakharBelum ada peringkat
- Body Parts Governed by PlanetsDokumen2 halamanBody Parts Governed by PlanetsBratva Ankit Mishra100% (1)
- Pathophysiology of InflammationDokumen50 halamanPathophysiology of InflammationElla Jones0% (1)
- KSPCB BIOMEDICAL POSTER 1aDokumen1 halamanKSPCB BIOMEDICAL POSTER 1armulmadgiBelum ada peringkat
- Case Study of Most Common Communicable DiseasesDokumen13 halamanCase Study of Most Common Communicable DiseasesnesjynBelum ada peringkat
- Foundations of Operative Surgery An Introduction To Surgical TechniquesDokumen165 halamanFoundations of Operative Surgery An Introduction To Surgical TechniquesTeodora-Valeria TolanBelum ada peringkat
- Lesson Plan On Post Natal ExercisesDokumen11 halamanLesson Plan On Post Natal Exercisesvarshasharma0593% (15)
- Et TR MedDokumen99 halamanEt TR MedThe ScienceBelum ada peringkat
- F Buski 111003095909 Phpapp01Dokumen15 halamanF Buski 111003095909 Phpapp01Ashik MajumdarBelum ada peringkat
- Beth PRC FormDokumen11 halamanBeth PRC FormNev Bryan DapitanBelum ada peringkat
- r145274208 Isabella Fonseca CUR145274208Dokumen1 halamanr145274208 Isabella Fonseca CUR145274208Isabella FonsecaBelum ada peringkat
- Etamsylate DS Meppo2010 PDFDokumen3 halamanEtamsylate DS Meppo2010 PDFAqmarlia PutriBelum ada peringkat
- 1.0 Thrombocytes SCDokumen10 halaman1.0 Thrombocytes SC西矢椛Belum ada peringkat
- Ventilator Graphics & Trouble-Shooting - EditedDokumen64 halamanVentilator Graphics & Trouble-Shooting - EditedAbhishek SinghBelum ada peringkat
- Shah - Cancer of The Head and Neck PDFDokumen12 halamanShah - Cancer of The Head and Neck PDFElizabetha SalzcenBelum ada peringkat
- Feeling GreatDokumen243 halamanFeeling GreatSunny LamBelum ada peringkat
- PRE Test 1Dokumen15 halamanPRE Test 1Naomi VirtudazoBelum ada peringkat
- Brain AbscessDokumen13 halamanBrain AbscessRian AprizaBelum ada peringkat
- Extravasation Neutral (Non-Irritant) Irritant Irritant With Vesicant Properties VesicantsDokumen12 halamanExtravasation Neutral (Non-Irritant) Irritant Irritant With Vesicant Properties VesicantsmarcBelum ada peringkat