Anda mungkin juga menyukai
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (399)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (73)
- Acute Kidney Injury W/ Hyperkalemia NCPDokumen5 halamanAcute Kidney Injury W/ Hyperkalemia NCPMyrvic Ortiz La OrdenBelum ada peringkat
- Dental Public HealthDokumen264 halamanDental Public HealthCorina Manole DanielaBelum ada peringkat
- Prometric McqsDokumen30 halamanPrometric Mcqsjishan8250% (2)
- Understanding-Ocd 2016 v2Dokumen27 halamanUnderstanding-Ocd 2016 v2Samanjit Sen Gupta100% (1)
- 2014 Final Paediatric Exam (تم الحفظ تلقائيًا)Dokumen258 halaman2014 Final Paediatric Exam (تم الحفظ تلقائيًا)wea xcz100% (4)
- Nursing Practice (5th Ed.) - Pitman, Nursing: Assessment and Management of Clinical Problems (9th Ed.) - St. Louis: ElsevierDokumen5 halamanNursing Practice (5th Ed.) - Pitman, Nursing: Assessment and Management of Clinical Problems (9th Ed.) - St. Louis: ElsevierDr-Marudhar MarudharBelum ada peringkat
- Periapical Radiolucencies As Evaluated by Bisecting-Angle and Paralleling Radio Graphic TechniquesDokumen9 halamanPeriapical Radiolucencies As Evaluated by Bisecting-Angle and Paralleling Radio Graphic TechniquesFlorin Ionescu100% (1)
- Significance of Facebow Transfer: January 2020Dokumen6 halamanSignificance of Facebow Transfer: January 2020Mahmoud Ibrahem maanBelum ada peringkat
- ImmunosuppresentsDokumen13 halamanImmunosuppresentsmadeputraBelum ada peringkat
- CDN 1 PDFDokumen22 halamanCDN 1 PDFJohn Mark100% (1)
- Conscious Sedation PaediatricsDokumen44 halamanConscious Sedation PaediatricsReeta TaxakBelum ada peringkat
- Position Paper On Teenage PregnancyDokumen3 halamanPosition Paper On Teenage PregnancyMark Anthony CabangonBelum ada peringkat
- HEPATITIS B VACCINE NURSING RESPONSIBILITIESDokumen14 halamanHEPATITIS B VACCINE NURSING RESPONSIBILITIESJannine BensiBelum ada peringkat
- Understanding Traumatic Brain Injury (TBIDokumen16 halamanUnderstanding Traumatic Brain Injury (TBIdcBelum ada peringkat
- Final Written Lab Exam Form ADokumen4 halamanFinal Written Lab Exam Form AErvin T MileBelum ada peringkat
- PrimaquineDokumen3 halamanPrimaquineVijayakumar NsBelum ada peringkat
- Prolonged LaborDokumen13 halamanProlonged Laborsujinaranamagar18Belum ada peringkat
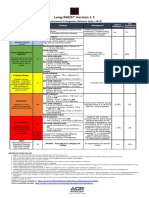
- Lung RADS® Version 1.1: Assessment Categories Release Date: 2019Dokumen1 halamanLung RADS® Version 1.1: Assessment Categories Release Date: 2019S Francisco MotBelum ada peringkat
- Chronic Suppurative Otitis Media PDFDokumen3 halamanChronic Suppurative Otitis Media PDFsarahBelum ada peringkat
- Retrograde Intubation Using Epidural Catheter - A Safe and Cost Effective Technique - A Case ReportDokumen2 halamanRetrograde Intubation Using Epidural Catheter - A Safe and Cost Effective Technique - A Case ReportIOSRjournalBelum ada peringkat
- Understanding the Benefits of Physical ActivitiesDokumen17 halamanUnderstanding the Benefits of Physical ActivitiesRealisan DulnuanBelum ada peringkat
- Chest Wall, Lung, Mediastinum, and Pleura ProceduresDokumen124 halamanChest Wall, Lung, Mediastinum, and Pleura ProceduresKenn BrillanteBelum ada peringkat
- Bladder Cancer Types, Symptoms, Tests & TreatmentDokumen1 halamanBladder Cancer Types, Symptoms, Tests & TreatmentCarmina AguilarBelum ada peringkat
- Case Study PneumothoraxDokumen9 halamanCase Study PneumothoraxLee_Cabral_693967% (3)
- Morpho - Pathology Final Summary: Chapter 1: Cellular Reactions To AggressionDokumen21 halamanMorpho - Pathology Final Summary: Chapter 1: Cellular Reactions To Aggressiondjxela89Belum ada peringkat
- Theory and Practice of Pure Tone Audiometry - PTADokumen12 halamanTheory and Practice of Pure Tone Audiometry - PTAsolhazBelum ada peringkat
- Not Eligible As No Experience of Teaching and ResearchDokumen5 halamanNot Eligible As No Experience of Teaching and ResearchVasanth Kumar AllaBelum ada peringkat
- Ann JeinaDokumen7 halamanAnn JeinaMizumoriFumairaBelum ada peringkat
- Psoriasis and Miracles With HomoeopathyDokumen3 halamanPsoriasis and Miracles With HomoeopathyEditor IJTSRDBelum ada peringkat
- Source Control in Emergency General SurgeryDokumen21 halamanSource Control in Emergency General SurgerylaviniaBelum ada peringkat