Anda mungkin juga menyukai
- What Went Wrong With The Achievement of Replacement Fertility in Bangladesh and Its Consequences On The Demographic Dividend The Role of Proximate DeterminantsDokumen24 halamanWhat Went Wrong With The Achievement of Replacement Fertility in Bangladesh and Its Consequences On The Demographic Dividend The Role of Proximate DeterminantsRussell KabirBelum ada peringkat
- Elderly Care in Bangladesh: Challenges in The New MillenniumDokumen12 halamanElderly Care in Bangladesh: Challenges in The New MillenniumRussell KabirBelum ada peringkat
- Electrocardiographic and Blood Electrolytes Findings in Athletic Students of Sports Academy in Bangladesh 2329 6879 1000218Dokumen4 halamanElectrocardiographic and Blood Electrolytes Findings in Athletic Students of Sports Academy in Bangladesh 2329 6879 1000218Russell KabirBelum ada peringkat
- Chikungunya Fever: An Emerging Public Health Problem in BangladeshDokumen5 halamanChikungunya Fever: An Emerging Public Health Problem in BangladeshRussell KabirBelum ada peringkat
- Relationship Between Contraceptive Prevalence Rate and Total Fertility Rate Revisiting The Empirical ModelDokumen14 halamanRelationship Between Contraceptive Prevalence Rate and Total Fertility Rate Revisiting The Empirical ModelRussell KabirBelum ada peringkat
- Exploring The Knowledge, Attitude and Practices Towards Use of Unprescribed Drugs Among Adults of A Selected City of SomalilandDokumen7 halamanExploring The Knowledge, Attitude and Practices Towards Use of Unprescribed Drugs Among Adults of A Selected City of SomalilandRussell KabirBelum ada peringkat
- Self Medication AntibioticsDokumen19 halamanSelf Medication AntibioticsRussell KabirBelum ada peringkat
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5795)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (589)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (400)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (74)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1091)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- 06 - SCM Academy - Purchasing Overview-EditedDokumen15 halaman06 - SCM Academy - Purchasing Overview-Editedalice.9Belum ada peringkat
- JP ResumeDokumen4 halamanJP ResumeLorilla AlvinBelum ada peringkat
- SEA PrizrenDokumen49 halamanSEA Prizrentom_hamm1008Belum ada peringkat
- History of Social CaseworkDokumen14 halamanHistory of Social Caseworknirmaljoy60% (5)
- Persuasive Speech Outline Draft 4Dokumen4 halamanPersuasive Speech Outline Draft 4AlexisBelum ada peringkat
- Delegates Schedule of FeesDokumen1 halamanDelegates Schedule of FeesAngelo Mark Ordoña PorgatorioBelum ada peringkat
- Bomba Denison PVDokumen34 halamanBomba Denison PVEdwin Quispe CarlosBelum ada peringkat
- (CS5043) Part 3Dokumen23 halaman(CS5043) Part 3Ahtsham GhaffarBelum ada peringkat
- Rsa536 16 26 10 2018Dokumen13 halamanRsa536 16 26 10 2018samsungindian 2015Belum ada peringkat
- Error Code List Ergopower-Est37/A: ZF Passau GMBHDokumen56 halamanError Code List Ergopower-Est37/A: ZF Passau GMBHTogu Marnaek SiagianBelum ada peringkat
- Chapter 1 (LMS)Dokumen35 halamanChapter 1 (LMS)Nhân TrịnhBelum ada peringkat
- Foreign LiteratureDokumen3 halamanForeign LiteratureAngeline HermosoBelum ada peringkat
- Document TitleDokumen5 halamanDocument Titlereyad binBelum ada peringkat
- Shantae ManualDokumen19 halamanShantae ManualJonathan Lesomthing100% (1)
- Topic: A Study On Awareness and Accessing Behavior Of: DEMAT Account in Rajpipla CityDokumen19 halamanTopic: A Study On Awareness and Accessing Behavior Of: DEMAT Account in Rajpipla CityBhavesh VasavaBelum ada peringkat
- Nordic District HeatDokumen52 halamanNordic District HeatFan DiBelum ada peringkat
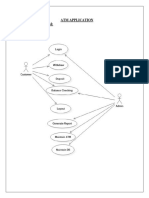
- Atm Application Use Case DiagramDokumen58 halamanAtm Application Use Case DiagramS. Mohd TharikBelum ada peringkat
- CCTV System Installation ChecklistDokumen5 halamanCCTV System Installation ChecklistAlvin Badz100% (1)
- Alberta Transportation Integral AbutmentDokumen13 halamanAlberta Transportation Integral AbutmentMehdi.MostBelum ada peringkat
- STRACOSMAN - Chapter 2Dokumen6 halamanSTRACOSMAN - Chapter 2Rae WorksBelum ada peringkat
- YEF Final ReportDokumen12 halamanYEF Final ReportNidhi SharmaBelum ada peringkat
- Family Managed Business Vs Non Family BusinessDokumen4 halamanFamily Managed Business Vs Non Family BusinessKARISHMA RAJ0% (1)
- Kvaerner Hydro VALVESDokumen24 halamanKvaerner Hydro VALVESEduardo CastilloBelum ada peringkat
- Class 10 AI NOTES CHAPTER 1Dokumen7 halamanClass 10 AI NOTES CHAPTER 1Vinayak Chaturvedi100% (4)
- Fabric EJDokumen20 halamanFabric EJOctama RizkyBelum ada peringkat
- Application Form For Entrance Exam 2020Dokumen2 halamanApplication Form For Entrance Exam 2020Ma.carmela AquinoBelum ada peringkat
- Digests PALEDokumen11 halamanDigests PALEInter_vivosBelum ada peringkat
- A01ES-DSP3+54B-D+FM2+YL5+PEA01 - APEM A01ES Series Emergency Stop Push Button, 1NC, Surface Mount, IP65 - RSDokumen3 halamanA01ES-DSP3+54B-D+FM2+YL5+PEA01 - APEM A01ES Series Emergency Stop Push Button, 1NC, Surface Mount, IP65 - RSrodinooBelum ada peringkat
- MODULE 1 Cafeteria by MJ RellonDokumen24 halamanMODULE 1 Cafeteria by MJ RellonTricia Ann A. SodsodBelum ada peringkat