Anda mungkin juga menyukai
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (890)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (587)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (119)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2219)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (73)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- HIPEC ProtocolDokumen7 halamanHIPEC ProtocolMariaBelum ada peringkat
- Doctor's Cancer Statement FormDokumen1 halamanDoctor's Cancer Statement FormANIS NAZREEN BT SODZIR -Belum ada peringkat
- What's New in The Management of Complex Tibial Plateau Fractures?Dokumen8 halamanWhat's New in The Management of Complex Tibial Plateau Fractures?juancrisBelum ada peringkat
- Spontaneous Regression of Septum Pellucidum-FornicealDokumen9 halamanSpontaneous Regression of Septum Pellucidum-FornicealjuancrisBelum ada peringkat
- Comparative Effects of Light or Heavy Resistance Power Training For Improving Lower Extremity Power and Physical Performance in Mobility-Limited Older AdultsDokumen7 halamanComparative Effects of Light or Heavy Resistance Power Training For Improving Lower Extremity Power and Physical Performance in Mobility-Limited Older AdultsjuancrisBelum ada peringkat
- A Comparison of Muscle Activations During Traditional and Abbreviated Tennis Serves.Dokumen13 halamanA Comparison of Muscle Activations During Traditional and Abbreviated Tennis Serves.juancrisBelum ada peringkat
- Cervical Cancer StagingDokumen35 halamanCervical Cancer StagingOttofianus Hewick KalangiBelum ada peringkat
- Skin Cancer: By: Kausthubhi KillamsettiDokumen33 halamanSkin Cancer: By: Kausthubhi KillamsettiKausthubhi KillamsettiBelum ada peringkat
- Manage Solitary Thyroid NodulesDokumen6 halamanManage Solitary Thyroid NodulesSathiyamoorthy KarunakaranBelum ada peringkat
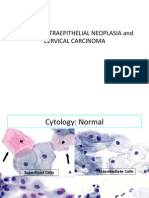
- 04 CIN and Cervical Cancer UNEDITEDDokumen120 halaman04 CIN and Cervical Cancer UNEDITEDRalph JuicoBelum ada peringkat
- Role of Imaging in Cancer Detection, Diagnosis and TreatmentDokumen30 halamanRole of Imaging in Cancer Detection, Diagnosis and TreatmentAnshul VarshneyBelum ada peringkat
- (23006676 - Current Issues in Pharmacy and Medical Sciences) Gastric LipomatosisDokumen3 halaman(23006676 - Current Issues in Pharmacy and Medical Sciences) Gastric LipomatosisPockets Ain't EmptyBelum ada peringkat
- Ivermectin Potential Anticancer DrugDokumen11 halamanIvermectin Potential Anticancer DrugJesus Bueno MorenoBelum ada peringkat
- Benign Skin TumoursDokumen7 halamanBenign Skin TumoursMan LorBelum ada peringkat
- Histopathological Reporting of ColorectalDokumen76 halamanHistopathological Reporting of ColorectalJohn SmithyBelum ada peringkat
- Antitumor Activity of A Benzaldehyde DerivativeDokumen2 halamanAntitumor Activity of A Benzaldehyde DerivativeAlberto BrevettoBelum ada peringkat
- Biochimica Et Biophysica ActaDokumen7 halamanBiochimica Et Biophysica ActaSelin AktaşBelum ada peringkat
- Volume3 Issue4 Jul Aug No.329 665 667Dokumen3 halamanVolume3 Issue4 Jul Aug No.329 665 667MadeKurniawanAsBelum ada peringkat
- Advanced Imaging Modalities PDFDokumen94 halamanAdvanced Imaging Modalities PDFJohnQ100% (1)
- Breast CalcificationsDokumen2 halamanBreast CalcificationsmoeBelum ada peringkat
- Treatment of Differentiated Thyroid Cancers with Tyrosine Kinase InhibitorsDokumen28 halamanTreatment of Differentiated Thyroid Cancers with Tyrosine Kinase InhibitorsSameer FasihBelum ada peringkat
- Distant Metastases of Nasopharyngeal Carcinoma: Literature ReadingDokumen33 halamanDistant Metastases of Nasopharyngeal Carcinoma: Literature ReadingTeuku Muhammad Rizqi FadhlillahBelum ada peringkat
- Ewings SarcomaDokumen9 halamanEwings SarcomaElvisBelum ada peringkat
- Evaluation of Serum and Tissue MagnesiumDokumen11 halamanEvaluation of Serum and Tissue Magnesiumeylül kayaBelum ada peringkat
- Scenario: (Everyone Said No)Dokumen4 halamanScenario: (Everyone Said No)Muthia KarinaBelum ada peringkat
- Medicineand Medical Research. 1 (1) : 24-24.: Daftar PustakaDokumen6 halamanMedicineand Medical Research. 1 (1) : 24-24.: Daftar Pustakaanon_31273229Belum ada peringkat
- 10 Cancer Symptoms Women Shouldnt IgnoreDokumen4 halaman10 Cancer Symptoms Women Shouldnt IgnoreRavindra DubeyBelum ada peringkat
- 1158 - Oncologic Imaging Urology (2017)Dokumen265 halaman1158 - Oncologic Imaging Urology (2017)Widya Surya AvantiBelum ada peringkat
- Poster ListDokumen8 halamanPoster ListAmalia Tri UtamiBelum ada peringkat
- EKSPRESI p40 DAN CK 5/6 UNTUK DIAGNOSIS SQUAMOUS CELL CARCINOMADokumen6 halamanEKSPRESI p40 DAN CK 5/6 UNTUK DIAGNOSIS SQUAMOUS CELL CARCINOMAEvrita Teny A.Belum ada peringkat
- Cytology II: Gynae and Non-Gynae CytologyDokumen126 halamanCytology II: Gynae and Non-Gynae Cytologybusiness onlyyouBelum ada peringkat
- Week 15 - ONCO COURSE TASK - Breast Cancer DetectionDokumen3 halamanWeek 15 - ONCO COURSE TASK - Breast Cancer DetectionGelo AlonzoBelum ada peringkat
- TOC Prof Chintamanis Comprehensive Book On SurgeryDokumen4 halamanTOC Prof Chintamanis Comprehensive Book On SurgeryKoustav ChakrabortyBelum ada peringkat
- NF 1 CriteriaDokumen2 halamanNF 1 CriteriaAlexandra E.Belum ada peringkat