Anda mungkin juga menyukai
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- Quantification of Dry Needling and Posture Effects On Myofascial Properties Using Ultrasound Scan PDFDokumen5 halamanQuantification of Dry Needling and Posture Effects On Myofascial Properties Using Ultrasound Scan PDFfisionovaisBelum ada peringkat
- Applied Kinesiology Collected PapersDokumen88 halamanApplied Kinesiology Collected PapersfisionovaisBelum ada peringkat
- Acupuncture, Trigger Points & Musculoskeletal PainDokumen362 halamanAcupuncture, Trigger Points & Musculoskeletal PainThezza Lion100% (2)
- Comparison of Relative Thickness of The Iliotibial Band Following Four Self-Stretching Exercises PDFDokumen8 halamanComparison of Relative Thickness of The Iliotibial Band Following Four Self-Stretching Exercises PDFfisionovaisBelum ada peringkat
- Reliability and Validity of Ultrasound Measurements of Muscle Fascicle Length and Pennation in Humans PDFDokumen10 halamanReliability and Validity of Ultrasound Measurements of Muscle Fascicle Length and Pennation in Humans PDFfisionovaisBelum ada peringkat
- Quantification of Dry Needling and Posture Effects On Myofascial Properties Using Ultrasound Scan PDFDokumen5 halamanQuantification of Dry Needling and Posture Effects On Myofascial Properties Using Ultrasound Scan PDFfisionovaisBelum ada peringkat
- Comparison of Relative Thickness of The Iliotibial Band Following Four Self-Stretching Exercises PDFDokumen8 halamanComparison of Relative Thickness of The Iliotibial Band Following Four Self-Stretching Exercises PDFfisionovaisBelum ada peringkat
- The Role of Passive Muscle Stiffness in Symptoms of Exercise-Induced Muscle DamageDokumen6 halamanThe Role of Passive Muscle Stiffness in Symptoms of Exercise-Induced Muscle DamagefisionovaisBelum ada peringkat
- Comparison of Relative Thickness of The Iliotibial Band Following Four Self-Stretching Exercises PDFDokumen8 halamanComparison of Relative Thickness of The Iliotibial Band Following Four Self-Stretching Exercises PDFfisionovaisBelum ada peringkat
- The Effects of SMR Using A Foam Roll or Roller Massager On Joint Range of Motion Muscle Recovery and PerformanceDokumen12 halamanThe Effects of SMR Using A Foam Roll or Roller Massager On Joint Range of Motion Muscle Recovery and PerformancefisionovaisBelum ada peringkat
- Ultrasound Guided Plantar Fascia ReleaseDokumen12 halamanUltrasound Guided Plantar Fascia ReleasefisionovaisBelum ada peringkat
- Anticancer: Prevenir e Vencer Usando Nossas Defesas NaturaisDokumen16 halamanAnticancer: Prevenir e Vencer Usando Nossas Defesas NaturaispatysalbrBelum ada peringkat
- An Acute Bout of Self-Myofascial Release Increases Range of Motion Without A Subsequent Decrease in Muscle Activation or Force PDFDokumen10 halamanAn Acute Bout of Self-Myofascial Release Increases Range of Motion Without A Subsequent Decrease in Muscle Activation or Force PDFfisionovaisBelum ada peringkat
- An Acute Bout of Self-Myofascial Release Increases Range of Motion Without A Subsequent Decrease in Muscle Activation or ForceDokumen5 halamanAn Acute Bout of Self-Myofascial Release Increases Range of Motion Without A Subsequent Decrease in Muscle Activation or ForcefisionovaisBelum ada peringkat
- Active Fascial Contractility - Fascia May Be Able To Contract in A Smooth Muscle-Like Manner and Thereby Influence Muscleskeletal DynamicsDokumen5 halamanActive Fascial Contractility - Fascia May Be Able To Contract in A Smooth Muscle-Like Manner and Thereby Influence Muscleskeletal DynamicsfisionovaisBelum ada peringkat
- Effects of Myofascial Release and Stretching Technique On ROM and Reaction TimeDokumen10 halamanEffects of Myofascial Release and Stretching Technique On ROM and Reaction TimefisionovaisBelum ada peringkat
- Do Exercises With The Foam Roller Have A Short-Term Impact On The Thoracolumbar FasciaDokumen37 halamanDo Exercises With The Foam Roller Have A Short-Term Impact On The Thoracolumbar FasciafisionovaisBelum ada peringkat
- Active Fascial Contractility - Fascia May Be Able To Contract in A Smooth Muscle-Like Manner and Thereby Influence Muscleskeletal DynamicsDokumen6 halamanActive Fascial Contractility - Fascia May Be Able To Contract in A Smooth Muscle-Like Manner and Thereby Influence Muscleskeletal DynamicsfisionovaisBelum ada peringkat
- Foam Rolling For Delayed-Onset Muscle Soreness and Recovery of Dynamic Performance MeasuresDokumen9 halamanFoam Rolling For Delayed-Onset Muscle Soreness and Recovery of Dynamic Performance MeasuresfisionovaisBelum ada peringkat
- Effects of Myofascial Release and Stretching Technique On ROM and Reaction Time PDFDokumen3 halamanEffects of Myofascial Release and Stretching Technique On ROM and Reaction Time PDFfisionovaisBelum ada peringkat
- Profiler Remote Quick Start 1.0 WebDokumen36 halamanProfiler Remote Quick Start 1.0 WebfisionovaisBelum ada peringkat
- Soundcraft Ui12Dokumen76 halamanSoundcraft Ui12fisionovaisBelum ada peringkat
- Studies of The Bowen TechniqueDokumen29 halamanStudies of The Bowen TechniquefisionovaisBelum ada peringkat
- Active Fascial Contractility - Fascia May Be Able To Contract in A Smooth Muscle-Like Manner and Thereby Influence Muscleskeletal Dynamics PDFDokumen5 halamanActive Fascial Contractility - Fascia May Be Able To Contract in A Smooth Muscle-Like Manner and Thereby Influence Muscleskeletal Dynamics PDFfisionovaisBelum ada peringkat
- Comparison of Relative Thickness of The Iliotibial Band Following Four Self-Stretching ExercisesDokumen8 halamanComparison of Relative Thickness of The Iliotibial Band Following Four Self-Stretching ExercisesfisionovaisBelum ada peringkat
- References Halliwick ResearchDokumen2 halamanReferences Halliwick ResearchfisionovaisBelum ada peringkat
- Anticancer: Prevenir e Vencer Usando Nossas Defesas NaturaisDokumen16 halamanAnticancer: Prevenir e Vencer Usando Nossas Defesas NaturaispatysalbrBelum ada peringkat
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (399)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (73)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (120)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- Dynamic Force AnalysisDokumen13 halamanDynamic Force AnalysisJakesBelum ada peringkat
- Illiquidity and Stock Returns - Cross-Section and Time-Series Effects - Yakov AmihudDokumen50 halamanIlliquidity and Stock Returns - Cross-Section and Time-Series Effects - Yakov AmihudKim PhượngBelum ada peringkat
- Acuvim II Profibus Modules Users Manual v1.10Dokumen36 halamanAcuvim II Profibus Modules Users Manual v1.10kamran719Belum ada peringkat
- Tech Specs - TC 5540 PDFDokumen2 halamanTech Specs - TC 5540 PDFziaarkiplanBelum ada peringkat
- The SphereDokumen9 halamanThe SpherePast Buanget100% (1)
- Cleats CatalogueDokumen73 halamanCleats Cataloguefire123123Belum ada peringkat
- T 096Dokumen3 halamanT 096abelBelum ada peringkat
- Synthesis of Glycerol Monooctadecanoate From Octadecanoic Acid and Glycerol. Influence of Solvent On The Catalytic Properties of Basic OxidesDokumen6 halamanSynthesis of Glycerol Monooctadecanoate From Octadecanoic Acid and Glycerol. Influence of Solvent On The Catalytic Properties of Basic OxidesAnonymous yNMZplPbVBelum ada peringkat
- GMS60CSDokumen6 halamanGMS60CSAustinBelum ada peringkat
- PassivityDokumen15 halamanPassivitySmarties AcademyBelum ada peringkat
- Fiber SyllabusDokumen1 halamanFiber SyllabusPaurav NayakBelum ada peringkat
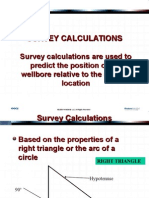
- 02 Survey Calculations - PpsDokumen96 halaman02 Survey Calculations - PpsLeo Ivan Aviles RicaldiBelum ada peringkat
- HANA OverviewDokumen69 halamanHANA OverviewSelva KumarBelum ada peringkat
- PDC NitDokumen6 halamanPDC NitrpshvjuBelum ada peringkat
- Engine Control System Circuit Diagram: Without This Message by Purchasing NovapdfDokumen3 halamanEngine Control System Circuit Diagram: Without This Message by Purchasing NovapdfJose Luis Gutierrez TamayoBelum ada peringkat
- GTG - TFA Belt DrivenDokumen2 halamanGTG - TFA Belt Drivensuan170Belum ada peringkat
- Nihonto Part IDokumen38 halamanNihonto Part IGergő VidaBelum ada peringkat
- EC 201 Network TheoryDokumen2 halamanEC 201 Network TheoryJoseph JohnBelum ada peringkat
- Geomorphic Evidences of Recent Tectonic Activity in The Forearc, Southern PeruDokumen11 halamanGeomorphic Evidences of Recent Tectonic Activity in The Forearc, Southern PeruVayolait BardBelum ada peringkat
- Mechanism of Muscle ContractionDokumen24 halamanMechanism of Muscle Contractionfisika100% (1)
- OIML R 137-1 & 2: Nternational EcommendationDokumen76 halamanOIML R 137-1 & 2: Nternational EcommendationAMY WEIBelum ada peringkat
- MIL-PRF-85704C Turbin CompressorDokumen31 halamanMIL-PRF-85704C Turbin CompressordesosanBelum ada peringkat
- CHMT 2009 Week 5 Coal PropertiesDokumen38 halamanCHMT 2009 Week 5 Coal PropertiesTiisetso MokwaneBelum ada peringkat
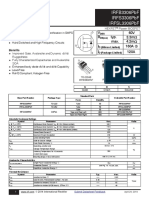
- Irfb3306Pbf Irfs3306Pbf Irfsl3306Pbf: V 60V R Typ. 3.3M: Max. 4.2M I 160A C I 120ADokumen12 halamanIrfb3306Pbf Irfs3306Pbf Irfsl3306Pbf: V 60V R Typ. 3.3M: Max. 4.2M I 160A C I 120ADirson Volmir WilligBelum ada peringkat
- HydrocarbonsDokumen5 halamanHydrocarbonsClaire Danes Tabamo DagalaBelum ada peringkat
- Guide-to-Proficiency-Testing-Australia 2019Dokumen29 halamanGuide-to-Proficiency-Testing-Australia 2019ffatikatuss100% (1)
- Alimak Alc - IIDokumen62 halamanAlimak Alc - IImoiburBelum ada peringkat
- 1 Tail & 2 Tail TestDokumen3 halaman1 Tail & 2 Tail TestNisha AggarwalBelum ada peringkat
- Simple Harmonic Oscillator: 1 HamiltonianDokumen10 halamanSimple Harmonic Oscillator: 1 HamiltonianAbdurrahman imamBelum ada peringkat
- Cópia de Teste Excel - Intermediário (5166) .XLS: BIM Technology For EngineersDokumen6 halamanCópia de Teste Excel - Intermediário (5166) .XLS: BIM Technology For EngineersFernanda AzevedoBelum ada peringkat